
Abstract
Background:
One of the anatomical variations in the maxillary sinus is the accessory ostium (AO). In the nasal cavity, the lateral wall’s vertical plane is parallel to the form of the AO, which is round or oval in appearance. During a nasal endoscopic examination, AO may be seen in contrast to the normal ostium of the maxillary sinus, which is hidden behind the uncinate process.
Methods:
The search for recent research articles on AO of the maxillary sinus was done with databases Scopus, PubMed, Medline, and Google Scholar. This review article discusses the prevalence, development, endoscopic examination, clinical significance, surgical importance, relationship with chronic sinusitis, and its management.
Results:
AO may interfere with ventilation and drainage of the maxillary sinus. Hence, it is important to evaluate the anatomical features of the AO for its relationship with sinus pathology. The development of maxillary sinusitis may be significantly impacted by the anatomical variance known as AO of the maxillary sinus. The middle meatus’s posterior nasal fontanelle is where AO is most frequently observed. The possible mechanism for the formation of AO is obstruction of the natural ostium of the maxillary sinus by sinusitis or due to anatomical and pathological factors in the middle meatus leading to rupture of membranous regions such as fontanelle.
Conclusion:
Clinicians must have adequate knowledge regarding the anatomical variations of the AO. It frequently appears in the fontanelle, the membranous portion of the middle meatus’ lateral nasal wall that is between the uncinate process and inferior meatus.
Introduction
Accessory ostium (AO) of the maxillary sinus is one of the important anatomical variations in the paranasal sinus.[1] It can be seen in different locations, shapes, and sizes. AO of the maxillary sinus is also called Giralde’s orifice.[1] AO might be unilateral, bilateral, solitary, or numerous.[2] In addition to the maxillary sinus’s natural ostium, it can also be present in the fontanelles that form the lateral wall of the nasal cavity.[3] The mucosal membrane, also known as the Schneiderian membrane, lines the bone cavity of the maxillary sinus, which has a pyramidal structure.[4] Through a natural ostium near the middle meatus, this mucosal membrane is joined to the nasal cavity. The natural ostium aids in the maxillary sinus’s drainage, ventilation, and maintenance of its physiological state.[5] The natural ostium is present at the superomedial aspect of the maxillary sinus, and obstruction of the natural ostium may lead to maxillary sinusitis.[6] The AO is an anatomical variation seen between the uncinate process and the inferior turbinate.[7] The uncinate process divides the fontanelle into the anterior and posterior fontanelles.[8] AO has been reported to be found in anterior fontanelle, posterior fontanelle, or rarely at the hiatus semilunaris.[9] As it runs parallel to the vertical plane of the lateral nasal wall, AO is seen as round or oval in form. AO can be easily visualized by endoscopic examination. This review article discusses on AO of the maxillary sinus and its impact on sinusitis.
Methods of Literature Search
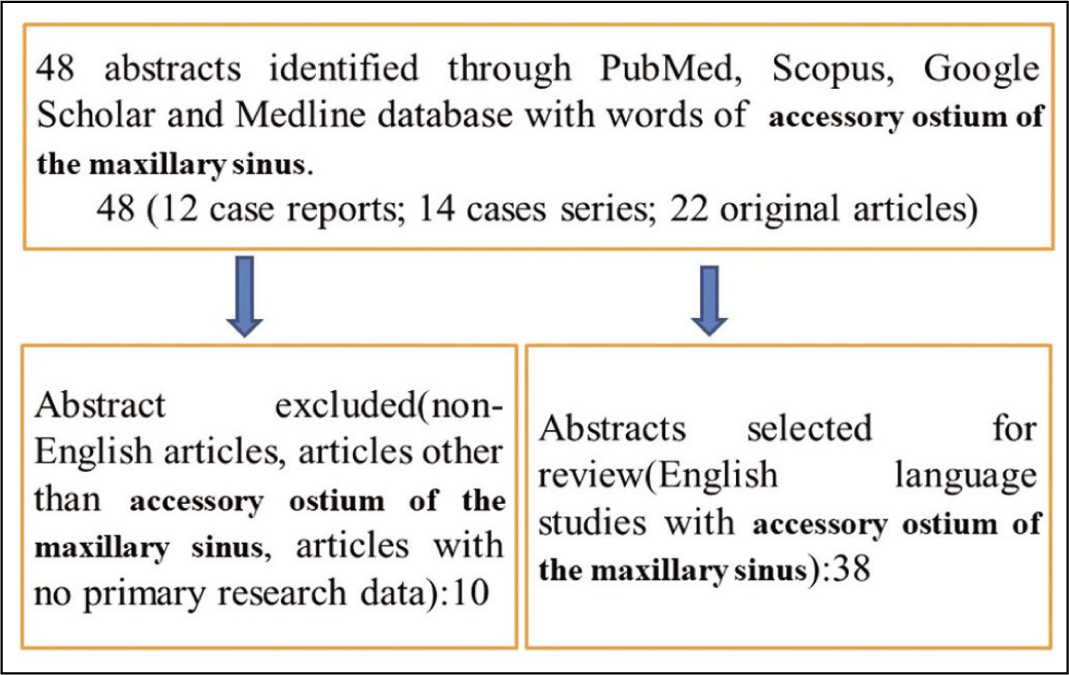
The search for recent research articles on AO of the maxillary sinus used several methodologies. The databases Scopus, PubMed, Medline, and Google Scholar were searched first online. A search strategy was created using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria for this review article. The citations were used to manually locate more research articles; however, our search strategy retrieved the abstracts of published works. The eligibility of randomized controlled trials, observational studies, comparative studies, case series, and case reports was assessed. A total of 48 articles such as 12 case reports, 14 case series, and 22 original articles were published [Figure 1]. This article focuses only on the AO of the maxillary sinus and its impact on sinusitis. A better knowledge of the AO of the maxillary sinus and its impact on sinonasal pathologies is provided by this review analysis. It will also catalyze further study and better awareness about the AO of the maxillary sinus.
Flowchart showing method of literature search
Prevalence of Accessory Ostium
There are variations in numbers of AO of the maxillary sinus.[10] In clinical settings, computed tomography (CT) and diagnostic nasal endoscopy are used to check the prevalence of AO of the maxillary sinus, whereas cadavers are used in anatomical studies to assess the condition. Clinical trials employing CT scan evaluation, cadaver analysis, and endoscopic evaluation have been used to study the prevalence of the AO, which has been shown to occur anywhere from 0% to 47.2%.[11] One study indicated a 10% incidence of AO by endoscopic investigation; however, no AO was detected in cadaveric evaluation.[12] In a CT scan study, Serindere et al. similarly found a prevalence of the AO of 10.5%.[13] Approximately 30% of people with chronic maxillary sinusitis and 10%–20% of healthy individuals have AO.[14] In one study of the Jordanian population, 29.5% of the research cohort’s paranasal CT scans showed the presence of AO.[15] The presence of AO causes a two-fold rise in the frequency of maxillary sinusitis.[7] In 1993, Rice and Scheaffer coined the term “AO of the maxillary sinus” to describe any openings on the lateral nasal wall other than a single primary ostium.[16] The size of the AO ranges from 1 to 10 mm.[17]
Development
AO is thought to cause sinus infections by damaging the fontanelles.[3] However, AO is found easily in diagnostic nasal endoscopy as present posteriorly. It is still questionable whether the AO is an acquired or congenital abnormality brought on by maxillary sinusitis.[18] A study supports acquired cause of AO where maxillary sinusitis results in perforations of the fontanelle.[18] This study used a rabbit model to demonstrate how AO might develop after severe maxillary sinusitis. Another study documents origin of AO due to chronic rhinosinusitis following extensive endoscopic procedure.[19] Severe maxillary sinusitis can block the natural ostium, and the absence of bony structures makes the fontanelle less resistant and more likely to perforate.[19] The fontanelle is a region of the middle meatus that can be seen below the uncinate process and above the inferior turbinate. Fontanelle is lined on both sides by mucous membranes: the nasal mucous membrane on the medial side and the mucosa of the maxillary sinus on the lateral side. There are anterior and posterior nasal fontanelles, depending on where they are located in the uncinate process.[20] The natural ostium of the maxillary sinus is located on the highest portion of the medial wall of the maxillary sinus and opens into the small ethmoidal infundibulum rather than the nasal cavity, where it might become infected or swollen and further impede sinus outflow.[21] Whether the AO is congenital or acquired is unclear. Some authors hypothesized that AO frequently follows a bout of acute maxillary sinusitis.[16]
Endoscopic Examination
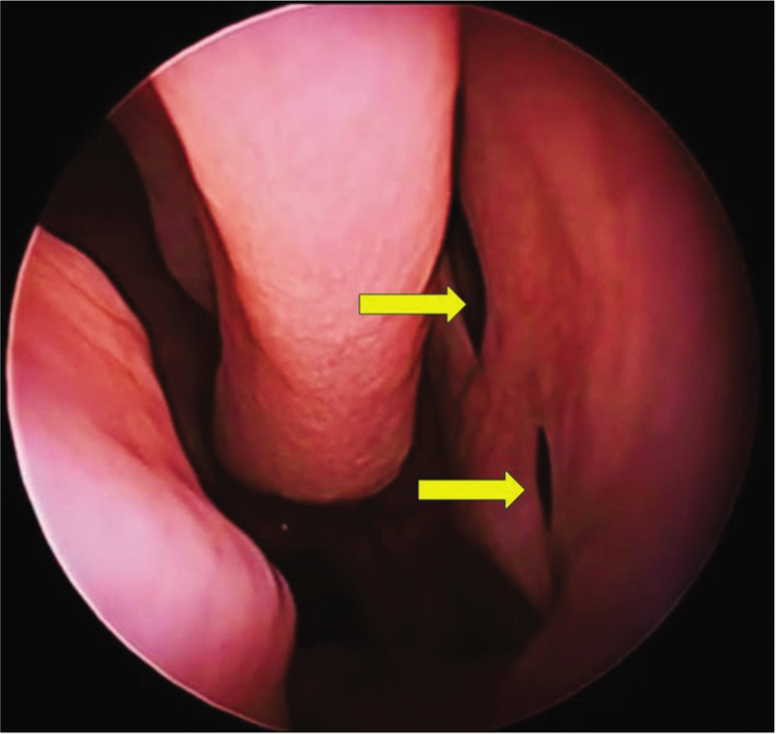
Nasal endoscopy is currently being utilized for diagnosis and surgical management of sinonasal pathologies. Since secretions constantly attempt to exit by the natural ostia, direct observation of the mucociliary clearance patterns has revealed that there are distinct channels in the paranasal sinuses. The oval-shaped natural ostium of the maxillary sinus is located anteriorly, and during a nasal endoscopic assessment, it is not discernible.[22] The maxillary sinus’s natural ostium is located at the highest point on its medial wall, making it poorly positioned for free drainage. In addition, it typically opens into the tiny ethmoidal infundibulum rather than the nasal cavity, and its inflammation may prevent drainage.[23] Along with the maxillary sinus’ natural ostium, which connects the sinus to the middle meatus, endoscopic in vivo examination frequently identifies the existence of AO in the maxillary fontanelle. Between inferior turbinate and uncinate process, there is a membranous region on the lateral nasal wall, covered only by the mucoperiosteum. This area is called a fontanelle, and the ethmoid process of the inferior concha divides the membranous area into two components such as anterior and posterior fontanelles.[24] The natural ostium of the maxillary sinus is commonly found on the anterior part of the posterior fontanelle. AO is most commonly seen at the posterior fontanelle.[25] The natural ostium of the maxillary sinus lies deep in the infundibulum and is obscured from view by the uncinate process; therefore, any ostium discovered at the middle meatus during endoscopic examination is usually an AO.[6,25] According to one study, the AO is clearly detectable during a normal endoscopic nasal examination since it is located on the posterior side and has an oval form.[26] AO connects to the lateral nasal wall and is 5–10 mm superior to the attachment of the inferior turbinate. The maxillary sinus can be characterized as triangular in adults. The lateral nasal wall’s vertical plane is parallel to the form of the AO, which is circular or oval. In comparison to the natural ostium of the maxillary sinus, AO [Figure 2] can be visualized during middle meatus examination by nasal endoscopy and AO can be found in unilateral or bilateral, single, or multiple [Figure 2]. Different studies have shown different incidences and locations of AO of the maxillary sinus [Table 1].
Diagnostic endoscopic examination of the nasal cavity showing two accessory ostia (yellow arrow)
Incidence and location of accessory ostium of the maxillary sinus
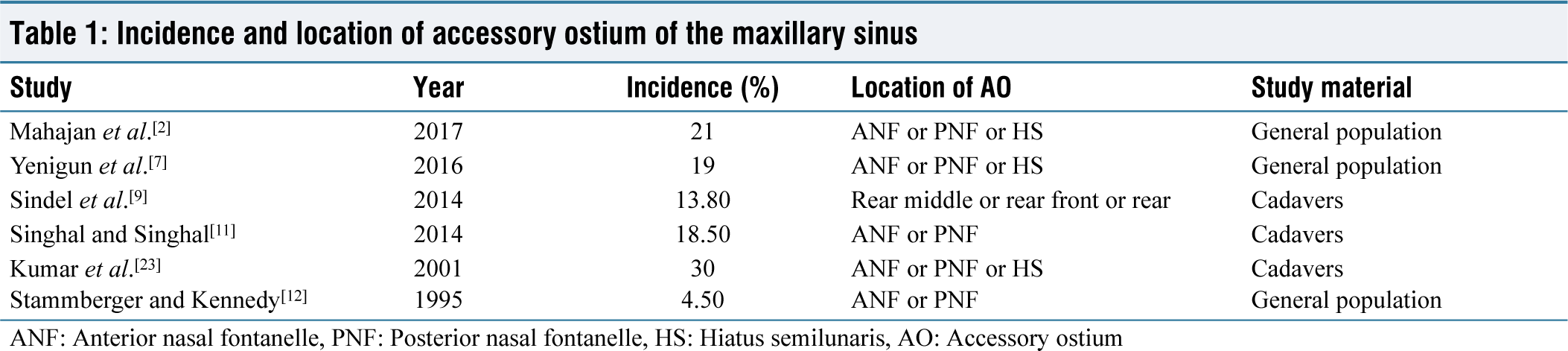
ANF: Anterior nasal fontanelle, PNF: Posterior nasal fontanelle, HS: Hiatus semilunaris, AO: Accessory ostium
ClinicalSignificance of Accessory Ostium
As per a study, having an AO was linked to an increased risk of mucous retention cysts by three times, mucosal thickening by two times, and sinusitis by two times.[7] An AO is related to mucosal thickness, maxillary sinusitis, and natural ostium blockage more so than individuals who do not have an AO, but not with a mucous retention cyst.[27] Endoscopic sinus surgery must have knowledge regarding the anatomy of the maxillary sinus, natural ostium, and AO in relation to the orbital floor, ethmoid infundibulum, and nasolacrimal duct. Clinically, endoscopic sinus surgeons may employ the AO to irrigate the maxillary sinus in certain circumstances. In addition to ostia, the fontanelle may be used to create a different route that might restore ventilation and drainage while treating maxillary sinusitis.[28] Both maxillary sinusitis and ethmoidal sinusitis are much more common in men. The existence of an AO is linked to both maxillary and ethmoidal sinusitis in addition to the male sex. Maxillary and ethmoidal sinusitis are frequently coexist; however, the exact reason is not known. Animal research has demonstrated the connection between the AO and acute sinusitis.[20]
Surgical Importance of Accessory Ostium
If the natural ostium of the maxillary sinus is discovered to be patent after performing uncinectomy, then middle meatal antrostomy is usually not done during endoscopic sinus surgery. If AO is present, it must be attached to or united to the natural maxillary sinus ostium. A backbiting forceps that is put into the AO and extends anteriorly into the natural ostium can be used to accomplish this. If the surgeon does not locate the natural ostium and connect it to AO, this will cause mucus to circulate between the maxillary sinus and nasal cavity, which will prolong the illness. As a result, functional endoscopic sinus surgery is unsuccessful, leading to the creation of a pseudo middle meatal antrostomy. Patients who have functional endoscopic sinus surgery and then visit a rhinology clinic with recurrent sinusitis should have a thorough endoscopic nasal evaluation.[29] In an adult person, the maxillary sinus is triangular, measuring 25 mm along the anterior limb of its base, 34 mm in depth, and 33 mm in height.[30] A CT scan of the nose and paranasal sinuses can be performed after an antibiotic course to check for the existence of a distinct natural ostium, an AO, or a posterior fontanelle ostium. The patient should be sent for a second operation where two ostia must be linked if distinct ostia are discovered. The natural ostium of the maxillary sinus should be sliced forward with a backbiter after being introduced into the AO. After creating this tissue edge, the extra tissue may be removed with a microdebrider. To prevent orbital damage and obtain the best outcomes, it is essential to distinguish the natural ostium of the maxillary sinus from the AO in the middle meatus while doing endoscopic sinus surgery.
Chronic Sinusitis and Accessory Ostium
One of the most common diseases that send a patient to the otorhinolaryngology clinic is chronic maxillary sinusitis. Despite receiving appropriate medical and surgical therapy, chronic sinusitis significantly increases morbidity. Anatomical differences in the nasal cavity, bacterial infection, allergies, and other factors all contribute to the complex etiology of chronic maxillary sinusitis.[31] AO is thought to be a significant contributor to the pathophysiology of chronic maxillary sinusitis.[32] Due to the recycling of mucus between the natural ostium and AO of the maxillary sinus, AO hinders mucociliary clearance of the sinus, which results in chronic maxillary sinusitis.[21] Inflammation of the mucosal lining of the nasal cavity and paranasal sinuses is a feature of the sinonasal disease chronic rhinosinusitis.[33] Patients of chronic maxillary sinusitis with AO often complain of nasal block and postnasal drip. Endoscopic assessment of the nasal cavity may show mucopurulent secretions from the middle meatus, and AO is visible. It is affecting around 16.3% of the adult population.[33] Chronic rhinosinusitis is mostly diagnosed based on clinical symptoms, which are then validated by a diagnostic nasal endoscopy and CT scan of the nasal cavity and paranasal sinus. The only method of mucous clearance in the maxillary sinus is mucociliary action, which occurs against gravity. The natural ostium of the maxillary sinus is targeted by cilia in the maxillary sinus. The secretions are not transferred by an AO, despite the fact that it is situated in a more favorable gravitational location than one might think.[34]
Management
An AO is a frequent middle meatus anatomical variation that might have a role in the development of chronic rhinosinusitis.[35] The paranasal sinus CT scans’ axial and coronal cuts assess the AO.[36] The paranasal sinuses are close to important tissues such as the orbits, internal carotid arteries, optic nerve, and base of the skull. Few anatomical variations increase the risk of injury to the vital structures during endoscopic sinus surgery. Diagnostic criteria of rhinosinusitis include major and minor criteria. Major criteria have facial pressure/pain, nasal obstruction, anosmia/hyposmia, nasal discharge/postnasal drip, and purulence on examination. The minor criteria for rhinosinusitis include headache, fever, dental pain, halitosis, fatigue, cough, and ear pain/fullness/pressure.[37] Diagnosis of chronic rhinosinusitis is made if two major factors or one major and two minor factors are present.[37] Patients of recurrent sinusitis need adequate endoscopic evaluation of the nasal cavity. CT scan is recognized as the gold standard method for identifying paranasal sinus disorders and different anatomical variations. A CT scan of the nose and paranasal sinuses should be performed after a period of medicinal therapy, and the results should be carefully scrutinized for the presence of a distinct natural ostium, an AO, or a posterior fontanelle ostium. In the event that it is discovered, the patient must be taken in for a second operation during which the two ostia should be joined. The natural ostium of the maxillary sinus should be sliced forward with a backbiting forceps after being introduced into AO. After creating this tissue edge, the extra soft tissue may be removed with a microdebrider. Medical treatment is initially tried for chronic rhinosinusitis. If a patient is planned for functional endoscopic sinus surgery, a middle meatal antrostomy is always required, if the natural ostium of the maxillary sinus is seen patent after the procedure of the uncinectomy. However, AO has to be joined to the natural ostium of the maxillary sinus. It is done by introducing a backbiting forceps into AO and extending it anteriorly into the natural ostium. Failure to see the natural ostium, and so connecting it to the AO, will lead to recirculation of mucous between the nasal cavity and maxillary sinus, leading to persistent infection.
Conclusion
For performing functional endoscopic sinus surgery and to understand chronic rhinosinusitis, an endoscopic sinus surgeon has to have a good grasp of the anatomy of the AO of the maxillary sinus. Chronic maxillary sinusitis and the presence of AO are significantly correlated. The presence of AO results in the recirculation of the mucus from the maxillary sinus to the nasal cavity through the natural ostium and back to the maxillary sinus through AO. The ability to combine the separate apertures into a single, sizable antrostomy in order to get the normal ventilation of the maxillary sinus and mucociliary function is a skill that endoscopic sinus surgeons should be well versed.
Footnotes
Acknowledgements
Author is thankful to Prof. (Dr.) Ashutosh Biswas, Executive Director, AIIMS, Bhubaneswar for his encouragement to write this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
Not applicable. This is a review article.
CRediT Author Statement
Dr. Santosh Kumar Swain: Concept, literature search, data acquisition, manuscript preparation, manuscript editing, and approval of the version to be published.
Data Availability
Data are available in a public, open access repository.
Use of Artificial Intelligence
Not applicable.