
Abstract
Introduction:
Primary hydatid cyst of the spinal cord is exceedingly rare. Diagnosis at the early stages is difficult as they may be asymptomatic or have mild vague pain. Patients typically present when there are features of cord/root compression. Magnetic resonance imaging (MRI) stands as the primary investigative modality, but even then, preoperative diagnosis might not always be possible as it may resemble other pathological conditions.
Methods:
This was a case report of a single case with evidence-based discussion. Informed consent was obtained.
Case Report:
We present a 62-year-old female patient with progressive paraparesis and numbness of bilateral lower limbs. MRI was suggestive of a tubercular pleurospinal lesion at the D9-D10 level. However, intraoperatively, it was identified to be a rare case of primary pleurospinal (thoracic) hydatid cyst. The patient was managed with complete surgical removal of all the cysts and antihelminthic drug therapy with no evidence of recurrence at the 2-year follow-up.
Conclusion:
Radiological diagnosis might not be accurate and hydatidosis must be kept in mind to avoid intraoperative confusion. Timely diagnosis, appropriate surgical planning, and comprehensive follow-up are crucial for achieving optimal outcomes.
Introduction
Hydatid cyst is caused by the cestode Echinococcus granulosus. The incidence of bony hydatid lesions ranges from 0.5% to 3% of hydatidosis with half of them occurring in the vertebral system.[1,2] The vertebral involvement is commonly a direct extension from an adjoining tissue/organ. Direct primary involvement of vertebral bone is rare, and contiguous intrathoracic involvement is even rarer.[2] Even with the advent of advanced magnetic resonance imaging (MRI) techniques, it might sometimes be difficult to arrive at a preoperative diagnosis as it may resemble other infectious conditions.[3]
Here, we present the case of a primary pleurospinal (thoracic) hydatid cyst with epidural extension causing spinal cord compression and paraparesis.
Case Report
Case presentation
A 62-year-old female patient presented to our hospital with a three-month history of progressive weakness, numbness of bilateral lower limbs, and difficulty in walking. She also complained of vague back pain for the past year. Neurological examination revealed paraparesis, with reduced muscle strength (MRC grade 3/5 bilaterally) and impaired sensation below the D8 level.
Diagnosis
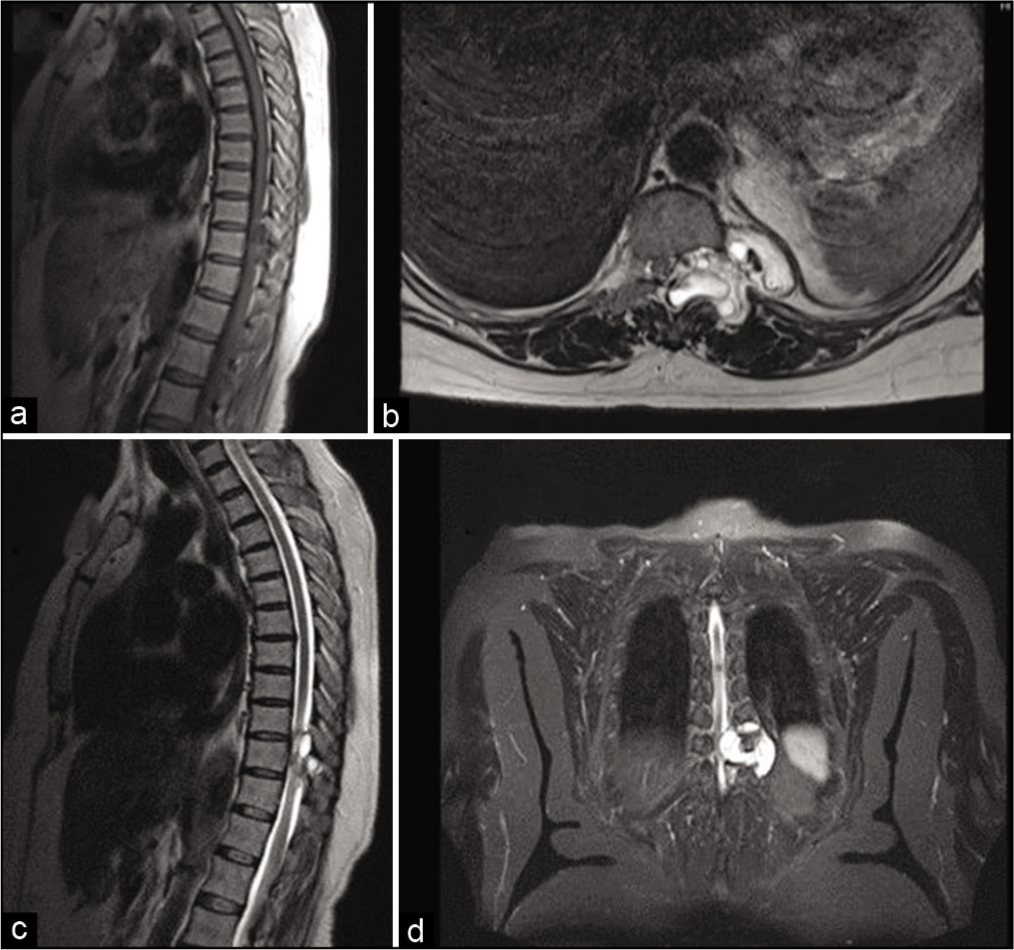
MRI imaging showed the presence of a T1 hypo, T2 hyperintense dumbbell-shaped pleurospinal multicystic lesion located at the D9-D10 vertebral level with spinal cord compression [Figure 1]. The radiologist provided a differential diagnosis of tuberculous/nonspecific abscess.
(a) T1 sagittal section showing heterogeneously hypointense lesion in the posterior aspect of D9-D10 vertebra, (b-d) T2-weighted images showing heterogeneously hyperintense dumbbell-shaped lesion with surrounding bony erosion and cord compression
Intervention
After a preanesthetic checkup, the patient was taken up for surgery. The patient was placed in a prone position under general anesthesia. A posterior midline incision was made extending from D8 to D11. Bilateral D9-D10 decompressive laminectomy relieved the pressure on the cord and the cord regained pulsatility. On the left lateral aspect, whitish cysts were seen extending along the root and exiting via the intervertebral foramina which was widened. A midline posterior durotomy was made and no intradural extension cysts were present. To gain better access and ensure complete removal, an extension into a left posterolateral D10 thoracotomy was made [Figure 2].
(a) Intraoperative imaging with T-shaped incision – midline vertical plus left posterolateral thoracotomy. The Dura (white arrow) was opened to ensure no intradural extension. Right lateral thoracotomy for extirpation of pleural cavity cysts – Lung parenchyma appeared normal. D9-D10 intercostal space (black arrow), (b) Excised hydatid cysts of varying sizes
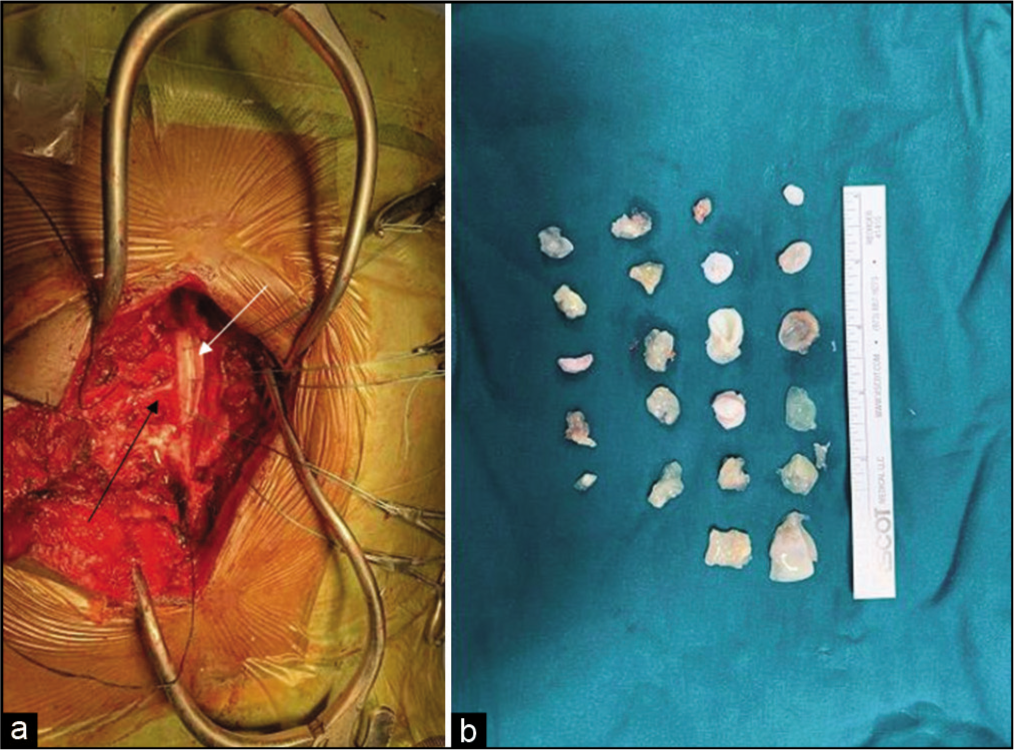
Careful dissection was carried out to identify the cysts, which were adherent to the spinal cord and surrounding tissues. Due to dense adhesions to the surrounding tissue, some cysts ruptured when attempting removal [Figure 2]. Contamination was kept to a minimum by continuous suction and preemptively covering the lung and surrounding tissue with cottonoids. After ensuring complete removal, the cystic cavity was thoroughly irrigated with 30% hypertonic saline. An intercostal drain was placed. The patient was extubated postoperatively, the ICD was removed on day two, and the patient was discharged on day four postoperatively.
Outcome and follow-up
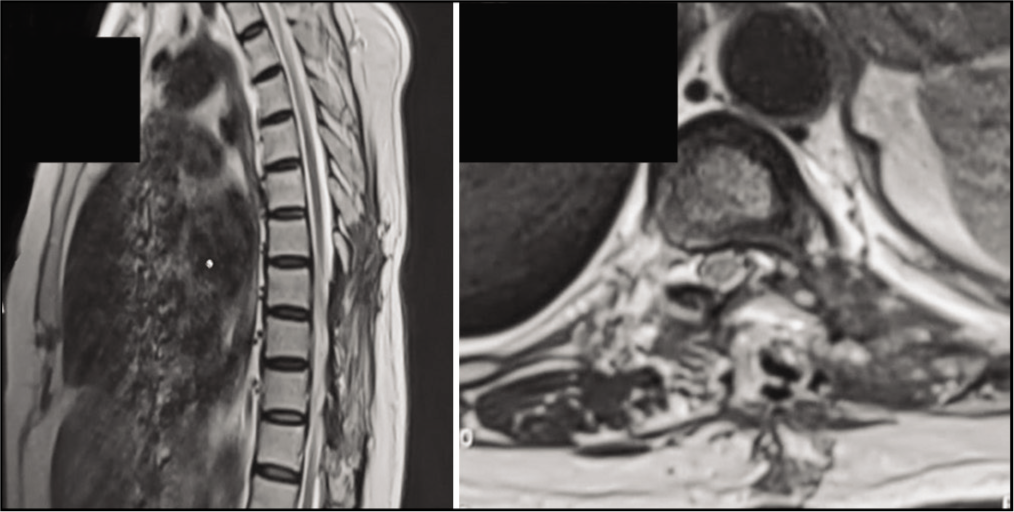
Postoperatively, the patient showed immediate improvement in motor strength and sensation. Histopathological examination confirmed the diagnosis of a hydatid cyst. The patient was prescribed albendazole for three months postoperatively. As of the review done at one-year postoperatively, the patient had no neurological deficit, and during the 24-month follow-up period, the patient remained asymptomatic, with no evidence of recurrence [Figure 3].[4]
Postoperative image at 2 years with postoperative changes and no recurrence
Discussion
Spinal echinococcosis was first reported in 1807.[5] The condition is endemic in countries with large sheep-rearing populations.[1] Humans acquire the infection via infected dogs or by consumption of contaminated food/water.[2] The cysts are carried through the bloodstream from the intestinal wall to various organs. Liver is the most common site (60-70%), followed by the lungs (10-15%). Spinal involvement is seen in 0.2%–1%.[6]
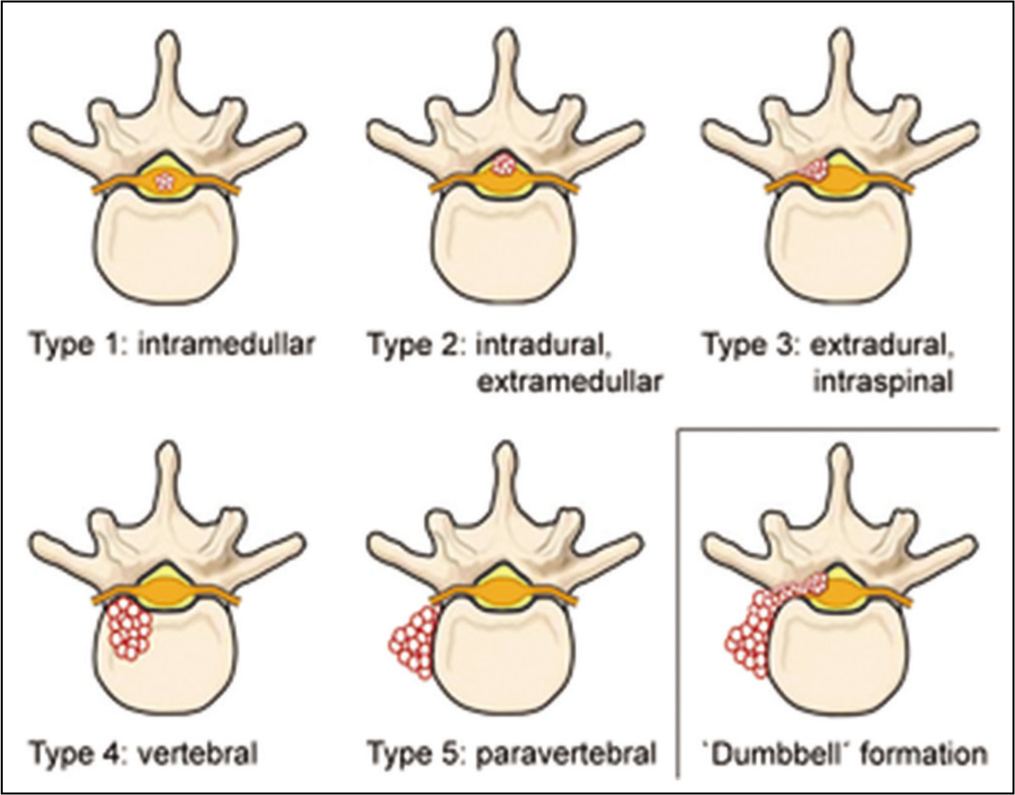
The occurrence of vertebral hydatidosis is most prevalent in individuals aged between 30 and 50 years but can occur in children as well.[5] Involvement of the vertebra in hydatid disease typically occurs as a result of direct extension from the abdomen, chest cavity, or pelvis. Among the various regions of the spine, the most commonly affected are the thoracic spine (52%), followed by the lumbar spine (37%), cervical spine (5.5%), and sacral spine (5.5%).[7-9] Braithwaite and Lees classified spinal hydatid disease based on radio-anatomic characteristics.[4,9] Another classification method is based on the route of infection, distinguishing between primary and secondary spinal hydatid disease[7] [Figure 4]. The vertebral body type is often seen as a dumbbell-shaped lesion as was present in our patient.
(Reproduced – source added): Classification of spinal cystic echinococcosis (CE) according to the Dew/Braithwaite and Lees classification (type 1–5) and ‘dumbbell’ formation.[4] Licensing: https://creativecommons.Org/licenses/by/4.0 /(unchanged)
Our patient presented with vague pain for the past year and progressive paraparesis for three months. The duration and characteristics of clinical symptoms can vary. Typical manifestations often include back pain, paraparesis (weakness in the lower limbs), radiculopathy (nerve root pain), sensory disturbances, deformity, and involvement of the sphincter muscles. Paraplegia, which refers to complete paralysis of the lower limbs, is observed in approximately 26% of cases.[10-12]
In our case, the preoperative diagnosis was difficult as the lesion closely resembled a tuberculous/nonspecific abscess, a diagnosis that has to be considered in an endemic country like India. The lesion was completely extrapulmonary and involved the vertebral pedicle, facet joints, and the body. MRI may not be conclusive in all cases and some other differential diagnoses mentioned in the literature that can closely resemble hydatidosis are arachnoid cyst, tubercular spondylitis, and chronic osteomyelitis.[13,14]
Surgical intervention remains the primary treatment modality, aiming for complete cyst removal when preserving neurological function. In this case, the posterior midline approach with an extension into a left lateral thoracotomy provided adequate exposure for complete cyst removal, resulting in a successful outcome. In a similar series by Prabhakar et al., wide decompressive laminectomy and debridement was recommended and in some patients, due to extensive vertebral body erosion, anterior decompression and spinal fusion was recommended as a second stage.[15] In our patient, the bony erosion was not severe enough to necessitate fusion and the decompression and excision alone was sufficient.
Thorough irrigation of the cavity with cysticidal agent (hypertonic saline 30%, cetrimide, and 70%–95% ethanol) is suggested for reducing recurrence.[16,17] In our patient, 30% hypertonic saline irrigation was utilized. In the postoperative period, oral albendazole was administered for 3 months. Our literature search did not provide any consensus as to the duration of therapy, which varied from study to study from 4 weeks to 1 year.[15,18]
Conclusion
This case report highlights the successful management of a rare primary pleural and spinal hydatid cyst located at the D9-10 level, leading to paraparesis. MRI findings are not pathognomonic and may simulate similar pathological conditions. Surgical intervention utilizing a posterior midline approach with an extension into a left lateral thoracotomy resulted in complete cyst removal and excellent postoperative recovery. Timely diagnosis, appropriate surgical planning, and comprehensive follow-up are crucial for achieving optimal outcomes in cases of pleurospinal hydatid cysts.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The authors certify that he has obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Informed Consent
Patient consent has been obtained for publication in accordance with the journal guidelines and shall be furnished on request.
CRediT Author Statement
Priyadharshan K.P. – Concept and design, draft and revision of intellectual content, literature search, discussion and interpretation, manuscript preparation, and review. Kodeeswaran M. – Concept, revision of draft, final approval of version to be published, and manuscript review. Meghena Mathew – Concept and design of study. Ashwin Kumar Mani – Concept and design of study. Haritha Reddy Vakamala – Concept and design, original draft, discussion, and interpretation. Jayamoorthy T. – Concept and design of study.
Data Availability
Data available - open access.
Use of Artificial Intelligence
Artificial intelligence was not used.