
Abstract
Background:
Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) are widely used medications for treating essential hypertension, but there is limited research comparing their effectiveness. To address this gap, a recent meta-analysis was conducted to evaluate and compare the efficacy of these two drug classes in decreasing blood pressure (BP) among patients with essential hypertension.
Objective:
Evaluating of comparative efficacy of ACEIs versus ARBs in reducing BP in essential hypertension.
Methods:
An extensive literature search for randomized controlled trials (RCTs) following PRISMA guidelines (2020), with inclusion criteria of age ≥18 years, with either gender and diagnosed of essential hypertension and receiving ACEIs or ARBs for at least 4 weeks. Patients with secondary hypertension, malignancy, symptomatic cardiovascular system (CVS) disease, hepatic involvement, and studies with Fimasartan and Allisartan were excluded. For this study, all RCTs that reported changes in mean systolic BP (SBP) and diastolic BP (DBP) before and after administration of the drugs were gathered. Standardized mean difference (SMD) was calculated using RevMan 5.4.1 software. The significance level was set at a P < 0.05.
Results:
A total of 28 RCTs (n = 9778) were included in our study. Both groups reduce SBP and DBP from the baseline values. Pooled analyses of studies showed that ARBs were superior to ACEIs with SMD = 0.179 in the random-effect model, 95% confidence interval (CI) (0.0975–0.260), P < 0.001, and in the fixed-effect model, SMD = 0.207, 95% CI (0.167–0.248), P < 0.001 in the mean reduction of SBP. Furthermore, for a mean reduction in DBP, ARBs were superior to ACEIs with SMD = 0.329 in the random-effect model, 95% CI (0.161–0.496), P < 0.001, and in the fixed-effect model, SMD = 0.317, 95% CI (0.276–0.357), P < 0.001. Our study included 28 RCTs with a combined sample size of 9778 participants. Both ACEIs and ARBs were found to effectively reduce SBP and DBP from their baseline values. However, our pooled analysis of the studies revealed that ARBs were more effective than ACEIs in reducing mean SBP, with an SMD of 0.179 in the random-effect model and 0.207 in the fixed-effect model. The 95% CIs for these estimates were (0.0975–0.260) and (0.167–0.248), respectively, with P < 0.001. Similarly, for a mean reduction in DBP, ARBs were found to be superior to ACEIs with a SMD of 0.329 in the random-effect model and 0.317 in the fixed-effect model, with 95% CIs of (0.161–0.496) and (0.276–0.357), respectively, and a P < 0.001.
Conclusion:
ARBs are more efficacious as compared to ACEIs in essential hypertension.
Keywords
Introduction
Hypertension is a major contributor to the global disease burden, with significant health implications. The World Health Organization reports that one out of every four men and one out of every five women worldwide suffer from hypertension.[1] Elevated blood pressure (BP) affects over one billion people and is responsible for an estimated 9.4 million deaths yearly.
Hypertension is a significant risk factor for various health issues, including myocardial infarction, congestive heart failure, stroke, end-stage renal disease, and sudden death. Consistently lowering BP is a well-established strategy for preventing end-organ damage and related health complications.[2] Despite the recognized importance of controlling BP in hypertensive patients, only one out of every five patients achieves adequate BP control to a level of ≤140/90 mmHg. Around 80%–95% of patients are diagnosed with primary or “essential” hypertension.[1] An increase in BP with no identifiable cause is referred to as essential hypertension. This condition raises the risk of cerebral, cardiac, and renal events.[3]
According to the Joint National Committee guidelines, the first-line treatment for hypertension should involve the use of a thiazide diuretic, calcium channel blocker, angiotensin-converting enzyme (ACE) inhibitor, or angiotensin receptor blocker (ARB).[4]
ACE inhibitors (ACEIs) work by inhibiting the peptidyl-dipeptidase enzyme that converts angiotensin I to angiotensin II. In contrast, ARBs selectively prevent angiotensin II from binding to angiotensin II receptor type 1.
ACEIs carry a higher risk of side effects than ARBs, mainly due to their tendency to increase the levels of bradykinin in circulation and tissues. This increase can result in the occurrence of cough and angioedema.[5]
The aim of the present study is to conduct an updated systematic review and meta-analysis that compares the effectiveness of ACEIs and ARBs in reducing BP.
Objective
Evaluating of comparative efficacy of ACEIs versus ARBs in reducing BP in essential hypertension.
Methods
This is a meta-analysis to compare the efficacy of two different drug classes used in essential hypertension.
Step 1: Identification and literature search
To identify relevant original randomized controlled trials (RCTs), we conducted a comprehensive search of articles in various databases, including PubMed, Medline, EBSCOhost, Scopus, Cochrane Library, Google Scholar, Alt HealthWatch, CINAHL Consumer Health Complete, and Health Source: Nursing/Academic Edition, without language restrictions. In addition, we screened the reference lists of all retrieved articles to identify any other relevant publications. The search was conducted using the appropriate search strings and MESH terms: “ACEIs such as Zofenopril, Enalapril, Lisinopril, Ramipril, Captopril, Imidapril, Perindopril, Fosinopril, Quinapril, Benazepril, Moexipril, Trandolapril, versus ARBs such as Irbesartan, Losartan, Candesartan, Valsartan, Olmesartan, Telmisartan, Azilsartan, Eprosartan, Saprisartan” OR “Essential Hypertension treatment AND randomized controlled trial.”
Step 2: Criteria for selection of studies
All study-related RCTs using either:
A suitable technique for concealing allocation (such as sealed opaque envelopes) can be employed Studies that were double blind, single blind, or unblinded.
We incorporated RCTs that examined the effects of ACEIs and ARBs on BP in individuals with essential hypertension. Our inclusion criteria encompassed RCTs conducted in adults with essential hypertension, specifically focusing on the comparison between ACEIs and ARBs. We included RCTs that adhered to the guidelines outlined in CONSORT (2018)[6] and PRISMA (2020).[7]
Step 3: Randomized controlled trials enrolment criteria
Inclusion criteria
Patients of either gender
Patients with age above 18
Patients diagnosed with or suffering from essential hypertension
We enrolled patients diagnosed with essential hypertension who had been receiving either ACEIs or ARBs as monotherapy for a minimum duration of 4 weeks. The patients had their systolic and diastolic BP (DBP) measurements taken while seated in the office/clinic.
Exclusion criteria
Secondary hypertension
Malignancy
Symptomatic CVS disease
Hepatic involvement
We excluded studies that utilized Fimasartan or Allisartan as treatments for hypertension, as well as studies with unpublished results. Since Fimasartan was approved for use solely in South Korea, and Allisartan was approved only in China at the time of the study’s initiation, it was deemed appropriate to exclude studies using these medications, given their limited usage and global availability.
Step 4: Type of intervention
Monotherapy ACEI versus ARB in essential hypertension.
Step 5: Clinical outcome measure
Primary outcome
Treatment with either ARBs or ACEIs resulted in a reduction in the mean systolic and diastolic blood pressure among individuals with essential hypertension.
Step 6: Data extraction
Mean reductions in systolic BP (SBP) and DBP from individual RCTs were extracted. The data extraction followed the standard reporting guidelines of QUOROM (2000). Two independent researchers verified the data, and any discrepancies were resolved through consensus.
The subsequent step involved the comparison of these extracted data. For each included study, various aspects were collected, including study characteristics (such as the first author’s name, title, publication year, and journal), duration of the study, drugs and doses administered in the treatment groups, and any additional treatments utilized. Furthermore, patient characteristics (such as the number of participants in each treatment group, age, gender, race, smoking and alcohol habits, history of previous antihypertensive treatment, and presence of comorbidities) were recorded. In addition, predefined outcomes related to BP levels were also extracted.
If a study did not report the standard deviation (SD) but instead provided the standard error of the mean or confidence interval (CI) as a measure of variability, the SD was computed using the RevMan→ version 5.4.1 software. In addition, if the reduction in BP from baseline or its SD was not explicitly mentioned in the text but presented in a graph, the values were extracted from the graph. In cases where it was not feasible to derive the BP reduction or its corresponding SD from the available data, the final SBP and DBP values, along with their corresponding SDs, were utilized.
Step 7: Nullification of bias
The authors made sure to only include studies that met the inclusion and exclusion criteria and had no conflicts of interest. In addition, they ensured that the allocation of ACEI and ARB groups was randomized appropriately.
Step 8: Measures of treatment effect
The authors employed a fixed and random-effect model to directly compare the effectiveness of ACEIs and ARBs and used data from published studies that compared these two antihypertensive treatments to extract the mean reductions in SBP and DBP for each drug in the individual RCTs. Based on these differences, they conducted a meta-analysis to calculate the standardized mean deviation (SMD) for each RCT, with statistical significance set at P < 0.05.
Step 9: Summary measures
Both fixed and random-effect models were employed to directly compare the active drugs. The primary summary measure was determined using standardized mean differences (SMDs) with a 95% CI and represented by funnel and forest plots. Analysis was conducted using RevMan→ version 5.4.1. A paired t-test was conducted to assess the significance of differences in adverse effects between the drugs, with a P < 0.05 considered statistically significant. The primary analysis of the study results was based on an intention-to-treat approach. For data synthesis and traditional meta-analysis, the researchers utilized RevMan version 5.4.1 from the Nordic Cochrane Center in Copenhagen, Denmark. Heterogeneity was assessed using both the Chi-square test, where a P < 0.10 indicated significant heterogeneity, and the I2 statistic, where a value exceeding 50% indicated moderate heterogeneity. The risk of bias across studies was visually assessed using funnel plots, and statistically, the risk was estimated using Egger’s test. It is important to note that funnel plot asymmetry tests were conducted only when there were at least 10 studies included in the meta-analysis. Due to the expected heterogeneity between the studies, the inverse variance method and random-effects model were employed for the two quantitative variables, SBP and DBP.
Results
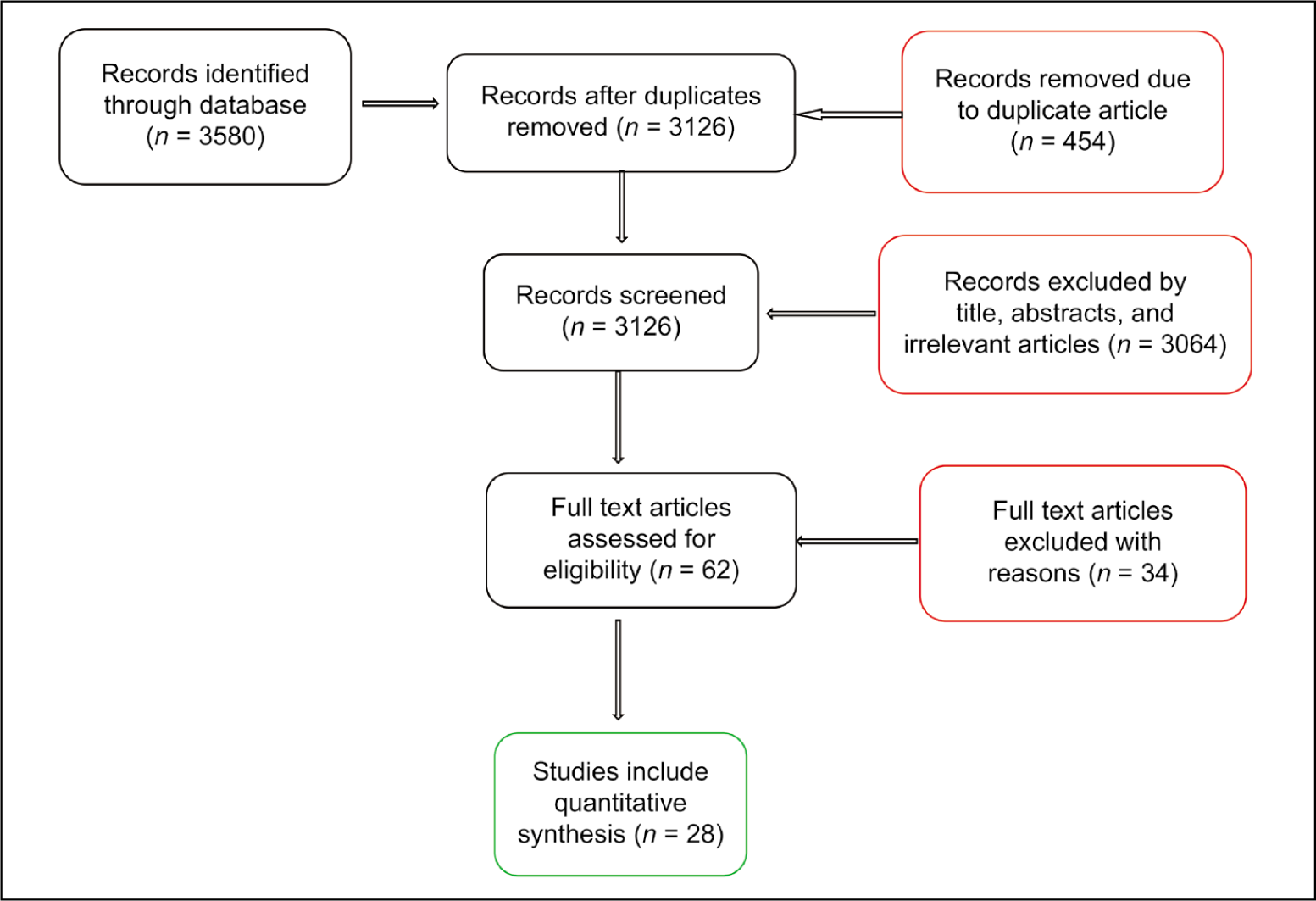
Out of the 62 papers initially identified, 34 were excluded for different reasons, as illustrated in Figure 1. The meta-analysis consisted of 28 studies, which involved a total of 9778 patients with essential hypertension. The studies that met the inclusion criteria compared the effect of ACEI and ARB in reducing BP in individuals with essential hypertension.
Preferred reporting items for meta-analyses flow diagram
Clinical efficacy data were available for comparison in all 28 studies, with BP reductions reported as both SBP and DBP in some studies. To facilitate the analysis and ensure standardization, the mean reduction in systolic and DBP was extracted from all the studies using the appropriate formula.
In Table 1, 4675 (n1) participants were given ACEI and 4969 (n2) participants were given ARBs. The mean SBP reduction (mmHg) of ACEI versus ARB for individual research was calculated.
Systolic blood pressure changes due to angiotensin-converting enzyme inhibitors versus angiotensin receptor blockers in essential hypertension in relation to standardized mean differences with 95% confidence interval

SMD: Standardized mean difference, SE: Standard error, CI: Confidence interval, GFR: Glomerular filtration rate
In Table 2, 4743 (n1) participants were given ACEI and 5035 (n2) participants were given ARBs. The mean DBP reduction (mmHg) of ACEI versus ARB for individual research was calculated.
Diastolic blood pressure changes due to angiotensin-converting enzyme inhibitors versus angiotensin receptor blockers in essential hypertension in relation to standardized mean differences with 95% confidence interval

SMD = Standardized mean difference, SE = Standard error, CI: Confidence interval, GFR: Glomerular filtration rate
ACEIs versus ARBs show a reduction in the mean SBP (mmHg) as well as mean DBP (mmHg) after their consumption.
During the statistical analysis, ACEI and ARB were assigned as n1 and n2, respectively, and the differences in their effects on mean systolic and DBP were incorporated in a meta-analysis to generate SMDs.
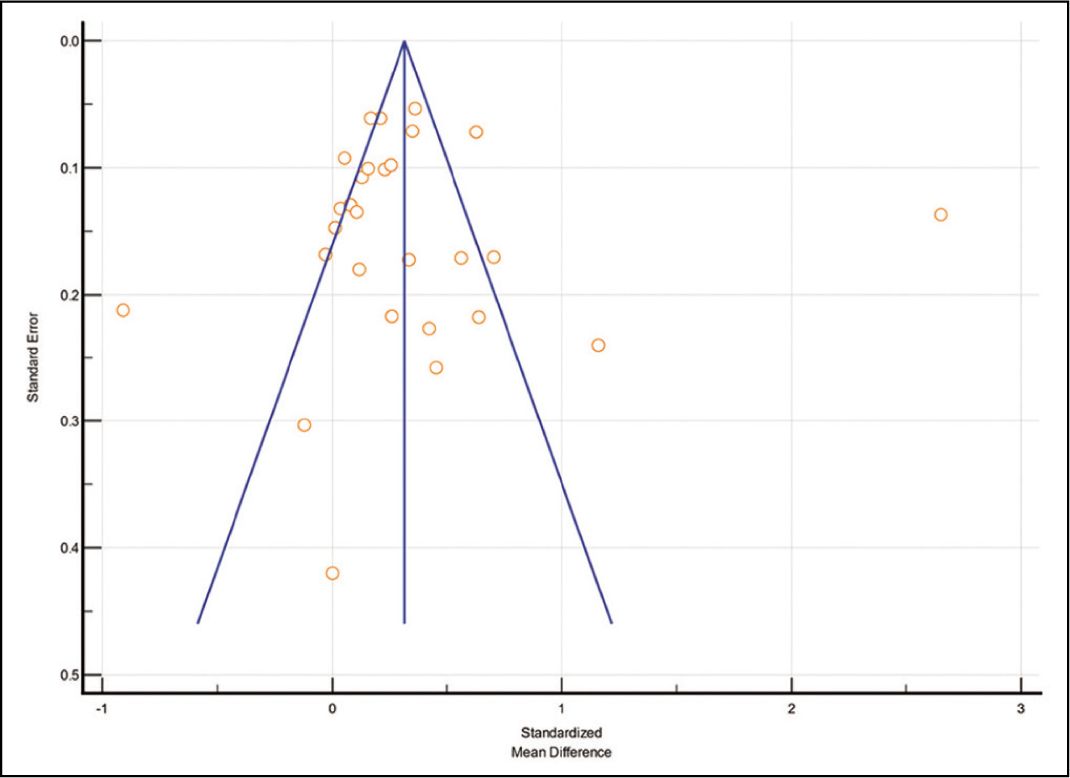
Both ACEIs and ARBs demonstrated reductions in both SBP and DBP from their respective baseline values. The pooled analyses of the studies indicated that ARBs were superior to ACEIs in terms of mean reduction in SBP, as evidenced by the random-effect model (SMD = 0.179, 95% CI 0.0975–0.260, P < 0.001) Mallaco (2012)[30] and the fixed-effect model (SMD = 0.207, 95% CI 0.167–0.248, P < 0.001). In addition, for mean reduction in DBP, ARBs also outperformed ACEIs, with a significant SMD of 0.329 in the random-effect model (95% CI: 0.161–0.496, P < 0.001) and an SMD of 0.317 in the fixed-effect model (95% CI: 0.276–0.357, P < 0.001). The funnel plots depicted in Figures 2 and 4 indicate fewer outliers and no publication bias. This is corroborated by the statistically significant results obtained from Kendall’s tau correlation test and the associated p-value in the publication bias table.
Funnel plot of studies included in systolic blood pressure reduction

Figures 3 and 5 display a forest plot representing the results, indicating that ARBs showed a greater mean reduction of BP compared to ACEIs in most of the studies included in the analysis.
Forest plot for systolic blood pressure reading in angiotensin-converting enzyme inhibitors versus angiotensin receptor blockers in essential hypertension

Funnel plot of studies included in diastolic blood pressure reduction
Forest plot for diastolic blood pressure reading in angiotensin-converting enzyme inhibitors versus angiotensin receptor blocker in essential hypertension

Moreover, Delles et al. 2008[27] (SMD is 0.740) and Malacco et al.[31] (SMD is + 0.715) showed the highest mean SBP reduction [Table 1], whereas Tikkanen et al. 1995[16] (SMD is 2.652) showed the highest DBP reduction [Table 2].
Discussion
In this systematic review and meta-analysis, the available evidence on the effectiveness of ACEIs and ARBs in reducing BP in patients with essential hypertension was analyzed. The meta-analysis, comprising 28 studies, yielded a key finding that ARBs exhibit greater efficacy than ACEIs in reducing both SBP and DBP.
ACEIs act by inhibiting the enzyme peptidyl-dipeptidase, thereby preventing the conversion of angiotensin I to angiotensin II. On the other hand, ARBs selectively block the binding of angiotensin II to angiotensin II receptor type 1.[5] The formation of angiotensin II, which is not mediated by ACE, is attributed to proteinases such as chymase, kallikrein, cathepsin G, and elastase-2 in human tissues. ACEIs do not inhibit the production of angiotensin II through non-ACE pathways, while ARBs are effective in blocking the actions of angiotensin II regardless of its mode of production.[32] Bradykinin is responsible for vasodilation as well as increased side effects such as cough and angioedema. ARBs are not responsible for an increase in bradykinin concentration, unlike ACEIs.
Furthermore, Anan et al. 2005[29] showed that ACEIs and ARB are equally efficacious in SBP and DBP reduction.
Twenty-eight RCTs were combined for a better statistical analysis. Overall, the results and conclusions of most previous studies were consistent with those presented herein. Almost all the drugs from both drug classes were included in the study.
There were several limitations to this study. We failed to include the side effects of both groups, neither we have taken combination therapy of both the antihypertensive drugs, and we have not stratified our efficacy endpoint based on age criteria, gender criteria, or race criteria. A previous study also compared the cognitive function of the elderly. Fimasartan and Allisartan were excluded as they were not used globally.
Based on the findings of this meta-analysis, the majority of the studies demonstrated that ARBs exhibited greater effectiveness compared to their counterpart in the treatment of essential hypertension. Chen et al., 2004[31] Coca et al.,[8] De Rosa et al.,[9] Himmelmann et al.,[10] Leonetti et al.,[11] Malacco et al.,[12] Mallion et al., 2011 (ambulatory patients) [14] Mallion et al., 2011[14] Palma et al.,[15] Tikkanen et al.,[16] Zanchetti and Omboni,[17] White 2002,[19] Derosa et al.,[20] Fogari et al.,[21] Holwerda et al.,[22] Nalbantgil et al.,[23] Omboni et al.,[24] Williams et al.,[26] Williams et al.,[26] Williams et al.,[25] Delles et al.,[27] Mallion et al. 2011 ambulatory patients,[28] Napoli et al., 2016[28] and Malacco et al. 2012[30] As demonstrated in Table 3, our study stands out by incorporating a greater number of RCTs when compared to other research endeavors. The data derived from this extensive inclusion not only provides valuable guidance for prescribers but also offers deeper insights into the comparative effectiveness of ARBs versus ACEIs.
Comparison of earlier studies with this meta-analysis

ARBs: Angiotensin receptor blockers, ACEI: Angiotensin-converting enzyme inhibitor, BP: Blood pressure, SBP = Systolic BP, DBP = Diastolic BP
Conclusion
The analysis revealed that ARB provides superior benefits over ACEI in terms of achieving better BP control. ARB demonstrated greater reductions in both systolic and DBP compared to ACEI. Therefore, ARB is a more favorable option for the treatment of essential hypertension, leading to improved outcomes.
Future work
Comparison of the efficacy of the drug classes can be done with stratification by age, gender, and race
The evaluation of hypertension can help assess the mortality and morbidity of the patients
The efficacy of different drug classes can be compared in the context of secondary hypertension
An adverse effect profile comparison can be done between ACEI and ARB.
Footnotes
Acknowledgements
We are thank full to head of department of pharmacology for their valuable suggestions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
Not applicable.
CRediT Author Statement
All authors have equal contribution toward the manuscript.
Data Availability
Yes.
Use of Artificial Intelligence
No.