
Abstract
Background:
Lipomas are the most frequent neoplasm of mesenchymal origin in the head-and-neck region. Around 15% of lipomas are found in the head-and-neck region. The usual site where lipomas can be found in the head-and-neck region is in the posterior triangle of the neck but they can also be found in the anterior neck, infratemporal fossa, submandibular space, larynx, pharynx, and parotid gland. The incidence of parotid lipoma ranges from 0.6% to 4.4% of all parotid neoplasms. There are two histological variants, focal lipoma and diffuse infiltrating variant. We describe two cases of rare focal lipoma of the parotid gland, therefore, must be reported. As rare as it may appear, existing relevant literature suggest management to includes definitive radiological investigations such as magnetic resonance imaging (MRI) and complete removal of lipoma with or without a cuff of parotid tissue.
Introduction
The parotid gland is the largest salivary gland in the human body. Various benign and malignant pathologies are associated with the parotid gland: mucoepidermoid carcinoma, adenoid cystic carcinoma, acinic cell carcinoma, and rarely lipomas. Lipomas are the most frequent neoplasm of mesenchymal origin in the head-and-neck region. Around 15% of lipomas are found in the head-and-neck region.[1-3] The usual site where lipomas can be found in the head-and-neck region is in the posterior triangle of the neck but they can also be found in the anterior neck, infratemporal fossa, submandibular space, larynx, pharynx, and parotid gland. The incidence of lipomas in the parotid gland ranges from 0.6% to 4.4% of all parotid tumors.[2] There are two histological variants, focal lipoma and diffuse infiltrating variant.
We describe two cases of rare focal lipoma of the parotid gland, therefore, must be reported. As rare as it may appear, existing relevant literature suggest management to include definitive radiological investigations such as magnetic resonance imaging (MRI) and complete removal of lipoma with or without a cuff of parotid tissue.
Case Reports
Case 1
A 53-year-old male with no comorbid presented with left-sided facial swelling for the past 2 years. On examination, there was 2 cm × 3 cm soft swelling of the parotid. Facial functions were intact and no cervical lymph nodes were appreciated. The patient subsequently underwent superficial parotidectomy. Intraoperatively, tumor of approximately 5 cm × 4 cm in superficial lobe of the left parotid gland was found. Facial nerve identified and saved. Histopathology reported parotid lipoma. The patient was seen in clinic on a 1-week postoperative follow-up. Facial functions were normal, however, he did complain of left ear numbness which could have been due to tension neuropraxia following stretching of greater auricular nerve.
Case 2
A 67-year-old male presented with a painless right angle of mandible swelling for 15 years. The patient underwent right intraparotid excision of mass. Intraoperatively, tumor was about 4 cm × 5 cm, interspersed between deep and superficial lobe of parotid, a facial nerve not encountered during surgery. Histopathology revealed intraparotid lipoma. The patient was lost to follow-up with ENT. Six years later, the patient presented with a lump in his retroareolar region of his right breast. Biopsy revealed invasive ductal carcinoma, mammography reported BIRAD IV. Clinically staged T4bN0, the patient subsequently underwent a mastectomy followed by radiation and chemotherapy.
Microscopic examination of tumors from both patients revealed circumscribed benign adipocytic neoplasms surrounded by thin fibrous capsule. The lesions were composed of sheets of mature adipocytes traversed by fibrous septate of variable thickness. No lipoblasts or atypical stromal cells were seen. At the periphery, native benign parotid gland parenchyma composed of serous acini and ducts were appreciated. A summary of patient demographics and outcomes of both cases is shown in Tables 1 and 2, respectively.
Patient demographics and preoperative investigations

FNAC: Fine needle aspiration cytology
Surgical and postoperative outcomes

Discussion and Conclusion
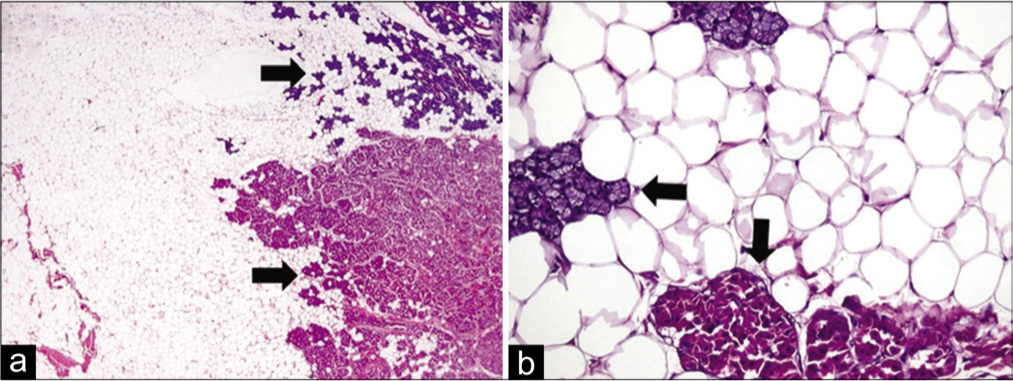
There are two variants of lipomas namely: focal lipoma and diffuse infiltrating variant.[4] Focal lipoma has a capsule that insulates it from surrounding parotid parenchyma. Diffuse infiltrating lipomatosis has adipocytes infiltrating parotid parenchyma.[5] Both of our patients had focal lipomas on histological examination, as shown in Figure 1a and b. Other lipomatous lesions such as fibro lipoma, angiolipoma, and sialolipoma have also been reported.[6,7] Hibernoma is a collection of brown fat as opposed to lipoma which is a collection of yellow fat.[8]
(a) Low power view showing sheets of mature adipocytes with clear cytoplasm. Native benign salivary gland parenchyma is also present at periphery (arrows). (H and E, ×20). (b) High power view showing mature adipocytes with clear cytoplasm. Normal serous acini with granular basophilic cytoplasm are also seen (horizontal arrow). Few acini also exhibit oncocytic change, i.e., homogenous, dense eosinophilic cytoplasm (vertical arrow). (H and E, ×200)
Lipomas of the parotid gland are present in the fourth to sixth decade of life.[2] Most lipomas of the deep lobe have been reported in the fourth decade.[4] They are more prevalent in males than females (3:1).[5,9] However, there are studies that have reported a greater predilection for males (10:1).[4] Both of our patients were males and had lipomas located in the superficial lobe. Parotid lipomas are painless, slow-growing tumors,[4] with soft to doughy consistency, more commonly in the superficial lobe of the parotid gland.[10] They are usually asymptomatic but if they grow large enough they can affect the mastication and speech. Patients commonly present with cosmetic disfigurement which is the primary concern.[10]
The mean time of presentation of patients is 3.2 years.[9] In our cohort, the first patient presented after 2 years and the second patient had this swelling increasing in size for 15 years. Etiological factors reported are heredity, obesity, diabetes, endocrine disorders, insulin injections, corticosteroid therapy, and trauma.[11] The concept of lipomas arising after trauma is now discounted.[10] Lipomas arising as a result of trauma are not true lipomas and are termed pseudolipomas as they lack encapsulation.[10] They occur in the thigh and pelvis where a deficiency in Scarpa’s fascia is present.[12] None of our patients had any comorbid conditions or had a history of trauma.
Preoperative radiological examination for a parotid neoplasm is commonly ultrasound as it is cheap, readily available and can be performed in the office. It can also be facilitated by fine-needle aspiration cytology (FNAC). Lipomas are well defined, hyperechoic to muscle and with linear echogenic lines.[13] MRI is now regarded as the primary imaging modality of parotid lipomas.[1] They have high-intensity signals on T1-weighted images and low-intensity signals on T2-weighted images.[1,14] T1 fat-suppressed images can reveal parotid lipomas to be of adipocyte origin leading to a definitive diagnosis. Computed tomography (CT) images reveal a homogenous, hypodense mass with few septations. Density ranges from − 50 to − 150 Hounsfield which is characteristic of lipomas.[1]
FNAC is a valuable modality for parotid neoplasms, in the case of parotid lipomas, they are of little clinical significance.[5,15,16] Management of parotid lipomas varies with some authors suggesting enucleation that is removal of lipoma with minimal parotid tissue, to others suggesting a formal superficial parotidectomy.[17-19] In our first case, the lipoma was situated slightly deep. The facial nerve was identified at the temporomastoid suture line and superficial parotidectomy was performed. In our second case, lipoma was more superficial, and an enucleation was performed. Facial nerve dysfunction after parotidectomy of benign lesions has been reported up to 65%.[20] Both patients had no facial weakness postoperatively.
Limitation
Despite the fact that lipoma was interspersed between deep and superficial lobe of parotid gland, the second case in our study developed clinically stage T4bNo breast carcinoma, 6 years after intraparotid excision of mass for parotid lipoma. As the cases included were retrieved retrospectively, this unusual association between intraparotid excision of mass interspersed parotid lipoma and later, development of other carcinomas, if not particularly breast, was not addressed initially, and could potentially be an unrecognized confounding factor. This requires more thorough studies prospectively.
Conclusion
Parotid lipomas are rare entities that must be kept as a differential for all clinically soft parotid swellings. Other lipomatous lesions such as sialolipoma, angiolipoma, and fibrolipoma can also be kept as a differential. Management includes definitive radiological investigations such as MRI and complete removal of lipoma with or without a cuff of parotid tissue instead of regular ultrasound followed by FNAC. Although our cases were managed on the same regular outlines, but reporting these cases would suffice the potential role of MRI and CT scans for parotid swelling as per existing literature.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Consent form was taken and duly signed by both participants of cases reported.
Declaration of Patient Consent
The authors certify that he has obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
CRediT Author Statement
AA: Made substantial contributions to the conception SA: Design of the work; and the acquisition, analysis, and interpretation of data and submission HI: Have drafted the work MI: Substantively revised work SH: Write-up and literature search.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available as containing information can compromise the privacy of research participants.
Use of Artificial Intelligence
Study was conducted after receiving institutional ethical committee exemption as it’s a retrospective chart review, performed in the department of Surgery at Aga Khan University Hospital, Karachi, Pakistan. A total of 213 cases were identified who underwent parotidectomy. Two cases were identified with parotid lipoma on final histology. Data was collected both from patients record and online database maintained in the hospital.