
Abstract
Introduction:
Although neurocysticercosis is the most common parasitic infestation in central nervous system, yet the intramedullary spinal involvement remains the extremely rare site of presentation. Due to its extreme rarity, these tumors pose diagnostic and therapeutic challenges and may be interpreted as intramedullary tumors. Hence to avoid this conundrum, a detailed clinical, radiological, and histopathological evaluation is mandatory to come to a definitive diagnosis.
Keywords
Introduction
Neurocysticercosis is the parasitic infestation of central nervous system, caused by the larval stage of Taenia solium. The prevalence of the disease is rare about 4% in endemic areas.[1] The occurrence of spinal cysticercosis is rarer still and accounts for 1.2%–5.8% of all cases of neurocysticercosis.[2]
Spinal cysticercosis can be extraspinal (vertebral) or intraspinal (epidural, subdural, arachnoid, or intramedullary). The ingestion of the larval form by eating undercooked food causes intestinal infection, which later on disseminates hematogeneously to encyst in the human brain, skeletal muscle, subcutaneous tissue and eyes, intramedullary spinal cord involvement being the least common.
In such cases, imaging findings are nonspecific and carry myriads of differentials; hence, the definitive tool for diagnosis remains detailed histopathological examination.
We, hereby report a case of intramedullary cysticercosis at D6-D7 level, which was treated surgically and diagnosed intraoperatively on frozen section examination.
Case Report
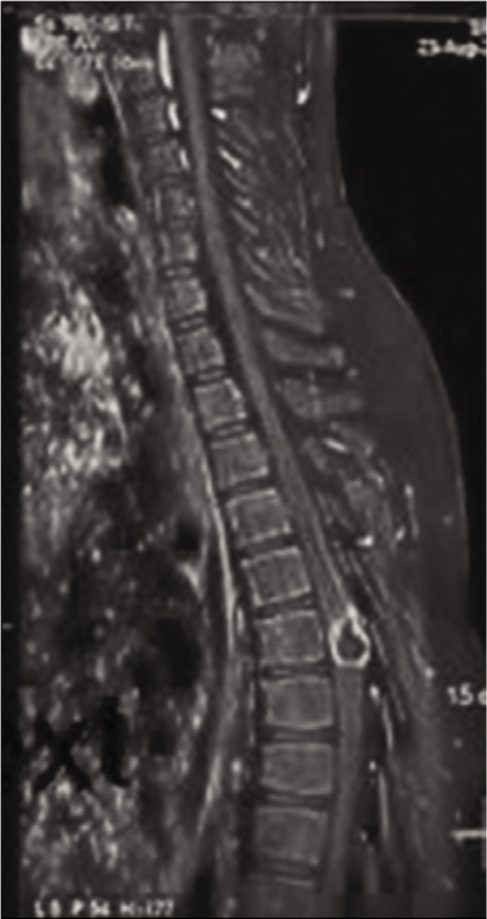
A 19-year-old male patient presented as a follow-up case of D6-D7-Intramedullary lesion. His magnetic resonance imaging (MRI) spine showed a lobulated intramedullary mass of 16 mm × 13 mm at D6 vertebral level. The lesion was hypointense on T1 and hyperintense on T2 and short tau inversion recovery (STIR). The lesion showed capsular and nodular enhancement with central necrosis. The differentials given on imaging were tuberculosis and neoplastic lesions such as ependymoma or astrocytoma [Figure 1]. Following this, the patient was put on anti-tubercular drugs for few months and was on steroids for increase in ataxia.
A lobulated intramedullary mass at D6-D7, showing hypointensity at T1 and hyperintensity at T2.
He visited the department of neurosurgery at our hospital with complaints of partial retention of urine, bilateral lower limb weakness, and back pain for 2 days. On admission, his vitals were stable. On general physical examination, the Glasgow Coma Scale was E4V5M6, extraocular movements were normal, respiration was spontaneous, stable, and adequate. Power in legs was normal.
He was further planned for D6-D7 Laminectomy along with excision of the intramedullary lesion.
Intraoperative findings
The dura was bulging out at the D6-D7 region. The dorsal surface of cord was partially branched due to intramedullary pressure. A well-defined cyst surrounded by a thin capsule and fatty tissue anteriorly and inferiorly respectively was seen.
Intraoperative consultation was done to exclude a neoplastic etiology. The frozen section revealed a cyst wall consistent with cysticercosis.
Pathological findings
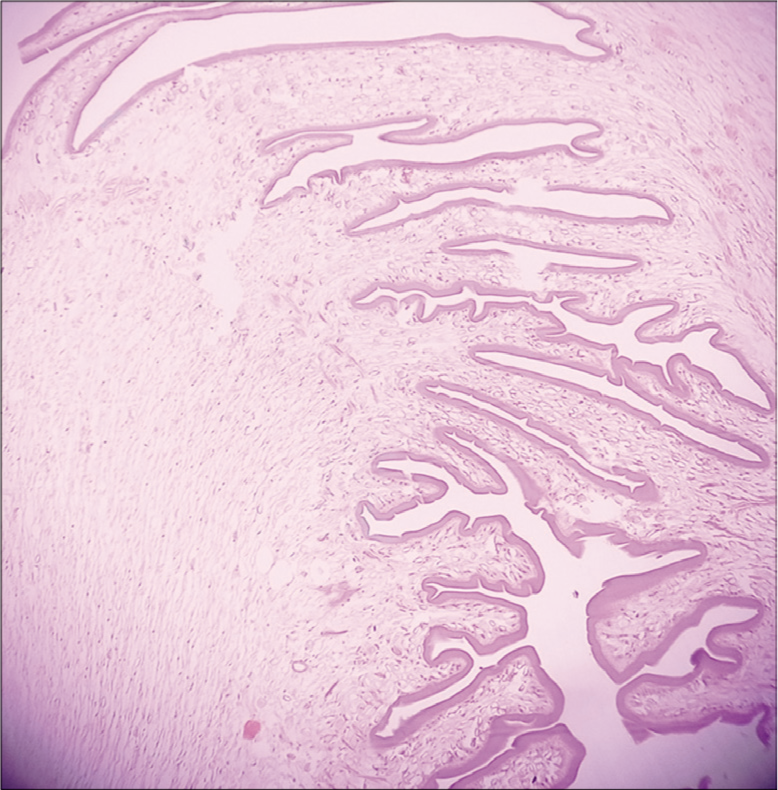
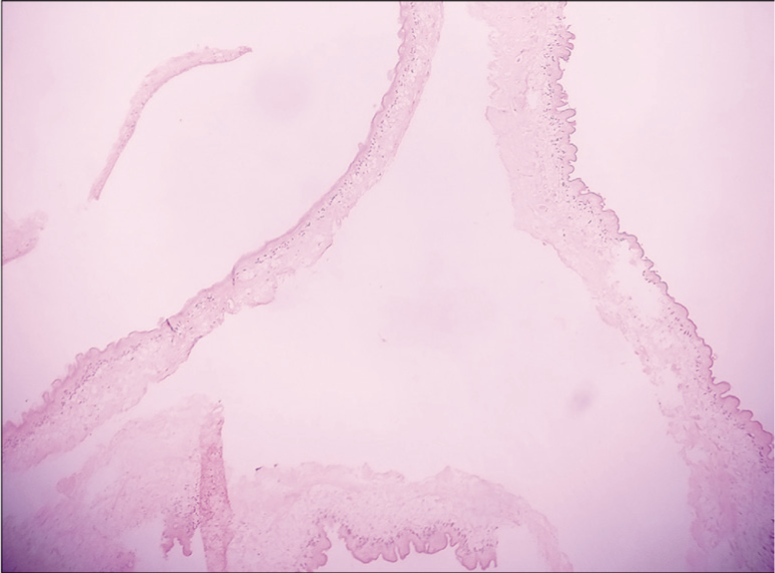
Grossly, a single-solid cystic soft-tissue piece was received measuring 1 cm × 0.8 cm × 0.5 cm. Microscopic examination of permanent sections revealed bits of tissue containing cyst wall with outer corrugated hyaline and inner parenchymal layer and focal invagination and calcification. Features were consistent with Parasitic Cyst of Cysticercosis Cellulosae [Figures 2 and 3].
Cyst wall with outer corrugated hyaline and inner parenchymal layer and focal invagination (H and E X100).
Cyst wall with outer corrugated hyaline and inner parenchymal layer and focal invagination (H and E X400).
Postoperative events
The prescribed guideline treatment of albendazole was advised and the patient responded well.
Discussion
Spinal neurocysticercosis is a rare form of cysticercosis, with isolated intramedullary site involvement being the rarest. The spread is either by blood or through ventriculo-ependymal pathway.[3] Clinically, the patient’s symptoms vary depending upon the location and range from vague pain and radiculopathy, paraesthesia, numbness, or weakness of limbs to frank cauda equine syndrome.
It is difficult to suspect a case of spinal neurocysticercosis in the absence of previous history.
Plain radiographs are of less value as sometimes calcification of cysts or soft tissue can be seen. MRI helps in diagnosing these lesions as they appear hyperintense on T2- and hypointense on T1-weighted images.
Cerebrospinal fluid (CSF) examination may show low or normal glucose levels, increased proteins, lymphocytic pleocytosis, and eosinophilia. Enzyme-linked immunosorbent assay or enzyme-linked immunoelectric transfer bolt assay of CSF or serum may help in the diagnosis.
In our case, there was no history of neurocysticercosis and the patient was not from an endemic region, hence CSF examination was not performed. The diagnosis of cysticercosis was largely dependent on the histopathology results. The constellation of symptoms of clinical history of exposure and radiological and histopathological findings aid in a definitive diagnosis.[4]
The differential diagnosis of intramedullary cystic lesions includes arachnoid cyst, ependymal cyst, neuroenteric cyst, sarcoidosis, and neoplasm such as ependymoma and astrocytoma. Our case was hypointense on T1 and hyperintense on T2 and STIR, hence the differentials of tuberculosis and neoplastic lesion ependymoma and astrocytoma were considered. If the diagnosis is doubtful and the neurological condition worsens, surgical excision of the cyst should be considered as in our case. Recent studies have reported that surgery is a good treatment option, which removes the mass, thereby decompressing the spinal cord and relieving the symptoms.
Albendazole is proven to be effective in the treatment of patients with neurocysticercosis (15 mg/kg/day) for 4–6 weeks.
Conclusion
Intramedullary cysticercosis represents a diagnostic challenge. Medical treatment may be considered in patient with stable neurological conditions and a strong suspicion for cysticercosis should be considered in the differential diagnosis of intramedullary cystic lesions. Surgery always remains the treatment of choice in patient with neurological deterioration and diagnostic dilemma to facilitate removal of the lesion and enable a definitive diagnosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
CRediT Author Statement
All author’s have contributed to the manuscript writing, editing and reviewing.
Data Availability
Dharmshila Narayana Superspeciality Hospital, New Delhi.