
Abstract
Introduction:
This study was carried out to know the demographic and clinicoradiological profile of acute stroke patients in our hospital, which will provide baseline data to plan for future preventive strategies for government and will help young physicians to deal with this disabling disease.
Materials and Methods:
A total of 250 patients with age >18 years were recruited for a hospital-based prospective analytical study. The participants were selected from those who attended the emergency department or were admitted to the hospital with a new onset of stroke, confirmed by neuroimaging such as computed tomography (CT) or magnetic resonance imaging (MRI). The study population comprised patients presenting with symptoms suggestive of acute stroke, above 18 years of age, and willing to provide informed written consent. Patients with old cerebrovascular accidents, transient ischemic attacks, stroke mimics, intracerebral bleed posthead trauma, or inconclusive or normal CT/MRI scans were excluded from the study.
Results:
Our study population (n = 262) had a mean age of 60.1 ± 14.8 years, with 181 males (69%) and 81 females (31%). The stroke subtypes were as follows: ischemic (54.6%), hemorrhagic (42%), and subarachnoid hemorrhage (SAH) (3.4%). Hypertension (85.1%), alcohol consumption (63%), and dyslipidemia (59.5%) were the predominant risk factors in our patients. In our study, majority of the hemorrhagic stroke was distributed in capsuloganglionic area (77 patients), followed by temporoparietal area and intraventricular bleed (10 patients each). In our study, there were 143 patients with ischemic stroke, among which 58 were in the left middle cerebral artery (MCA), 46 in the right MCA, 6 in the left anterior cerebral artery (ACA), 14 in the right ACA, and 18 in posterior cerebral artery territories. In our study, the sensitivity of clinical localization of anterior circulation stroke was 94.35%, specificity of 89.47%, negative predictive value (NPV) of 70.83%, and positive predictive value (PPV) of 98.32%. Similarly, the sensitivity of clinical localization of posterior circulation stroke (PCS) was 89.47%, specificity of 94.35%, NPV of 98.32%, and PPV of 70.83%.
Conclusion:
The most common stroke subtype was ischemic (54.6%), followed by hemorrhagic (42%) and SAH (3.4%). Hypertension, alcohol consumption, and dyslipidemia were the predominant risk factors. Among hemorrhagic strokes, the capsuloganglionic area had the highest distribution. The clinical localization showed high sensitivity and specificity for both anterior and PCSs.
Introduction
Stroke is a complicated neurological disease that can result in specific neurological abnormalities due to thrombus, emboli, hemorrhage, inflammatory and noninflammatory vasculitis, or hematological illnesses such as coagulopathy. Stroke is a significant cause of disability and the second leading cause of death globally.[1] Its burden is expected to rise, particularly in middle- and low-income countries like India, due to the increasing prevalence of risk factors such as obesity, diabetes mellitus (DM), hyperlipidemia, and hypertension. The frequency of stroke also rises with advancing age. Despite progress in reducing age-standardized death rates, the overall burden of stroke remains high and is anticipated to increase as populations age, and noncommunicable diseases become the main cause of morbidity in low- and middle-income countries. Effective stroke prevention strategies are crucial to address this escalating health challenge.[2]
More than three times as many Asians died from strokes as from coronary heart disease (CHD). According to another study, Asian males had a stroke death rate of 44–102.6/100,000 people, compared to 19.3 for Australian males. The average age of stroke patients is thought to be 15 years lower in underdeveloped nations than in wealthy ones. According to a research conducted in India, persons under the age of 40 years account for roughly 10%–15% of all stroke cases. In India, a higher percentage of young people are impacted than in wealthy nations. The most frequent subtype of stroke is ischemic, followed by thromboembolic, and between 21% and 48% of strokes in young people are brought on by atherosclerotic major artery occlusive disease. Stroke occurs more frequently in males than in women. The ratio of men to women in India is 7:1. This can be because males in India are more likely than women to use tobacco products and drink alcohol, which are risk factors. The average age at which males in India get a stroke is 63–65, compared to 57–68 for women.[3-5]
Currently, the majority of stroke diagnoses are made through neuroimaging methods such as computed tomography (CT) scans or magnetic resonance imaging (MRI). Numerous countries, including India, have done research on the epidemiology and risk factors of acute stroke. Stroke is the third leading cause of mortality globally, behind CHD and all forms of cancer. Asians do, however, have a greater frequency of stroke and a lower risk of CHD compared to Caucasians.[6,7] Therefore, this study was carried out to know the demographic and clinic radiological profile of acute stroke patients in our hospital which will provide baseline data to plan for future preventive strategies for government and will help young physicians to deal with this disabling disease.
Materials and Methods
After obtaining institutional ethics committee approval (SVMH/March 22, 2021), a total of 250 patients with age >18 years were recruited for a hospital-based prospective analytical study. The participants were selected from those who attended the emergency department or were admitted to the hospital with a new onset of stroke, confirmed by neuroimaging such as CT or MRI. “New onset stroke” refers to the sudden onset of neurological symptoms due to disrupted blood flow in the brain, characterized by rapid development of focal deficits. Symptoms emerge within minutes to hours, indicating an acute event. Radiologically, acute brain imaging (CT/MRI) assesses acute infarcts and bleeds, providing critical information for prompt diagnosis and appropriate treatment. Subacute infarcts or bleeds, visible but occurring days to weeks before assessment, are not considered part of “new onset stroke,” which focuses on recent symptoms and acute radiological findings for timely intervention and better patient outcomes.
The study was conducted in the Emergency Block/Medical Wards of the Department of General Medicine at SVRR Government General Hospital, Sri Venkateswara Medical College, Tirupati. The study population comprised patients presenting with symptoms suggestive of acute stroke, above 18 years of age, and willing to provide informed written consent. Patients with old cerebrovascular accidents, transient ischemic attacks, stroke mimics, intracerebral bleed post head trauma, cerebral venous thrombosis, and inconclusive or normal CT/MRI scans were excluded from the study. The study period was 1 year from the date of approval from the Institutional Scientific and Ethical Committee. The study methodology involved conducting history and clinical examinations, obtaining written and informed consent from each patient, and conducting various baseline investigations including CT scans, MRIs, complete blood tests, liver and renal function tests, serum electrolyte analysis, urine tests, baseline electrocardiograms (ECGs), chest radiographs, lipid profiles, two-dimensional echo, and carotid Doppler. Sociodemographic parameters such as age, gender, socioeconomic status (SES), and locality of patient were assessed. Clinicoradiological parameters such as risk factors, type of stroke, speech abnormalities, presence of 7th nerve palsy, sensory deficit, echo changes, and ECG changes were assessed. A total of 250 patients with age >18 years are recruited from those who attended the emergency or are admitted in hospital with the new onset of stroke and confirmed by neuroimaging.
Continuous data were expressed as mean ± standard deviation and median and analyzed by unpaired t-test. Categorical data presented as numbers and percentages were analyzed by Chi-square test. P ≤0.05 was considered statistically significant.
Results
The mean age of our study population was 60.103 years with a standard deviation of 14.795 years. In our study, 181 patients were male, showing a male predominance in cerebrovascular accidents. There were 81 females in our study. In our study of 262 patients, 143 patients (54.6%) had ischemic stroke, 110 patients (42%) had hemorrhagic stroke, and nine patients (3.4%) had subarachnoid hemorrhage (SAH). In our study, according to new B. G. Prasad SES Classification, majority of the patients belonged to middle class (165 patients), followed by lower class (91 patients). There were six patients from upper class. In our study of 262 patients, 55% (144) of patients were from urban area and 45% (118) of patients were from rural area. In our study of 262 patients with stroke, hypertension was the predominant risk factor, which was present in 85.1% of patients followed by alcohol consumption (63%), anemia (6.6%), dyslipidemia (59.5%), smoking (37.4%), diabetes (21%), and previous history of stroke and heart disease [Table 1]. As per TOAST classification of stroke, 42% had large artery stroke, followed by 54.6% cardioembolism and 3.4% had subarachnoid hemorrhage.
Distribution of variables among the study participants (n=262)
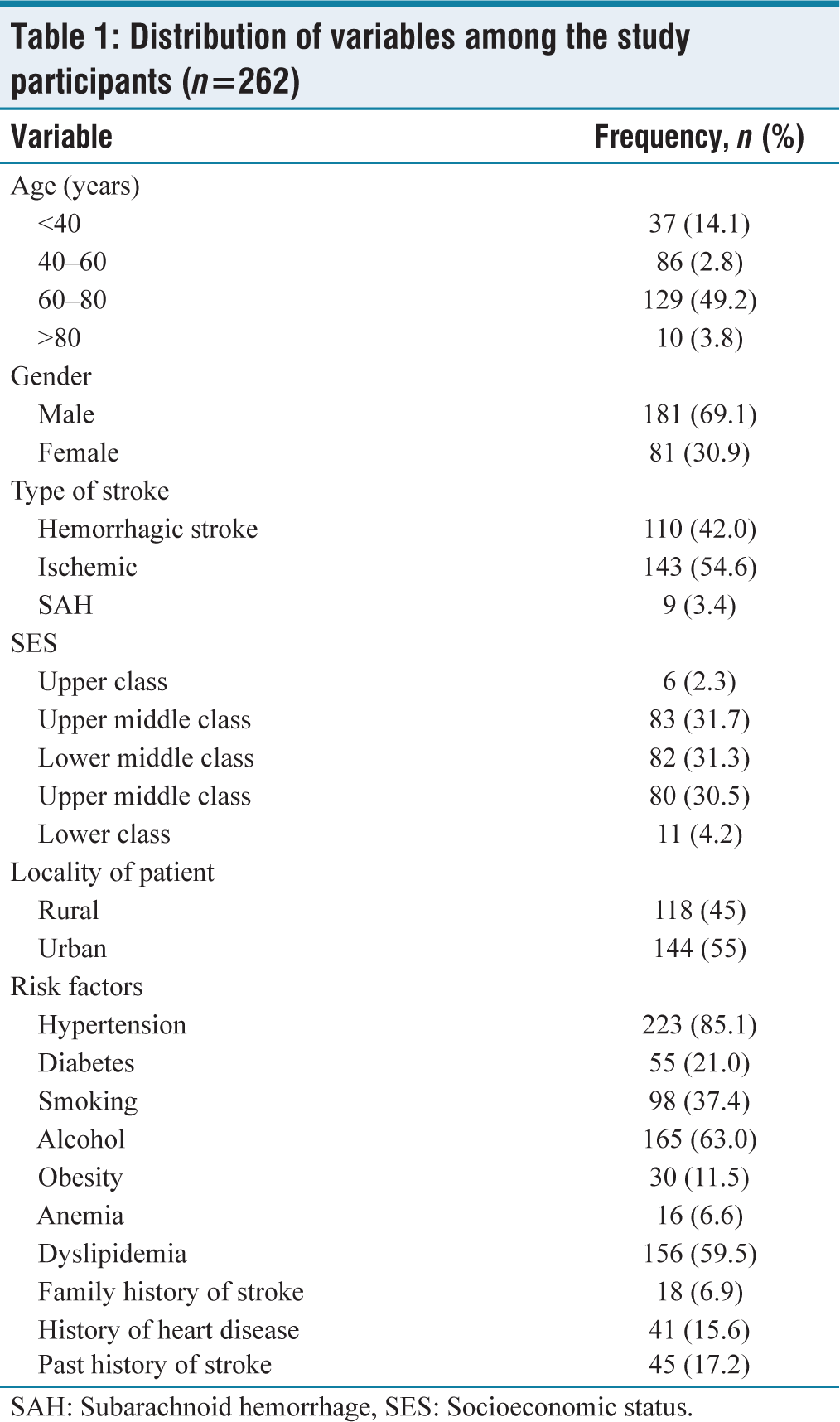
SAH: Subarachnoid hemorrhage, SES: Socioeconomic status
Aphasia was more predominant in hemorrhagic stroke, which was present in 57.3% of patients and among 28% of patients with ischemic stroke. Dysarthria was found in 34.3% of patients with ischemic stroke and 17.3% of patients with hemorrhagic stroke. In 10 patients (7%) with ischemic stroke, speech could not be assessed due to altered sensorium. The distribution of speech abnormalities among type of stroke was statistically significant. In our study of 262 patients with stroke, among hemorrhagic stroke, five patients had left upper motor neuron (UMN) palsy, and 16 patients had right UMN palsy. Among patients with ischemic stroke, 20 patients had left and 19 patients had right 7th nerve UMN palsy. In our study of 262 patients, sensory deficit was present in 16 patients, of which eight had hemorrhagic stroke and eight patients had ischemic stroke.
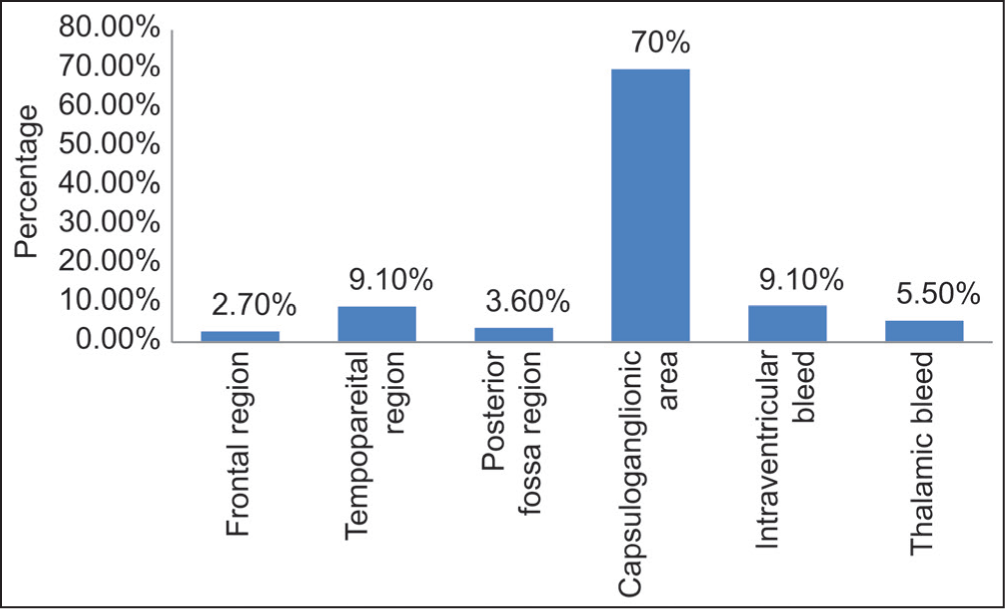
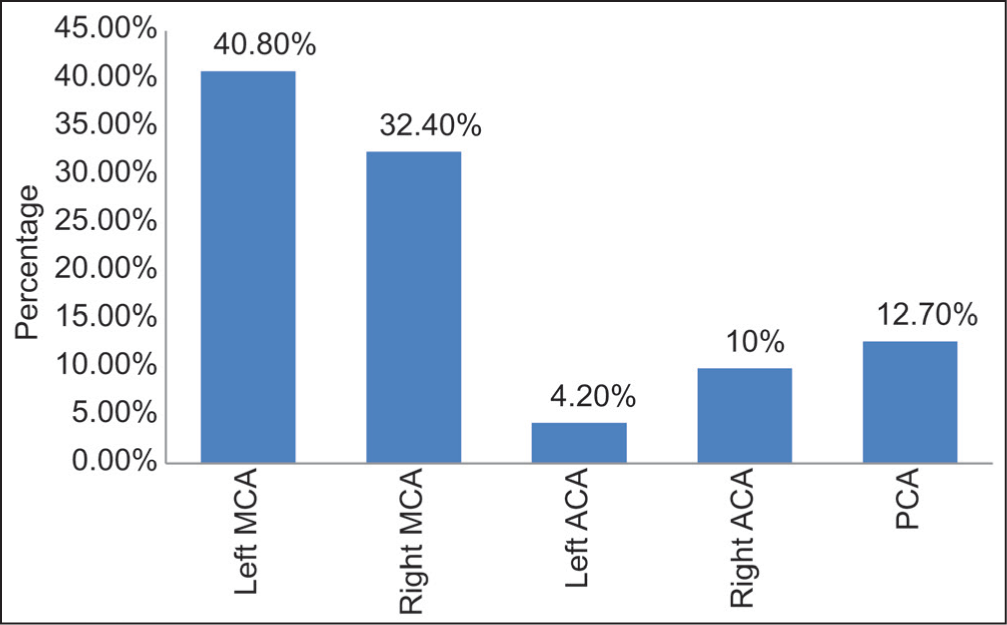
In our study population of 262 patients, echo changes were seen in 28 patients with hemorrhagic stroke, 32 patients with ischemic stroke, and one patient with SAH. Atrial fibrillation was seen on ECG in 24 patients of our study population who had ischemic stroke [Table 2]. In our study, majority of the hemorrhagic stroke was distributed in capsuloganglionic area (77 patients), followed by temporoparietal area and intraventricular bleed (10 patients each) [Figure 1]. In our study, there were 143 patients with ischemic stroke, among which 58 were in the left middle cerebral artery (MCA), 46 in the right MCA, six in the left anterior cerebral artery (ACA), 14 in the right ACA, and 18 in posterior cerebral artery territories [Figure 2].
Distribution of affected area among hemorrhagic strokes (n = 110)
Distribution of study variables among type of stroke in our study population
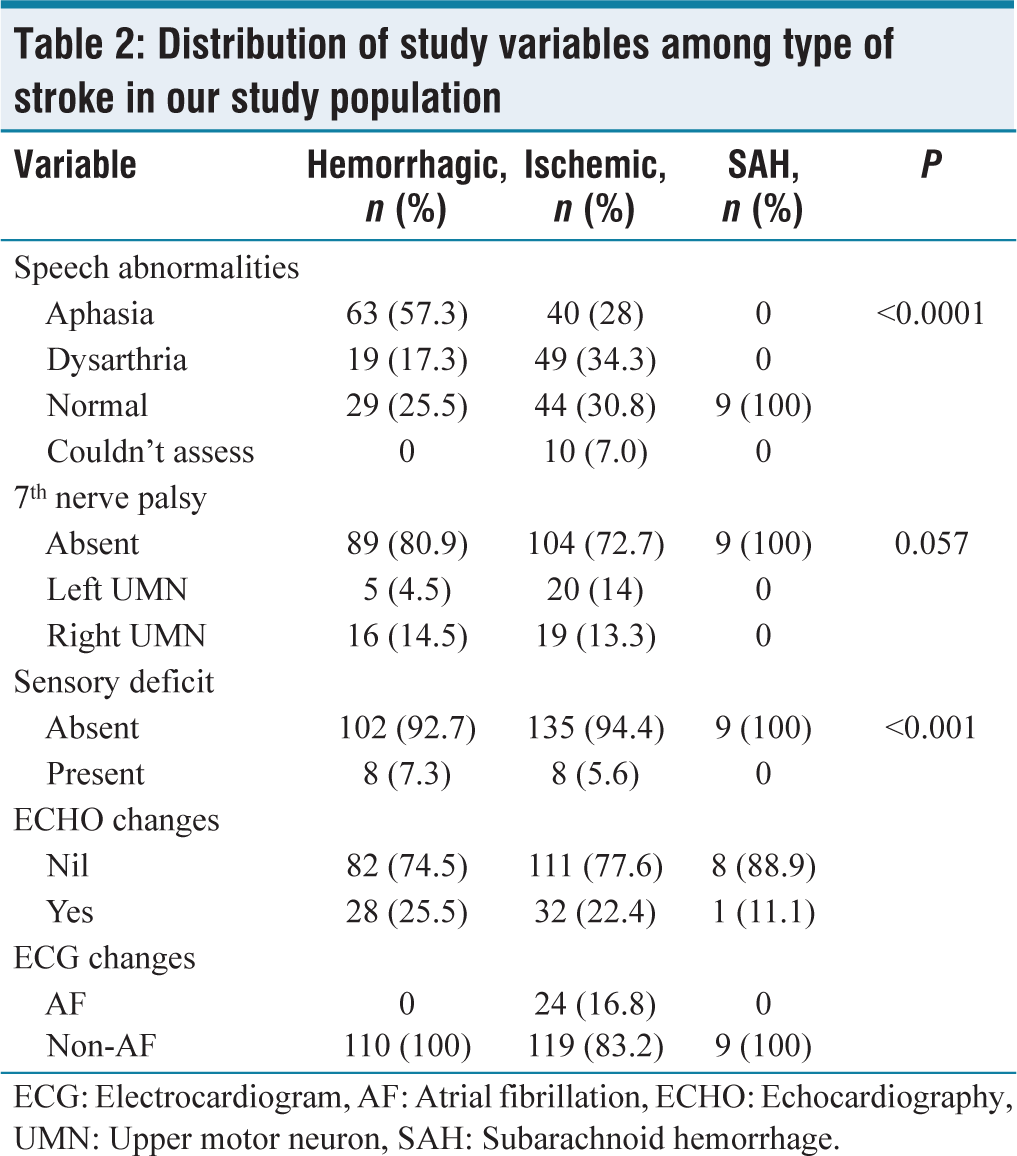
ECG: Electrocardiogram, AF: Atrial fibrillation, ECHO: Echocardiography, UMN: Upper motor neuron, SAH: Subarachnoid hemorrhage
Distribution of affected vessel in ischemic stroke (n = 143)
In our study, the sensitivity of clinical localization of acute coronary syndrome (ACS) was 94.35%, specificity of 89.47%, negative predictive value (NPV) of 70.83%, and positive predictive value (PPV) of 98.32%. Similarly, the sensitivity of clinical localization of posterior circulation stroke (PCS) was 89.47%, specificity of 94.35%, NPV of 98.32%, and PPV of 70.83% [Table 3].
Diagnostic accuracy of clinical localization of ischemic stroke
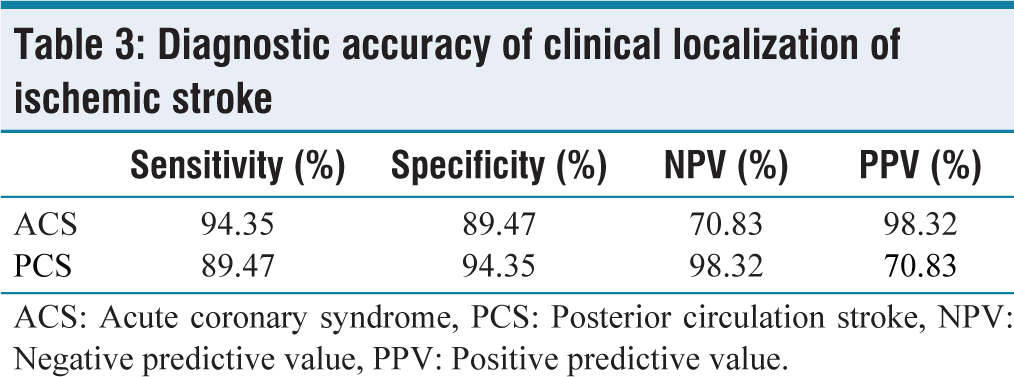
ACS: Acute coronary syndrome, PCS: Posterior circulation stroke, NPV: Negative predictive value, PPV: Positive predictive value
In our study of 262 patients, 35 patients expired of the disease accounting for a mortality rate of 13.35%. 28 patients had complete recovery and 199 patients had partial recovery among our study population. Among hemorrhagic stroke, there were 27 deaths accounting for mortality of 24.54%. None of the patients had complete recovery. Among patients with ischemic stroke, 4 patients died, 116 patients had partial recovery, and 23 patients had complete recovery. The mortality rate among ischemic stroke was 2.7%. Among patients with SAH, the mortality rate was 44.4%.
Discussion
Cerebrovascular diseases, specifically stroke, are the most prevalent and serious neurological illnesses that affect adults. They account for at least 50% of the neurologic illnesses in a general hospital and are the second leading cause of mortality worldwide. However, stroke often receives less attention from health-care professionals compared to other disorders. Understanding the risk factors associated with stroke is crucial for implementing effective preventative measures.
Hypertension is the most significant modifiable risk factor for cerebrovascular disease, while age is the most significant nonmodifiable risk factor for ischemic stroke. Other modifiable risk factors include smoking, hyperlipidemia, and DM. The elderly population is at the highest risk for stroke, with individuals aged 61–80 years experiencing a higher-than-average incidence. Studies have consistently found that the mean age of stroke patients ranges from 57 to 63 years.
Males have a higher incidence of ischemic strokes across all age categories, but females over the age of 60 years have a higher incidence of ischemic infarcts. The general male prevalence in stroke was corroborated by Bogousslavsky and Regli[8] Lausanne stroke registry, with female preponderance in extreme age categories (30 and >70–80 years). In the Barcelona Stroke Registry,[9] the mean age was 64.80 ± 11.97 for males and 68.54 ± 13.92 for women. Women were more severely impacted by stroke after the age of 50–60 years, a decade later than males. It could be connected to the protective advantages of being in the reproductive age range before the age of 50 years, to women’s higher life expectancies, and to men’s earlier demise from vascular risk factors. It also agrees with research by Aiyar et al.,[10] Pinhero et al.,[11] and Eapen et al.[12] who discovered that men have strokes more frequently than women. SES also plays a role in stroke mortality, with individuals from lower SES experiencing higher rates of stroke. Several studies have shown an inverse relationship between SES and stroke mortality.
The incidence of stroke varies between urban and rural areas, with rural regions often having higher rates. Differences in stroke incidence may be influenced by the prevalence of main stroke risk factors in rural areas. Efforts to reduce stroke risk in rural areas should focus on both primordial risk factor prevention and primary risk factor control.
Ischemic stroke is the most common type of stroke, accounting for the majority of cases, followed by hemorrhagic stroke. Hypertension is present in a high percentage of stroke patients, particularly those with hemorrhagic stroke. Diabetes is also linked to an increased risk of stroke, doubling to quadrupling the chances of developing ischemic cerebrovascular disease.
Smoking and alcohol consumption are significant risk factors for stroke. Chronic heavy drinking and acute intoxication increase the risk, particularly among young adults. Elevated levels of low-density lipoprotein and total cholesterol contribute to atherosclerosis, a leading cause of stroke. Lowering plasma cholesterol levels through interventions, such as statin medication, have been shown to reduce the risk of stroke. Independent of the other cardiovascular risk factors that often go along with this condition, DM is linked to stroke. In fact, the relative risk of stroke was 3.0 for diabetes women and 1.8 for diabetic males across all age groups.[13,14]
According to Bogousslavsky et al., DM was seen in 12.6% of patients.[15] Barcelona stroke registry documented 21% of patients with diabetes among the ischemic strokes.[9] According to Kumral and Bayülkem, individuals with ischemic stroke had a diabetes prevalence of 26%.[16] The rise in the number of diabetics in our research was reflective of the Southeast Asian region’s overall rise in diabetes incidence. The incidence of stroke in the research by Nag et al.[17] was 19.5% in the hemorrhagic group and 28.8% in the ischemic group, which is comparable to our study’s 8.18% for hemorrhagic stroke patients and 30.06% for ischemic stroke patients. It boosts platelet aggregation, elevates blood fibrinogen, and raises hematocrit and blood viscosity levels. The chance of having another stroke is significantly reduced when a smoker stops smoking. Smokers are 50% more likely to get a stroke. All men and women, regardless of age, have an increased risk of ischemic stroke when they smoke. The relative risk of stroke for present and former smokers was 1.5 and 1.17, respectively, compared to nonsmokers, according to Shinton and Beevers[13] meta‑analysis. The risk of stroke is two to three times higher in smokers compared to nonsmokers. Women were more at risk for stroke than males were, and the risk increased proportionately with daily cigarette use. It is brought on by a rise in atherogenesis, a reduction in the blood’s capacity to supply oxygen, cardiac arrhythmias, and arterial spasm. In their stroke series, Bogousslavsky and Regli[8] reported that 45.6% of the patients smoked cigarettes. According to the Hamburg Stroke Data Bank, ischemic stroke patients who smoked smoked 44% of the time.[18] Similar findings were found in our investigation and these studies. In the Barcelona stroke registry, 36.2% of ischemic stroke patients smoked. In accordance with Kumral’s and Bayülkem research,[16] 28% of patients smoked. Smoking is an important risk factor in our study which is distributed among 37.4% of population but in contrast to other studies smoking is found to be not that significant (P = 0.105) risk factor for the occurrence of stroke. This might be due to uneven distribution of the study population.
The most frequent infarct site, according to Vidya and Majmudar,[19] was parietal (33.7%), followed by frontal (16.7%) and basal ganglia (10.5%). This finding was in line with research by Eapen et al.,[12] in which the parietal region (56%) was the most frequent location, followed by the basal ganglia and the frontal region. In our study, the sensitivity of clinical localization of ACS was 94.35%, specificity of 89.47%, NPV of 70.83%, and PPV of 98.32%. Similarly, the sensitivity of clinical localization of PCS was 89.47%, specificity of 94.35%, NPV of 98.32%, and PPV of 70.83%. Clinical localization is statistically significant with radiological localization.
By focusing on a tertiary care hospital setting, our study had captured data from a significant proportion of stroke cases in the region, allowing for a more comprehensive understanding of stroke epidemiology and its impact on different sociodemographic groups. This local focus enhances the applicability of the findings to health‑care providers and policymakers in the area. The study has expanded the knowledge base on clinicoradiological parameters in acute stroke patients. By examining the prevalence and characteristics of specific clinical variables, such as speech deficits, 7th nerve palsy, and sensory deficits, the research has shed light on the neurological presentations of stroke cases and their potential implications for diagnosis, treatment, and prognosis. Overall, this study has significantly added to the understanding of sociodemographic data and clinicoradiological parameters in acute stroke patients. By filling knowledge gaps and providing context‑specific insights, the research contributes to the broader field of stroke epidemiology, patient management, and stroke prevention efforts at both national and international levels.
Limitations
In patients with aphasia, altered sensorium, it was difficult to elicit the complete clinical features and neurological examination. Blinding was not done; thus, the presentation complex could be biased by the interpreter. Outcome was not measured by functional scoring systems. Moreover, it is not correlated with individual risk factors, because of the confounding nature and more than one risk factors were present in study population.
Conclusion
Cerebrovascular diseases, particularly stroke, pose a significant burden on global health. The most common stroke subtype was ischemic (54.6%), followed by hemorrhagic (42%) and SAH (3.4%). Hypertension, alcohol consumption, and dyslipidemia were the predominant risk factors. Among hemorrhagic strokes, the capsuloganglionic area had the highest distribution. The clinical localization showed high sensitivity and specificity for both anterior and PCSs. Understanding the risk factors associated with stroke, including hypertension, age, smoking, diabetes, and high cholesterol, is crucial for effective prevention and management strategies. In addition, addressing socioeconomic disparities and promoting healthy lifestyle choices can contribute to reducing the incidence and impact of stroke.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
Sri Venkatewara Medical College-SVMH/March 22, 2021.
CRediT Author Statement
Data collection – D Jennifar Evanjalin, Angel Jose, Gudluru Pujith Kumar
Data analysis – Rajasekhar G, Ketham Reddy Girish Reddy
Data curation – Ketham Reddy Girish Reddy
Manuscript writing – All authors; Proof reading -Rajasekhar G.
Data Availability
All data is contained within the manuscript.
Use of Artificial Intelligence
AI has not been used in writing the manuscript.