
Abstract
Background
Health care service utilization remains inadequate among pregnant migrants from humanitarian source countries after resettlement. A cross-sectional registry study compares the utilisation of obstetric care between migrants from humanitarian source countries (HSC) and Finnish-born (FiB) women in Finland.
Methods
Data were obtained through the medical birth registry (MBR) and the Population Information System. The sample included all births among FiB (n = 93,600) and HSC-born (n = 3,155) women in Finland in 2015–2016. The analysis included t-test, x2 test and logistic regression. Key outcome variables were birth mode, analgesia in vaginal birth, episiotomy, perineal tear, manual removal of placenta, uterine curettage, and length of stay (LOS) in the birth hospital.
Results
Caesarean delivery (CD) prevalence was higher in the HSC group compared with the Finnish-born group in elective (7.2% vs 6.5%), urgent (13.0% vs 8.9%) and emergency (1.8% vs 1.1%) procedures. In the vaginal births, episiotomy was conducted in 20.9% of the HSC and 20.6% of the FiB group (p = .755). No differences appeared in uterine curettage (0.6% vs 0.7%; p = .801). Manual removal of placenta was required less often among migrants (1.1% vs 1.8%; p = .01), whereas perineal tears were more common in this group (2.1% vs 1.1%, p < .001) compared with the Finnish-born group. Analgesia in vaginal birth was less common in the HSC group in all but one of the controlled pain relief methods. HSC group’s mean LOS in the birth hospital was 3.59 days, and FiB group’s 3.47 days (p = .004).
Conclusion
Migrant background is associated significantly with elevated CD risk, lower analgesia usage, and longer perinatal hospitalisation.
Introduction
Utilisation of health care services is suboptimal among pregnant humanitarian source country migrants in their country of resettlement. 1 This is alarming news for public-based health care systems when organising care for a new population group with an already existing risk for complex burden of physical and infectious diseases,2, 3 psychological trauma experiences,4, 5 socioeconomic vulnerability and unstable living conditions. 1 Female migrants from humanitarian source contexts can, furthermore, carry an increased risk of being exposed to conflict-related sexual violence,6, 7 female genital cut (FGC), 8 and sustain serious pre-existing gynaecological issues, such as obstetric fistula.9, 10 Therefore, it was not surprising that following the 2015 global refugee crisis, the World Health Organization (WHO) raised special worry over the sufficient delivery of health services to pregnant and birthing migrant and refugee women. 1
In light of existing literature, this worry is not in vain. Earlier studies show significant gaps in the delivery of obstetric care between humanitarian source country migrants and the receiving country-born women. Specific issues have been raised in significantly smaller provision of such care procedures as induction of labour,11, 12 pharmacological analgesia,13, 14 inhalation pain relief, 15 instrumental delivery16, 17 and episiotomy in vaginal birth. 18 Caesarean delivery (CD) rate has been reported notably higher in humanitarian source country migrants in contexts with low to moderate CD rate.17, 19–22 Alarmingly, especially urgent and emergency CDs are required significantly more often in humanitarian source country migrants’ childbirths in countries with otherwise very small need for these services.23–26
Despite the rising amount of migrant maternity care research in Europe, the WHO Regional Office states that the majority of migrant maternity care research is still conducted outside of this geographical area, and thus, the existing study results’ generalisability to the European context is questionable. 1 Many countries in the region lack population-level health service research on the humanitarian source country migrant mothers. Targeting this knowledge gap, this study investigates migration from a humanitarian source country as a potential social determinant for health care utilisation, and analyses how it is associated with obstetric care received in a setting where access to care is universal and available at very low cost to all women regardless of their residential status. The specific objectives are to compare humanitarian source country migrants and Finnish-born parturient women’s utilisation of the following obstetric care components: birth mode, analgesia in vaginal birth, episiotomy, perineal tear, manual removal of placenta, uterine curettage and length of stay (LOS) in the birth hospital.
Materials and Methods
Design
The cross-sectional study analysed medical birth registry (MBR) data, including all humanitarian source country migrants (n = 3,155) and Finnish-born women (n = 93,600) who gave birth in Finland in 2015–2016.
Setting and Data Source
Finland is a country of 5.5 million inhabitants located in Northern Europe. Obstetric care and births in the country are centred in 23 public birth hospitals. The obstetric and postpartum hospital care is mainly midwife-led, nonetheless organised with an immediate possibility to involve obstetricians, gynaecologists, anaesthesiologists and other medical specialists in the care. Out of all the births in Finland, 99.6% take place in public health care facilities, and 99.7% of the parturients have participated at least partially in the public prenatal care programme, provided free of charge to all women residing in the country. 27 All the maternity care facilities, from outpatient clinics to birth units and hospital wards, report their parturients’ prenatal and obstetric health records to the Finnish Institute for Health and Welfare, which compiles the data into a national MBR. As for all the clinical outcome measures, the data of this study were extracted from the MBR of the years 2015–2016. As for the women’s country of birth information, we utilised population register data from the Finnish Digital and Population Data Service Agency.28, 29
Population
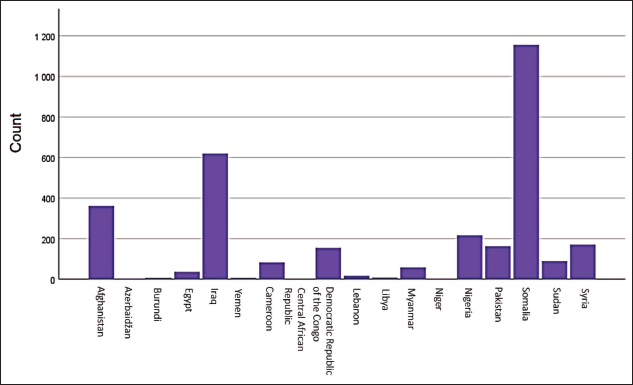
The European data protection legislation banned the registration of ethnicity and race, so we had to use the country of birth as a proxy for their origin. 30 Enabled by the Digital and Population Data Service Agency’s 29 country of birth data, we tracked from the 2015–2016 MBR data set all the births given by women (n = 3,155) who were born in altogether 18 pre-defined humanitarian migration source countries. In the definition of these humanitarian source countries (HSC), we consulted the Finnish Migration Office’s public statistics31, 32 on asylum seekers’ and quota refugees’ countries of origin, and four online humanitarian need or conflict-reporting databases.33-36 A country was listed as a humanitarian migration source country on two conditions: (a) Finland had received humanitarian migrants from the country in 2015–2019; and (b) this country was classified in two out of the four utilised databases33-36 as an area of humanitarian crisis, such as generalised conflict or serious public order disturbance. Countries of birth are presented in Figure 1.
Measures
The main outcome variables included the following clinical care procedures: induction of labour, instrumental vaginal birth, pharmaceutical and non-pharmaceutical pain relief during vaginal birth, CD, urgent or emergency CD, manual removal of placenta, episiotomy in vaginal birth, uterine curettage after vaginal birth, and perineal suturing of 3rd to 4th degree tear after vaginal birth. Furthermore, we calculated the LOS in the birth hospital in days as an additional outcome measure on health care utilisation.
To describe the participants’ background characteristics, we controlled those background variables recommended by the International Consortium for Health Outcomes Measurement (ICHOM) trackable in the utilised data set. 37 These variables were the woman’s age, height, weight, and body mass index (BMI) immediately prior to pregnancy, living with partner status, previous CD, number of previous births, anaemia, gestational diabetes mellitus (GDM), smoking, and the number of foetuses in the current pregnancy. Furthermore, we controlled the infant’s birth weight, as well as the obstetric complications, including placenta previa, breech position, other malpresentations, shoulder dystocia, placental abruption and eclampsia.
Statistical Analyses
We conducted statistical analysis on IBM version 25 SPSS Statistics© software on the prevalence of and probability (odds ratios, OR) for the selected outcome measures. In the comparison of care procedure utilisation, differences between the groups were investigated employing the t-test and χ2 test. The association of migration from a humanitarian source country and the probability of undergoing a certain care procedure, that is, the key outcome variables, was studied using bivariate logistic regression and reported as OR with 95% confidence interval (CI).
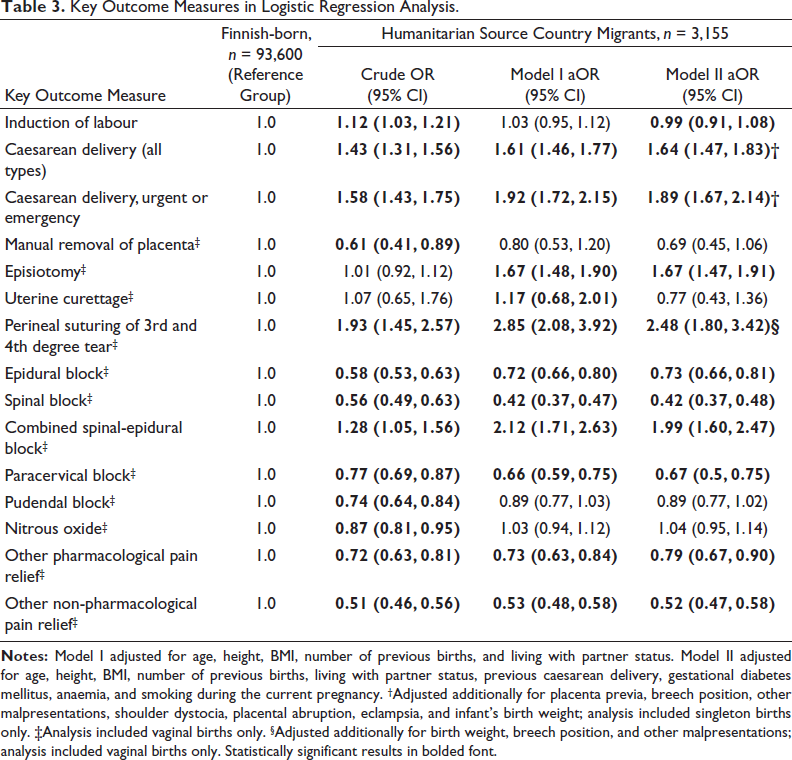
The ORs were adjusted for confounding factors: in Model I for age, height, BMI, number of previous births, and living with partner status, and in Model II for the above-mentioned, and additionally for previous CD, GDM, anaemia, and smoking during the current pregnancy. In Model II CD outcome ORs, we used only singleton births and added adjustment for placenta previa, breech position, other malpresentations, shoulder dystocia, placental abruption, eclampsia, and infant’s birth weight.37, 38 In Model II analysis, we included vaginal births only for calculating the probability of manual removal of placenta, episiotomy, all pain relief methods, and for perineal suturing of 3rd to 4th degree tear. In the probability of perineal suturing of 3rd to 4th degree tear, the OR was adjusted for birth weight, breech position, and other malpresentations. The level of statistical significance in t-tests, χ2 tests, and logistic regression analyses was considered as p < .05.
Results
Demographic Factors and Obstetric and Medical History
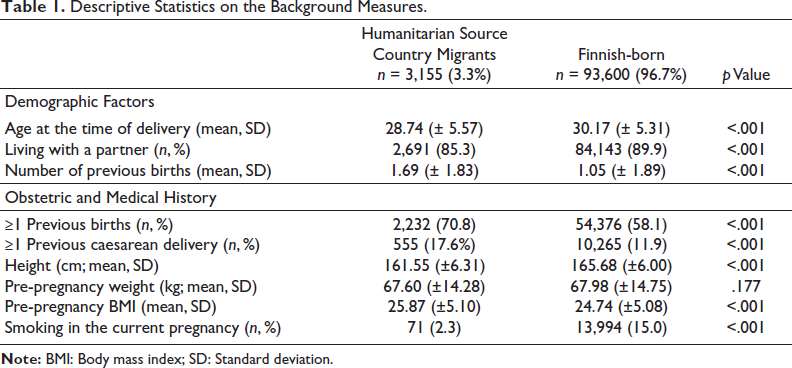
Altogether 96,755 births were included in the final analysis. Mothers born in the HSC, from hereafter referred to as the migrant group, were significantly younger with a mean age of 28.74 years (SD = 5.57), lived with a partner less often, and had more previous births (mean 1.69, SD = 1.83) than the women in the Finnish-born group. The migrant mothers also were more often parous (70.8% vs 58.1%; p < .001), and had at least one previous CD significantly more often than the Finnish-born mothers (17.6% vs 11.9%; p < .001). The mean weight prior to current pregnancy did not differ between the groups (p = .177), whereas the Finnish-born group was significantly taller in mean height (165.68 vs 161.55 cm, p < .001) and had a lower mean BMI (24.74 vs 25.87; p < .001). Smoking during the current pregnancy was reported in 2.3% of the migrant group vs 15.0% of the Finnish-born group (p < .001).
Complications in the Current Pregnancy
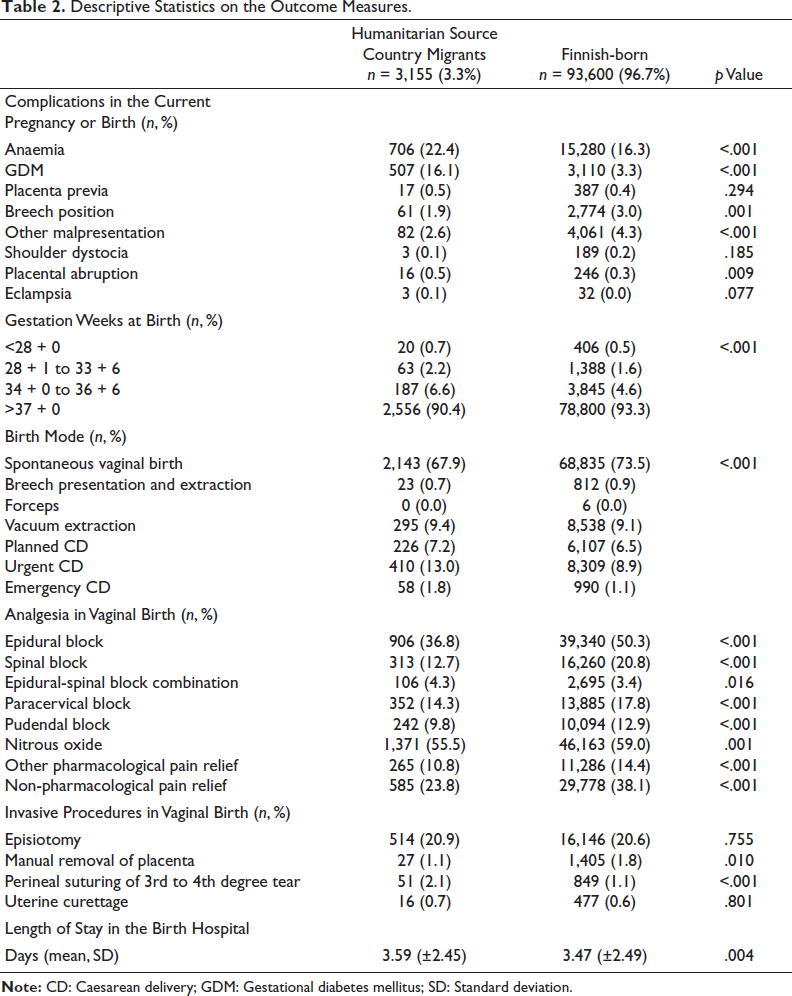
Significantly more GDM and anaemia were reported in the migrant group (p < .001), whereas breech position (p = .001) and other malpresentations (p < .001) were significantly more prevalent in the Finnish-born group. No statistically significant differences appeared in the prevalence of placenta previa, placental abruption, shoulder dystocia, and eclampsia between the groups.
Birth Mode
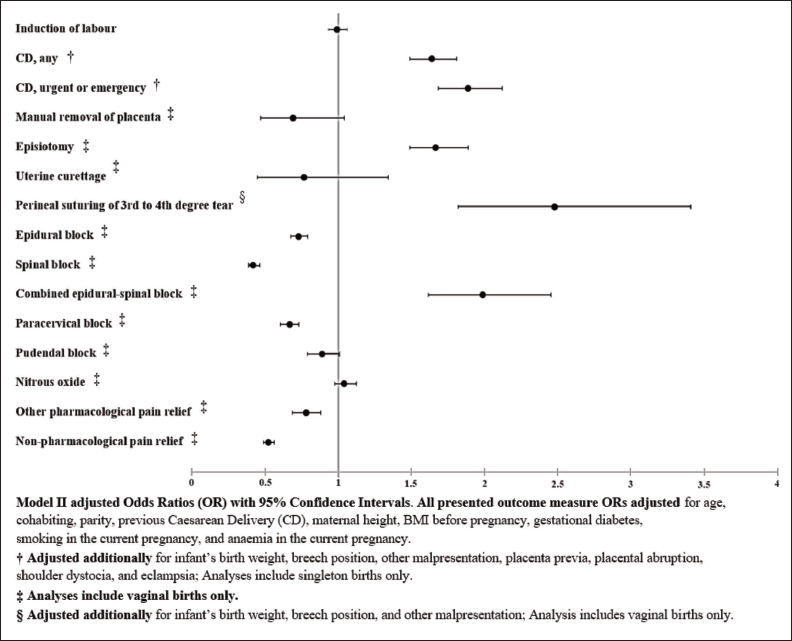
Spontaneous vaginal birth was the most common birth mode in both groups: 67.9% of the migrant women, and 73.5% of the Finnish-born women gave birth vaginally (p < .001). The migrant group had significantly higher prevalence of CD in both planned (7.2% vs 6.5%), urgent (13.0% vs 8.9%) and emergency (1.8% vs 1.1%) procedures. Compared with the Finnish-born reference group, migrant mothers’ probability was significantly elevated for any form of CD (Model II aOR = 1.64; 95% CI 1.47, 1.83), as well as for urgent or emergency CD (Model II aOR = 1.89; 95% CI 1.67, 2.14) in both unadjusted and adjusted logistic regression models.
Breech presentation and extraction in vaginal birth were reported in 0.7% of the migrants and 0.9% of the Finnish-born group, and vacuum extraction was needed in 9.4% vs 9.1% of the births, respectively. Forceps as the birth mode was an extremely rare procedure: only six births out of the total sample required this instrumental assistance, all of them reported among the Finnish-born mothers.
Analgesia in Vaginal Birth
Significant differences emerged in all controlled pain relief methods between the comparison groups. The Finnish-born group had a notably higher usage percentage in epidural, pudendal, paracervical and spinal blocks, and in the use of inhalable nitrous oxide, other pharmacological and non-pharmacological pain relief methods. The Model II aOR in the migrant group was 0.73 (95% CI 0.66, 0.81) for epidural; aOR = 0.42 (95% CI 0.37, 0.48) for spinal; aOR = 0.67 (95% CI 0.59, 0.75) for paracervical, and aOR = 0.89 (95% CI 0.77, 1.02) for pudendal block. For nitrous oxide usage among the migrant women, the aOR was 1.04 (95% CI 0.95, 1.14), for other pharmacological pain relief, the aOR was 0.78 (95% CI 0.67, 0.90), and for non-pharmacological pain relief methods aOR = 0.52 (95% CI 0.47, 0.58). Combined epidural-spinal block was the only analgesia method more commonly used in the migrants’ group (4.3% vs 3.4%; aOR = 1.99; 95% CI 1.60, 2.47).
Invasive Procedures in Vaginal Birth
Approximately one-fifth of both groups underwent an episiotomy in vaginal birth (20.9% vs 20.6%; p = .755). The probability for episiotomy was significantly higher in the migrant group (aOR = 1.67; 95% CI 1.47, 1.91). No differences appeared in uterine curettage (0.6% vs 0.7%; p = .801). Manual removal of placenta was required more often in the Finnish-born women’s births (1.8% vs 1.1%; p = .01), whereas 3rd and 4th degree tears requiring perineal suturing were more common in the migrants’ group (2.1% vs 1.1%; aOR = 2.48; 95% CI 1.80, 3.42).
Table 1 compiles the descriptive statistics on the population’s background measures, and Table 2 on the outcome measures. Table 3 presents the results of logistic regression analysis on the outcome measure’s association with migration from a humanitarian source country. A concise illustration of the key findings is presented in Figure 2.
Descriptive Statistics on the Background Measures.
Descriptive Statistics on the Outcome Measures.
Key Outcome Measures in Logistic Regression Analysis.
Outcome Measures and Association with Migration from a Humanitarian Source Country.
LOS in Birth Hospital
The mean LOS in the birth hospital was 3.59 days (SD = 2.45) among the migrant women, and 3.47 days (SD = 2.49) among the Finnish-born women (p = .004). Migrant women’s Model II aOR for hospital stay of less than three days was 0.77 (95% CI 0.71, 0.84), difference remaining significant when adjusted additionally for gestation weeks, birth mode and infant’s birth weight (aOR = 0.90, 95% CI 0.81, 0.99). With the same adjustments, a slight yet significant difference was found between the comparison groups in the migrant women’s higher probability of 3–6 days’ hospital stay (aOR = 1.13; 95% CI 1.03, 1.23), but not in the hospitalisation time of more than seven (aOR = 1.09; 95% CI 0.92, 1.30), and more than 14 days (aOR = 1.15; 95% CI 0.69, 1.92).
Discussion
This study presented a cross-sectional comparison of the obstetric care of migrants from HSC and Finnish-born women given birth in Finland in 2015–2016. Our analysis of 96,755 births revealed significantly higher quantity and probability for the migrant women for CD as the birth mode, and for episiotomy and perineal suturing of 3rd to 4th degree tear in vaginal birth. On the contrary, the migrant group had utilised significantly less often all but one of the monitored pain relief methods compared with the Finnish-born women.
Considering the migrant group’s shorter mean height, the more probable previous CD, and the notably higher prevalence of GDM, and the earlier reported sexual and reproductive issues such as FGC 39 —all known risk factors for CD, it was not surprising that the CD prevalence emerged significantly elevated among the humanitarian source country migrants, also in our data. The migrant group’s total CD percentage, as well as the OR for CD, appeared somewhat similar in our data as in the recent reports comparing the general population and migrant women from a typical HSC. Report by Wanigaratne et al. 19 had compared refugee immigrants with Canadian women in Canada, and found slightly elevated risk for CD in the first-mentioned group (aOR = 1.04; 95% CI 1.00, 1.08). Nearly identical findings had been found in Trinh et al., 20 comparison of Sub-Saharan African migrants’ and Australian non-indigenous women’s probability for CD (aOR = 1.08; 95% CI 1.00, 1.17). From contexts geographically closer and societally more similar to the present study, Juárez et al., 23 Liu et al., 17 Bakken and Stray-Pedersen 25 , Eslier et al., 21 Bastola et al. 26 and Mæland et al. 40 have presented CD findings very similar to ours, indicating the results’ generalisability to the European context, as called for in the WHO report. 1
The women in our humanitarian source country migrants’ sample had received significantly less often pharmacological and non-pharmacological analgesia in vaginal birth than the Finnish-born comparison group. The inspection of earlier literature does not make this finding surprising. Studies with a similar type of comparative cross-sectional design have reported aligned results on migrants’ lower utilisation of birth analgesia from Germany, 14 Australia,18, 41 the UK, 42 Sweden,43–45 Israel, 46 Spain,13, 47 Finland 15 and Norway 48 .
Interestingly, the migrant women in our sample had significantly higher usage of combined epidural-spinal block analgesia. This could potentially result from at least two reasons. First, a combined epidural-spinal block is a widely preferred anaesthesia method for possible CD, 49 and thus, with the higher probability for initially induced vaginal birth ending up in urgent or emergency CD, the migrant women in our sample could have received a spinal catheter if there had been obvious danger signs for obstructed or prolonged labour, leading potentially to urgent or emergency CD. Second, administering any of the monitored analgesia methods requires an understanding of oral instructions to some extent, and the birthing woman’s ability to cooperate accordingly. In a context in which both migrant women50, 51 and midwives 52 have earlier reported on language barrier hindering the sufficient delivery of obstetric care, it can be hypothesised whether this has been a contributing factor in the analgesia utilisation among the present study’s sample. Consequently, preference for one effective analgesia method with possibilities for quick onset and re-dosage 49 can have limited the number of pain relief choices offered to, or chosen by, the migrant women, which might have been seen as a partial solution for both the discussed problems, even though no clear evidence on this method’s superiority exists. 53
The third potential reason for fewer analgesia methods could be women’s preference not to utilise the offered pain relief methods. Little published data on migrant women’s birth preferences in the country of resettlement exists to date. In Sheridan et al., 54 samples of 632 women, parturients of Nigerian origin living in Ireland, had preferred significantly more often an analgesia-free birth plan than the Irish comparison group. 54 Therefore, it is noteworthy that this study had no possibility to examine what the women themselves would have wished for their births, and how these wishes were taken into account by the care professionals. Such an investigation would require a more complicated methodology, and yet it would be difficult to capture whether the personal wishes or the medical needs would be the most suitable indicator for judging successful delivery of obstetric care. A notable issue for further research is also to question whether or not the country-born women would represent a ‘desirable standard for populations to strive toward’. 55
Strengths and Limitations
The Finnish MBR’s suitability for maternity care research purposes is recognised and discussed in a recent review article, 56 enforcing the relevance of these data for research questions and methodology in our study. The utilised data set consists of mandatorily reported maternity care measures and outcomes throughout the population. 57 The good data accuracy and high coverage can minimise the risks of underreporting and sampling bias, whereas the large sample size ensures good statistical accuracy. 58 As a limitation, our study was not able to include irregular migrants from HSC, as the MBR data do not include individuals with no valid person number. Also, our methods did not allow controlling of the parturient women’s education and income level, or the parturient’s personal knowledge and attitudes towards birth. In addition to the confounding factors controlled in our analyses, these are all considerable issues influencing potentially in the birth mode,17, 38, 59 and usage of pain relief methods during birth.60–62
Conclusion
The present MBR study provides evidence that even after adjusting for multiple physical and sociodemographic variables, significant differences in the performed obstetric care procedures among the country-born and foreign-born women’s births exist. Recommendation for further research is to investigate deeper the underlying mechanisms and reasons for these observed differences in care utilisation.
Footnotes
Acknowledgement
The authors wish to thank Matti Estola, PhD, for the assistance in statistical analysis.
Authors’ Contributions
The design of the study and the decision on the statistical tests were mutually agreed upon by all authors. Mika Gissler responded to the merging of the DVV population registry data with the MBR data, and prepared them for the analysis conducted by Satu Leppälä in collaboration with the faculty statistician. Satu Leppälä prepared the initial text for the article, which Reeta Lamminpää, Mika Gissler and Katri Vehviläinen-Julkunen commented on and edited. All authors contributed to and accepted the final text.
Data Statement
The Finnish register data have been given for this specific study, and the data cannot be shared without authorisation from the register keepers. More information on the authorisation application for researchers who meet the criteria for access to confidential data can be found at
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
An institutional review board, the Hospital District of Northern Savo Ethics Committee, granted ethical approval (decision number 254/2017) for the study prior to registry data application. For the registry data usage, additional research permits were received from the Finnish Institute for Health and Welfare (THL/1105/5.05.00/2019) and Finnish Digital and Population Data Service Agency (DVV/899/2020-3).
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study received funding from the Finnish Cultural Foundation North Savo Regional Fund (grant number 65191875), from the Finnish Concordia Fund, and the University of Eastern Finland, Department of Nursing Science. The funding sources did not participate in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Informed Consent
This was a register-based study, which does not require patient consent in Finland.