
Abstract
Aim
National guidelines in Sweden suggest that certain ‘priority’ groups of pregnant women, including women with fear of childbirth (FOC), may benefit from increased continuity in midwifery care. Although comorbidity indeed exists between FOC and mental health problems, it might also be mediated by individual resources. The purpose of the study was to identify profiles of women based on FOC, depressive symptoms, major worries and sense of coherence (SOC) and to study those profiles in relation to women’s perceptions of changes occurring during pregnancy.
Methods
A longitudinal cohort study was conducted on 171 pregnant women with FOC or depressive symptoms in a rural area of Sweden, whose care was following a midwifery continuity of care (MCoC) model. After collecting data using two online questionnaires (in mid-pregnancy and 2 months after birth), addressing background and including validated instruments measuring FOC, depressive symptoms, major worries and SOC, a k-means cluster analysis was conducted to define profiles of women.
Results
The three identified clusters: Emotionally healthy, Fearful with resources and Emotionally fragile, showed no differences in socio-demographic background or type of MCoC model. However, major differences did emerge in women’s feelings and perceptions of changes during pregnancy, along with minor differences in health-related variables. Women in the Emotionally fragile cluster had less positive scores for most questionnaire items.
Conclusion
The results indicate levels of vulnerability within certain priority groups. In response, healthcare professionals should examine pregnant women’s backgrounds beyond screening in order to more fully understand their emotional states.
Introduction
Pregnancy is a period when physical, emotional and social changes occur and when both facilitators and barriers affect women’s well-being in general, and especially affect their emotional health. One such facilitator is the sense of coherence (SOC), a major construct in salutogenic theory that reflects how people view the world and cope with life’s stressors. For example, people with a high level of SOC tend to view the world as being manageable, comprehensible and meaningful. Investigated in various populations, SOC has been described as a stable personality disposition.1, 2
In studies on SOC in relation to pregnancy, a systematic review of 34 scientific articles showed inconsistencies in pregnant women’s socio-demographic background factors and SOC, particularly regarding parity, country of origin, level of education and income level. The review also revealed that lower SOC is associated with increased parental stress, depressive symptoms, fear of childbirth (FOC) and post-traumatic stress disorder. 3
At the same time, some inconsistencies have been observed in the trajectory of SOC during pregnancy and the early postnatal period. In one study, a statistically significant increase in SOC from the antenatal to postnatal period was found to be associated with high-birth satisfaction, whereas decreased SOC was associated with epidural anaesthesia, assisted vaginal births and low-birth satisfaction. 4 By contrast, a study from Sweden investigating SOC from pregnancy to a year following birth showed that women’s SOC was unstable during pregnancy, improved after birth, but subsequently worsened 12 months later. 5
FOC, a possible barrier to health and well-being, affects 14% of all women worldwide. 6 A systematic review of 21 studies aiming to detect causes and outcomes of FOC and concluded that stress, anxiety, depression and lack of social support were associated with the fear during pregnancy. However, no strong associations between FOC and demographic variables were detected. Although the key predictors of FOC relate to negative birth experiences and operative births in the past. 7
Depressive symptoms and major worries might also be signs of poor emotional well-being and may co-occur with FOC.8, 9 In populations with FOC, depressive symptoms have been estimated at 32%, 10 and are found in association with low antenatal attachment and limited positive mother–child bonding. 11 Another important barrier to maternal well-being is experiencing major worries, with the most reported worries during pregnancy being about the baby’s health, giving birth, being admitted to the hospital and the risk of miscarriage.12, 13
In Sweden, antenatal care is provided at outpatient clinics within the primary health sector, with midwives as the main caregivers. The uptake of antenatal care in the country is nearly 100%. For uncomplicated pregnancies, eight to nine visits to the midwife are recommended, 14 and the midwife is to consult an obstetrician in cases of complications. Nearly all births occur in hospital-based labour wards, where midwives are independently responsible for uncomplicated births and work in collaboration with obstetricians in case of complications. For women with severe FOC, all Swedish hospitals offer 2–4 counselling sessions from midwives. 15 When other mental health problems are present, a referral to a psychologist or psychiatrist is recommended.
Midwifery continuity of care (MCoC) models are rare in Sweden despite evidence of their benefits for women and their babies. 16 Moreover, recent national guidelines in Sweden suggest that MCoC models should be offered to certain ‘priority’ groups, including women with language barriers, FOC and/or psychosocial vulnerability. 17
Aim
Research on women’s emotional well-being has shown that some women who suffer from FOC also have depressive symptoms, anxiety and/or major worries. From a salutogenic perspective, SOC may mediate the influence of fear, anxiety, worries or depressive symptoms; however, knowledge of their interrelationships remains limited. In response, in our study we aimed to identify profiles of women based on FOC, depressive symptoms, major worries and SOC, and to study those profiles in relation to various background- and health-related variables.
Methods
Design
A longitudinal cohort study was designed for pregnant women whose care followed an MCoC model with two options during a 2-year period.
Participants
Pregnant women with FOC or depressive symptoms were recruited at week 20th of gestation and followed up 2 months after birth.
Setting and Procedure
The study was conducted during 2022–2024 in a rural area near a mid-sized city in Sweden. During the study period, the only labour ward in the area was located in the city, and some women had to travel up to 250 km to give birth. There were 29 clinics in the area that provided antenatal care, and the annual birth rate at the hospital was approximately 2,600.
At week 20 of gestation, all pregnant women in the region are offered screening at their designated antenatal clinics, which aim to identify symptoms of FOC and depressive symptoms. FOC is measured using the Fear of Birth Scale (FOBS),18, 19 while the Edinburgh Postnatal Depression Scale (EPDS) 20 is used to detect depressive symptoms. Cut-off values of 60 points on the FOBS and 13 points on the EPDS were used as indicators of FOC and depressive symptoms, respectively. Women who met those criteria were informed about the study and asked if they were interested in following the MCoC model.
The MCoC model offered two options. One option was to receive all remaining care with a group of midwives who could provide continuity of care via physical meetings at the antenatal clinic in the family centre and on-call assistance during labour and birth. In the other option, women residing far from the city could continue to receive antenatal care from a local midwife closer to home, and in addition, have video calls and assistance with births with the MCoC midwives. Groups following either option were offered online parent education classes and counselling for FOC, with the number of counselling sessions based on the women’s needs. All participating women also completed a follow-up meeting at the hospital with the on-call midwife on the day after the birth and a digital follow-up 5 days later.
Data Collection
Women consented to participate in the longitudinal study by completing an online questionnaire anonymously shortly after enrolment (background data), and a follow-up questionnaire 2 months after birth (women’s perceived changes and feelings during pregnancy). Women who consented received a personal code from a local project leader to gather their follow-up responses. A secure online platform, REDCap, was used to collect data.21, 22
Questionnaires
Data about demographic background (e.g., age, civil status, country of birth, level of education and option of MCoC model) were collected using the first questionnaire, as were health- and pregnancy-related data regarding chronic diseases, self-rated physical and emotional well-being, and whether any help for mental health conditions had ever been received. The pregnancy-related questions concerned parity, whether the pregnancy was planned or welcomed, assisted conception and preferred mode of birth. By contrast, the second questionnaire, completed 2 months after birth, contained a battery of questions addressing women’s perceived changes and feelings during pregnancy, all assessed on seven-point Likert scales.
Instruments Used in Cluster Analysis
Women’s emotional well-being was additionally assessed using four validated instruments included in the first questionnaire. First, FOC was investigated using the FOBS,18, 19 which consists of two 100 mm visual analogue scales anchored by calm/worried and no fear/strong fear. Participants were asked to respond to the question ‘How do you feel right now about the approaching birth?’ and were instructed to place a mark on the two scales. Cronbach’s alpha for the two items in our study was 0.903.
Second, depressive symptoms were assessed using the EPDS, 20 which contains 10 items concerning depressive symptoms. Participating women were instructed to refer to their feelings from the previous week while answering each item on a four-point Likert scale ranging from 0 to 3, and total scores ranging from 0 to 30.
Third, the 16-item Cambridge Worry Scale (CWS), 23 was used to identify sources of the women’s worries. The 16 items address worries about housing, finances, health, work, childbirth, the risk of miscarriage, admittance to hospital, giving birth, and caring for the infant. Each item is assessed on a scale ranging from 0 to 5, and all 16 items are totalled to form a continuous variable ranging from 0 to 80.
Fourth and finally, the 13-item (SOC scale2) was used to gauge the women’s personality and resourcefulness. Addressing the three dimensions of comprehensibility, manageability and meaningfulness, the SOC scale’s 13 items are assessed on numerical scales ranging from 1 to 7 and totalled to give a total score ranging from 13 to 91. 2
Analysis
The participants’ background data were documented using descriptive statistics (i.e., n and %). Women’s level of FOC, depressive symptoms, worries and SOC was assessed on continuous variables that were transformed into z scores. A k-means cluster analysis was conducted on the four instruments to identify subgroups or profiles of women within the cohort. In general, cluster analysis serves to group data based on similarities and homogeneity within clusters and heterogeneity between clusters. 24 No formal statistical criteria were applied to determine the number of clusters. Instead, two-, three- and four-cluster solutions were tested, and the three-cluster solution was selected based on its conceptual clarity and the interpretability of the resulting clusters. The clusters were labelled according to the grouping and the direction of the four scales.
FOBS scores, EPDS scores, CWS scores and SOC scores were documented in terms of the mean, standard deviation (SD), and the range between the minimum and maximum. Following cluster formation, differences between the clusters were examined using chi-square tests for categorical background variables and one-way analysis of variance (ANOVA) for each continuous variable separately. Women’s perceptions about changes and feelings during pregnancy were analysed using ANOVA as well. All p values less than .05 were regarded as being statistically significant.
To assess the robustness of the cluster solution and group comparisons, several sensitivity analyses were conducted. Alternative cluster solutions were explored, and while some variation in cluster composition was observed, the overall patterns of differences between groups remained consistent. Non-parametric alternatives (Kruskal–Wallis and Fisher’s exact test) were used to confirm the findings from ANOVA and chi-square tests, which did not alter the results.
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for observational studies was followed, and the study was approved by the ethical board [DNR information removed for peer review].
Results
A total of 171 women participated in the study and completed both the background questionnaire and the four instruments (i.e., FOBS, EPDS, CWS and SOC) that formed the basis for cluster analysis. Missing data were minimal across background variables, with zero to one missing items on a few variables. All available data were used in the analyses, and no imputation was applied.
Figure 1 shows the standardised mean scores (z scores) of variables for the four included measures (FOBS, EPDS, SOC and CWS) across the three identified clusters. Values on the y-axis represent SDs from the sample mean. Positive values indicate above-average scores and negative values indicate below-average scores.
Clusters Based on Fear of Childbirth (FOC), Edinburgh Postnatal Depression Scale (EPDS), Cambridge Worry Scale (CWS) and Sense of Coherence (SOC).
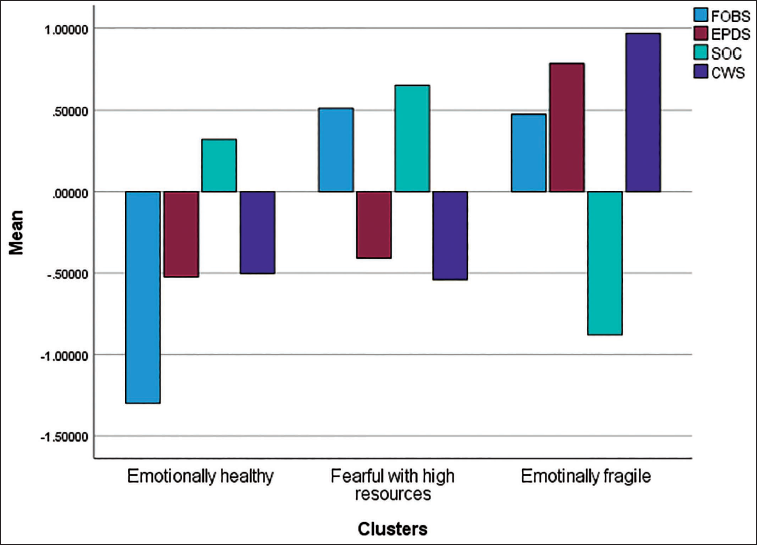
As shown in Figure 1, the first cluster, labelled Emotionally healthy, included 47 women (27.5%); the second, labelled Fearful with resources, included 64 women (37.4%); and the third, labelled Emotionally fragile, included 60 women (35.1%). The Emotionally healthy cluster had below-average scores for fear, depressive symptoms and worries and a slightly above-average SOC score, whereas women in the Fearful with resources cluster showed elevated levels (above-average) of FOC, low levels (below-average) of depressive symptoms and worries and an above-average level of SOC, suggesting they experienced some emotional distress but perceived themselves as having coping resources. Last, the Emotionally fragile cluster had elevated levels of fear, worries and depressive symptoms and a markedly below-average SOC, indicating higher emotional vulnerability and fewer perceived resources.
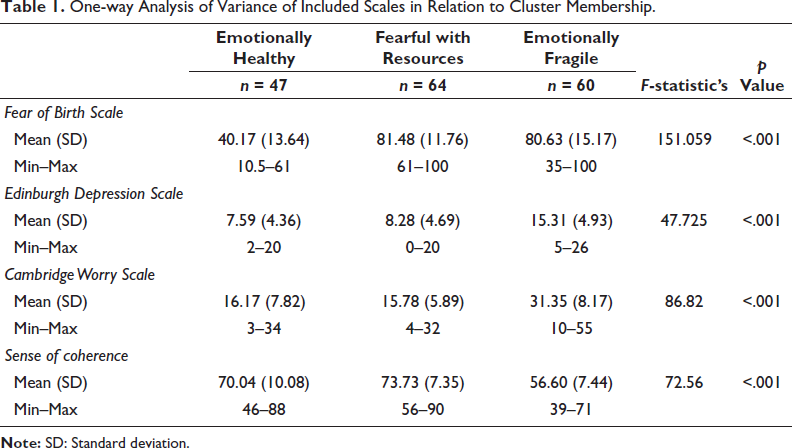
Table 1 presents detailed information about the participants’ scores on the scales in relation to the clusters. Statistically significant differences emerged between all scales and clusters. The Emotionally fragile cluster had the highest levels of depressive symptoms and worries, but the lowest levels of SOC. Meanwhile, the Fearful with resources cluster had the highest FOBS score.
One-way Analysis of Variance of Included Scales in Relation to Cluster Membership.
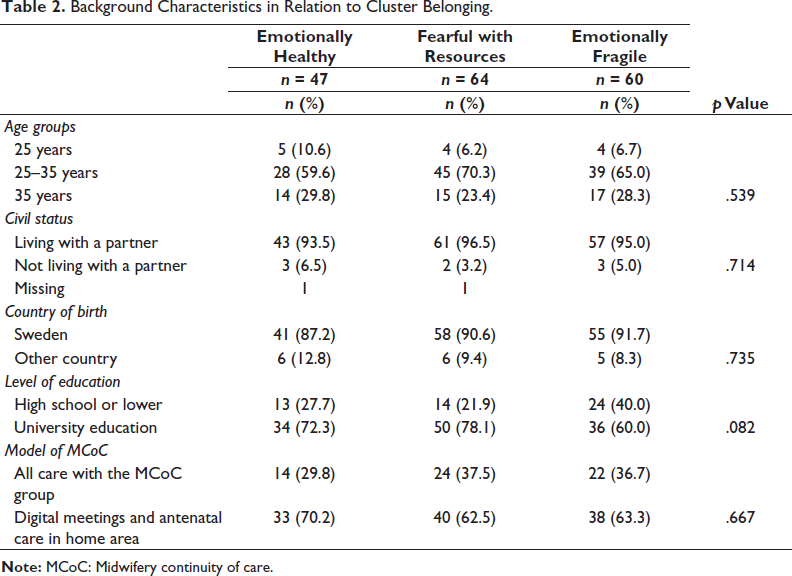
Next, Table 2 shows the background characteristics of women in each cluster. Most women were 25–35 years old (65%), living with a partner (95%), and born in Sweden (90%). Women’s levels of education were high, with 70% having earned a university education. Regarding the option of the MCoC model, 65% opted for the digital model, whereas 35% received in-person care at the antenatal clinic. No statistically significant differences in background characteristics surfaced between the clusters.
Background Characteristics in Relation to Cluster Belonging.
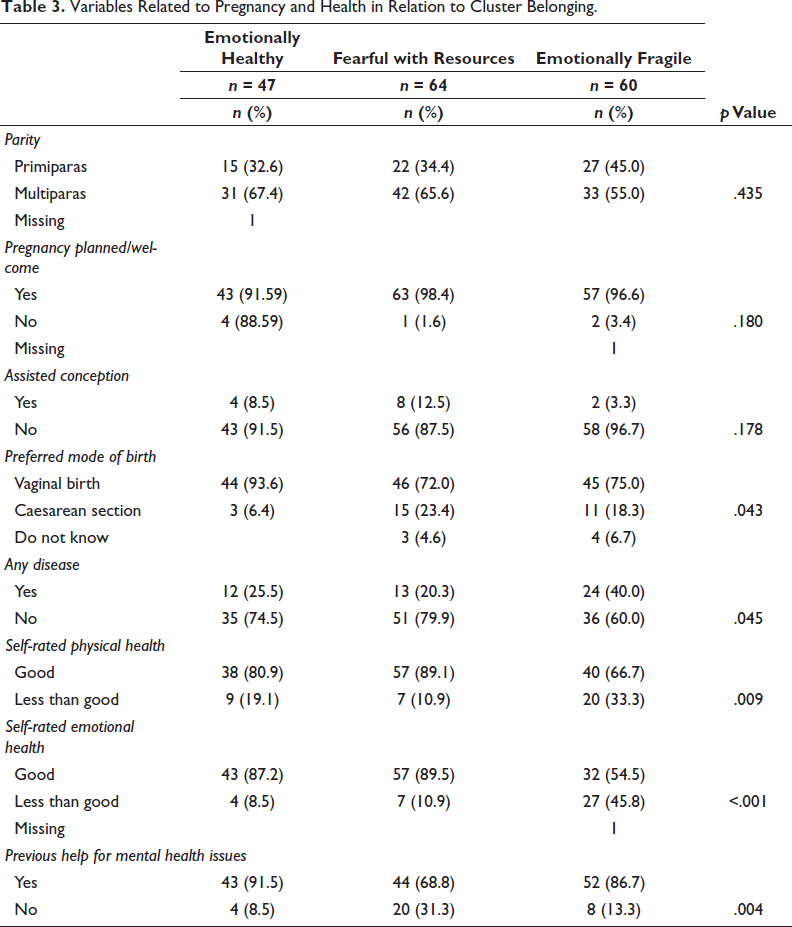
As Table 3 shows, most women were multiparous (63%), and nearly all women stated that their current pregnancy was planned or welcome (96%). Eight per cent had assisted conception, and 18% preferred to receive a caesarean section. No statistically significant differences emerged between the clusters regarding pregnancy-related variables. Table 3 also shows that nearly one in three women reported having a disease—most commonly anxiety, asthma, depression and pregnancy-induced diabetes. Although most women reported good physical (78%) and emotional (77%) health, statistically significant differences emerged between the clusters and their reported health, with women in the Emotionally fragile cluster being more likely to report poor health. Meanwhile, 80% of women had previously received help for mental health conditions, and, on that count, there was a statistically significant difference between the clusters. The most previously reported form of help was counselling (79%), followed by seeing a psychologist (70%), seeing a social worker (51%), having medication (46%) and seeing a psychiatrist (21%).
Variables Related to Pregnancy and Health in Relation to Cluster Belonging.
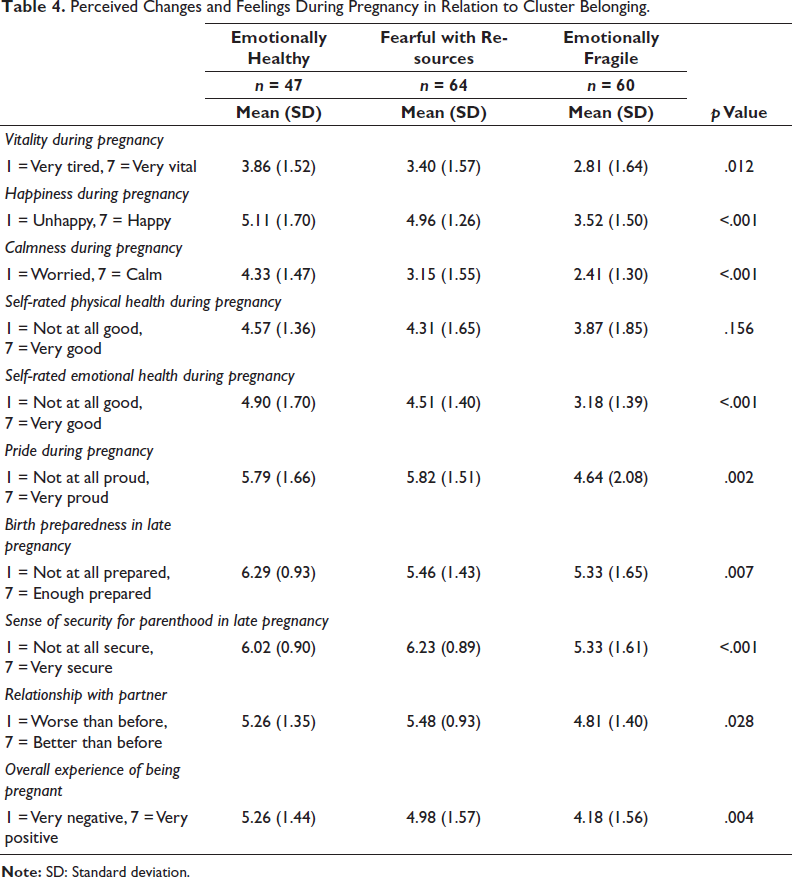
Last, Table 4 presents the results for items addressing women’s perceived changes and feelings during pregnancy. All items were assessed on seven-point Likert scales, and the highest rankings (i.e., most positive) emerged for a sense of security with parenthood (M = 5.87, SD = 1.24), birth preparedness (M = 5.60, SD = 1.50) and pride (M = 5.41, SD = 1.81). The lowest scores, by contrast, were for self-rated emotional health during pregnancy (M = 4.15, SD = 1.65), vitality during pregnancy (M = 3.32, SD = 1.62), and calmness during pregnancy (M = 3.13, SD = 1.59). Statistically significant differences arose between all items except for the assessment of physical health during pregnancy, and women in the Emotionally fragile cluster scored lowest on all items.
Perceived Changes and Feelings During Pregnancy in Relation to Cluster Belonging.
Discussion
The main finding of this study was that the profiles of women based on cluster analysis did not show any differences in background characteristics, but rather showed obvious differences in their self-reported health and their perceptions of changes and feelings about pregnancy.
Cluster analysis resulted in three clusters labelled according to the direction of the four scales. The labels were somewhat similar to those developed in past studies. The Emotionally healthy cluster in the present study was somewhat equivalent to a cluster in another study on women receiving care following an MCoC model. 25 In that study, only two clusters were identified based on SOC scale scores, EPDS scores, CWS scores and FOC. The difference between that study and the present study was that the other study included a question on women’s feelings about the approaching birth as a proxy for FOC, 26 which was assessed on a five-point Likert scale ranging from ‘Very positive’ to ‘Very negative’. Findings representing the Emotionally fragile cluster, which included 35% of the pregnant women in our study, resembled the findings for an equivalent cluster in a previously mentioned study. 25 Those findings, based on data from a regional cohort study and a national cohort study using nearly the same instruments, showed a similar prevalence of 35% of women, indicating different levels and nuances of fragility or vulnerability among women who present with FOC or poor mental health.
The other two clusters were inspired by a study of 1,419 women involving a cluster analysis using the Hospital Anxiety and Depression Scale (HADS)-Anxiety, HADS-Depression, FOBS-Worry, FOBS-Fear and the Self-Efficacy Scale. 27 The four clusters in that study were labelled ‘Resourceful–robust’, which had low levels on the HADS scales and the FOBS, and elevated levels of self-efficacy; ‘Resourceful–fearful’, which had moderate levels of all measures; ‘Vulnerable–fearful’, which had no symptoms of depression or anxiety but high levels of fear and somewhat decreased levels of self-efficacy; and the ‘Fragile–fearful’, which had elevated levels of fear, anxiety and depression and low levels of self-efficacy. Compared with the clusters in that study, the Fearful with resources cluster was somewhat similar to the Fearful–resourceful cluster, while our Emotionally fragile cluster corresponded to the Fragile–fearful cluster. 27 Although SOC and self-efficacy may not measure exactly the same thing, both constructs have, nevertheless, been used as proxies for personality.
Beyond that, no differences have emerged between the clusters in their background characteristics or pregnancy-related variables. However, statistically significant differences did surface between the clusters regarding the assessment of their health and feelings, and their perceptions of their pregnancies, with women in the Emotionally fragile cluster presenting the most negative findings. Interestingly, women in the Emotionally healthy cluster were most likely to have sought or received help for their mental health condition (91%), and women in the Emotionally fragile cluster also reported a high degree of help-seeking (87%). Their profiles differed nonetheless, and learning which aspects made treatment successful would be worthwhile, for example, by conducting a qualitative study with in-depth interviews.
The lack of between-cluster differences in background characteristics and pregnancy-related variables raises the question of how women who need additional support, sometimes called ‘vulnerable groups’, can be identified and defined. Vulnerable groups or ‘priority groups’, as worded by Bradford et al., 28 can be identified based not only on socio-economic status, which is often primarily considered in efforts to help certain groups. In a systematic review, 28 31% of 175 MCoC initiatives were directed towards ‘priority groups’, meaning women living in rural or remote areas, Indigenous women, young women, women from socially deprived areas, refugees and immigrants. 28 Women with FOC are not always included in priority groups when it comes to receiving MCoC; however, from a Swedish perspective, their inclusion in such care is strongly advised. Indeed, the Swedish National Board of Health and Welfare 17 has recommended that the introduction of MCoC models should be directed towards priority groups in research projects before being implemented at the national level. What is also discovered from the cluster analysis is that levels of vulnerability exist and that women’s feelings and perceptions of their pregnancies differ from cluster to cluster, which can alter their level of vulnerability. For those reasons, women’s emotional states and feelings should also be taken into account when offering MCoC to so-called priority groups.
As for limitations, the findings should be interpreted in light of the study’s observational design, the self-reported nature of the data and the rather small sample. It was impossible to randomise women to the two MCoC models due to the project’s short time frame, the limited number of women in the target group, and allowing the women to choose their type of MCoC model. Moreover, no differences surfaced between the clusters or options for MCoC models in the study, likely due to the inclusion criteria and the screening procedure.
Despite these limitations, the findings are in the same direction as other studies that have used similar instruments to perform cluster analysis.
The three-cluster solution was selected based on conceptual clarity and interpretability. Compared to two- and four-cluster solutions, it offered more distinct and meaningful groupings. Sensitivity analyses confirmed that the overall pattern of results was robust and remained stable when alternative statistical tests were applied.
However, it should be noted that cluster analysis involves certain subjective decisions, including the choice of the number of clusters and included variables. While we tested alternative solutions and found consistent patterns, the final cluster solution should be interpreted with this inherent subjectivity in mind. Cluster analysis is foremost a method that is not inferential, and therefore, no conclusions can be drawn for a general population.
As for the study’s strengths, validated instruments were used as a basis for cluster analysis, and those instruments could also be used for comparisons with similar studies. After all, the FOBS and EPDS are commonly used in clinical practice as screening tools to detect FOC and depressive symptoms, respectively. Beyond that, follow-up studies are needed to examine the birth outcomes for the clusters as a means to increase knowledge of birth outcomes’ usefulness for health care practitioners.
Clinical Implications
Health care practitioners should be aware that women with FOC/depressive symptoms are not a homogeneous group. It is therefore important to thoroughly investigate pregnant women’s emotional state during health care visits. Midwives have a good opportunity to provide the best evidence-based care.
Conclusion
Because the results indicate levels of vulnerability within priority groups, and because other research has shown that mental health vulnerabilities might affect not only women but also their children in both the short and long term, healthcare professionals should examine pregnant women’s background beyond screening, in order to more fully understand their emotional states.
Footnotes
Authors Contribution
All authors contributed to the conception and design of the study, design of the survey, analysis and interpretation of the data. Data were collected online. The first draft of the manuscript was written by Ingegerd Hildingsson, and all authors participated in drafting and revising the manuscript and approving the final version submitted.
Data Availability
Data are available upon request.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study received ethical permission from the Swedish ethical committee (DNR 2021-0194). In the article, the DNR has been anonymised, but will be inserted if published.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained in writing from all individual participants included in the study.