
Abstract
Introduction
Teamwork is considered as an effective strategy in the provision of quality patient care, including the prevention of mother-to-child transmission (PMTCT) of human immunodeficiency virus (HIV). Multidisciplinary teamwork (collaborative practice) among healthcare workers has been widely accepted as a source of optimising healthcare provision and improving patient safety. The World Health Organization (WHO) has endorsed the need to establish effective teamwork within healthcare settings, in a quest to address the challenges of fragmented health systems, to improve the utilisation of an efficient and effective workforce and to deliver high-quality patient care. We aim to understand the key contributory factors in establishing effective multidisciplinary teamwork among healthcare workers in providing PMTCT services to HIV-positive pregnant women and their infants.
Methods
Data were collected using in-depth interviews. Interviews were conducted in the three tertiary hospitals and associated health clinics in Fiji between April–May 2013 and February–March 2014. Ethical approvals were obtained. A total of 58 healthcare providers were interviewed, including doctors (n = 12), midwives (n = 19), nurses (n = 14), laboratory technicians (n = 5) and counsellors (n = 8). The data were analysed using thematic analysis.
Results
We found that multidisciplinary teamwork was an overarching theme, followed by three sub-themes in discussing what constitutes effective multidisciplinary teamwork among these healthcare providers in delivering PMTCT services to HIV-positive pregnant women and their infants. The three sub-themes included integration of PMTCT services, effective communication and supportive colleagues.
Discussion
Our findings would be useful in developing strategies to foster teamwork and improve working relationships between healthcare workers in other similar settings.
Keywords
Introduction
Teamwork among healthcare workers is considered as an effective strategy in the provision of quality patient care, leading to improved health outcomes, provider satisfaction and efficient use of organisational resources.1–5 The World Health Organization (WHO) has endorsed the need to establish effective teamwork within healthcare settings, 6 in a quest to address the challenges of healthcare systems. The WHO recommends developing specialised multidisciplinary teams consisting of healthcare workers from different professional backgrounds (e.g., physicians, nurses, midwives and other related healthcare workers) working together and utilising a wide range of skills and knowledge to improve the utilisation of an efficient workforce and deliver high-quality patient care.6, 7 Other interchangeable terms have been widely used to refer to teamwork among healthcare workers, such as interprofessional collaboration, 8 interprofessional teamwork, 5 collaborative practice 9 and multidisciplinary teamwork. 7
The multidisciplinary teamwork approach is vital in streamlining human immunodeficiency virus (HIV) care, 7 including prevention of mother-to-child transmission (PMTCT) services, due to the complexity of intervention. 8 PMTCT intervention is composed of essential sequential steps, known as the cascade of treatment, that are needed to prevent mother-to-child HIV transmission. The PMTCT cascade involves the uptake of services, including antenatal care, HIV counselling and testing, receiving antiretroviral therapy for HIV-positive pregnant women, safe birth, infant follow-up, infant feeding recommendations and postnatal follow-ups.10, 11 Due to the complexity of the PMTCT cascade, 10 it requires several skilled healthcare workers across the health system to work together to provide PMTCT services. Therefore, multidisciplinary teamwork is particularly important to provide high-quality PMTCT services to HIV-positive pregnant women and their infants.6, 12 Barriers to multidisciplinary teamwork which include poor communication, lack of common goals, lack of leadership, poor team cohesion, professional culture and hierarchical relationships.13, 14 Lack of teamwork and communication breakdown among healthcare workers were considered as a barrier in providing quality HIV care,15, 16 including PMTCT services provision. 15 Studies have shown that communication breakdown resulted in unnecessary delays in service provision, disputes among healthcare workers, work fatigue 13 and a reduction in healthcare workers’ motivation to provide quality HIV care. 17 Lack of effective communication and collaboration among interprofessional teams has resulted in poorly coordinated patient care. 18
Fiji is classified as a low HIV prevalence country. However, HIV infection rates are gradually increasing. 19 In Fiji, PMTCT services were provided at the three divisional hospitals and their associated reproductive health centres at the time of data collection of this study. Fiji’s National Prevention of Parent to Child Transmission of HIV Policy 2010–2014 and the National Strategic Plan 2012–2015 recommended that PMTCT care should include a holistic approach to HIV treatment and care, and the development of a multidisciplinary core team. 19 An HIV core team should consist of an obstetrician, a midwife/nurse, a counsellor and a pediatrician 20 to oversee the PMTCT service provision across the continuum of care. The formation of this multidisciplinary healthcare team was to ensure the provision of comprehensive antenatal care and postnatal management for HIV-positive mothers and their infants. 20
There is a growing number of studies on teamwork among HIV workers, most of which have focused on teamwork in high HIV prevalence settings.3, 21, 22 However, this paper focuses on multidisciplinary teamwork among PMTCT workers from the perspectives of healthcare workers regarding health system challenges in a low HIV prevalence country. We conducted the research to explore facilitators related to the provision of PMTCT services in Fiji. This paper presents the partial findings from an extensive research project. The aim of this paper was to understand the key contributory factors in establishing effective multidisciplinary teamwork among healthcare workers in providing PMTCT services in Fiji.
Methods
The methods section of this study was guided by the Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist 23 and Standards for Reporting Qualitative Research (SRQR). 24 The COREQ checklist includes 32 required items designed to improve transparency and ensure comprehensive reporting of interviews in qualitative research (Supplementary Table 1). The SRQR checklist can be found in Supplementary Table 2.
Study Setting
The study was conducted at the three main divisional hospitals and their three associated reproductive health clinics where PMTCT services are provided in Fiji. The study sites included urban and semi-urban hospitals to ensure the study findings covered the different geographic locations and provided divergent viewpoints. 25 The pseudonyms for the study sites (Hospitals A, B and C) were used to maintain the anonymity of the study participants.
Study Design
This study took a qualitative approach to explore healthcare workers’ perspectives on health system challenges and facilitators for the provision of PMTCT services in tertiary hospitals in Fiji. Healthcare workers were recruited purposively. Healthcare workers across the broad spectrum of PMTCT service provision (from doctors to HIV counsellors) were carefully selected from different sites where PMTCT services were provided in Fiji.
In-depth interviews were conducted to collect data using a semi-structured, open-ended interview guide, enabling participants to respond freely and to elaborate where necessary. Healthcare workers were approached through the Head of Obstetrics and Gynaecology department and the Midwife in Charge of the Maternity unit, both of whom arranged for written information about the study to be sent to potential participants.
Data Collection
The lead investigator (A.R.) conducted interviews between April and May 2013 and February and March 2014 in three hospitals. A total of 58 healthcare workers who were involved in the provision of PMTCT services were interviewed. Theoretical saturation was reached. The intention of these interviews was to understand healthcare worker perspectives on the barriers and enabling factors in providing PMTCT services. The interview schedules of previously published qualitative studies of HIV-related health services were reviewed to inform the development of the interview guide.26–28 All interviews were conducted in English and audio-recorded, with permission to do this sought at the beginning of each interview. The duration of each interview varied between 30 min and an hour.
Data Analysis
The data were analysed using a thematic analysis approach, which encompasses the identification, analysis, and reporting of themes within the data.
The interviews were transcribed verbatim (by A.R.). During transcription, the study participants were de-identified and numerical identifiers were used to prevent identification of participants. All transcripts were double-checked against the audio recordings to ensure no errors occurred during transcription.
All interview transcripts were coded using NVivo 10 data management software (A.R.). An inductive coding technique was employed, where themes were derived from the interview data that were relevant to the study’s objective. The selection of codes was discussed between the authors (A.R. and N.A.A.) prior to their integration into themes. Codes describing similar types of data were grouped to identify a theme. The emerging themes were validated after discussion among authors. 29
A draft code list was prepared by carefully checking the first five interview transcripts to derive codes by hand (by A.R.). The draft code list was independently checked by the study’s co-author. Subsequently, the final code list was developed (A.R. and .A.A.).
Ethical Approval
Ethical approval was obtained from the relevant ethics committees. To ensure transparency in communication, each participant was given a detailed participant information sheet. Written consent was also obtained from all participants prior to their participation in the study.
Findings
We identified several themes in the data from the larger study; however, this paper focuses on multidisciplinary teamwork among healthcare workers while providing PMTCT-related services to pregnant women in the hospitals included in the study.
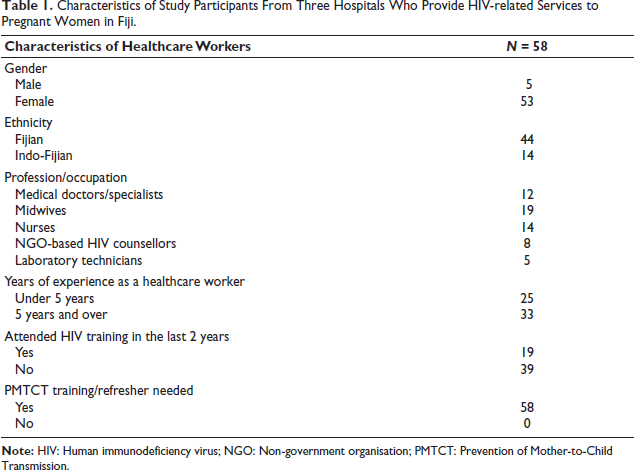
A total of 58 healthcare providers, including government-employed doctors (n = 12), midwives (n = 19), nurses (n = 14), laboratory technicians (n = 8) and non-government organisation (NGO)-based HIV/Health Screening counsellors (n = 5), were interviewed. Six healthcare workers refused to participate due to their busy work schedules. Most of the healthcare workers who participated in the study identified as women; five were men (Table 1). The majority had over 5 years of experience (with an average of 7 years’ experience) working in antenatal clinics and PMTCT services. A few healthcare workers, specifically 19 out of 58, had received training on PMTCT in the previous 2 years. The thematic analysis identified the three main factors associated with facilitating teamwork among these workers. These three sub-themes include integration of PMTCT services, effective communication and supportive colleagues.
Characteristics of Study Participants From Three Hospitals Who Provide HIV-related Services to Pregnant Women in Fiji.
Integration
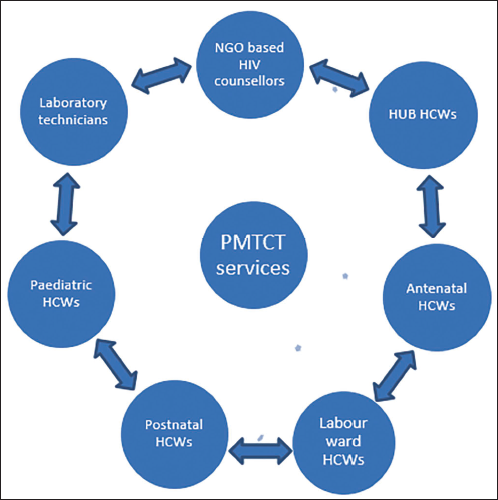
Integration of PMTCT services within the routine maternal and child health services in the three leading hospitals was evident from the interviews. Most of the healthcare workers, including doctors, nurses and midwives in this study, highlighted that several different hospital departments were involved in the provision of PMTCT services. These include obstetric and gynaecological units (including antenatal clinic, labour and postnatal wards), paediatric units and the HIV testing laboratory (Figure 1). The NGO-based HIV counsellors were responsible for providing pre- and post-HIV test counselling to pregnant women attending all three hospitals included in the study. The data showed that doctors were in charge of PMTCT service provision across the hospitals. In addition, the associated reproductive health centres were involved in follow-up and continuity of care for the HIV-positive women after they had been discharged from the hospital. The interview data showed that PMTCT services were linked or integrated across most study sites (partially at Hospital A).
Most of the healthcare workers, including doctors, nurses, midwives and HIV counsellors interviewed in this study, stated that because of integrated PMTCT services, healthcare workers at different levels of service provision were working together as a team. While the word ‘integration’ was not mentioned by these workers, most of them stated that different departments were connected and working with each other in the PMTCT service provision.
One midwife expressed the importance of teamwork across the continuum of PMTCT service provision. She acknowledged that once a pregnant woman was diagnosed as HIV-positive, a chain of services was offered to her. The treatment and care of HIV-positive pregnant women and their infants were provided by utilising a teamwork approach.
When we initially started [the PMTCT services], we were more confined because services were not linked, but now it is a team approach. Once someone is identified [as HIV-positive], we straight away get in the paediatrician and they talk about how the baby’s going to be cared for. And the HUB [reproductive health] centre, they come in when the patients are still in the hospital, because they need to follow these cases up. So, it’s more of a team approach now. (Interview_9, Midwife, Hospital A)
Senior doctors and midwives reported that each hospital had a specialised PMTCT team, known as the ‘HIV core team’. At the time of data collection, the core team met monthly to oversee the patient’s treatment and care plan to ensure a smooth HIV service provision. Similarly, a senior midwife and a doctor shared their experience that once a pregnant woman is diagnosed as HIV-positive, the HIV specialised units begin working together to provide the best treatment and care for both the HIV-positive mother and her infant. The quotes below reflect participants’ views on how healthcare workers from different departments are involved in PMTCT service provision.
Once a case [HIV-positive pregnant woman] has been identified, there’s a team approach in looking after them, so they can get the right care. We inform the obstetrician who recommends [the treatment and care plan] for the HIV-positive mother. Then we get in the paediatrician; they’ll talk about the feeding options [for the infant] and then the HUB [reproductive health] centre. (Interview_27, Midwife, Hospital B)
When we have a [HIV-positive] pregnant mom, then the HIV core team meet and discuss it [the care plan]. O and G [Obstetrics and gynaecology doctor] will contribute [to the care plan], like what medication they will be on, how the follow up is going to be and once they deliver. The paediatrician will look after the case and then it will come to the HUB—[reproductive health] centre. (Interview_52, Doctor, Hospital C)
Similarly, a midwife mentioned that the healthcare workers were collaborating with other specialised units as PMTCT services were integrated within the health system.
We have a [integrated] system in place, once we have a [HIV] positive mum, we started networking [with other units across hospital], We network with the paediatrician and others, that we have someone, who will be delivering very soon. Then they [paediatrician] need to come and discuss the feeding options and commence looking after the baby. So, the right care is given to them. (Interview_26, Midwife, Hospital B)
Communication
Most of the doctors, nurses, midwives and NGO-based HIV counsellors across the study sites considered continuous communication among themselves and with other specialised units essential for developing good relationships and facilitating teamwork.
We have good teamwork [because] we communicate amongst each other to provide the right care to these cases [HIV-positive pregnant women]. (Interview_6, Nurse, Hospital A)
Our interview data also indicated healthcare workers considered ongoing communication between hospital staff and the NGO-based HIV counsellors from Hospitals B and C essential for developing good working relationships between them. Many healthcare workers from Hospitals B and C discussed effective communication as an outcome of increased access to HIV test counselling, particularly post-test counselling, which led to improved communication and higher referral counselling rates.
When we refer to HIV-positive pregnant mothers, as it elaborates on the process of how the care cascade begins for HIV-positive pregnant women. We talk to them in a way, you know, they are happy and then they start sending the mothers to us [HIV test counselling]. Otherwise, they [hospital workers’ just sit there and do their work and not knowing what we are here for. (Interview_36, HIV counsellor, Hospital B)
On the other hand, the interviews from Hospital A indicated otherwise. NGO-based healthcare workers from Hospital A revealed low rates of post-test HIV counselling among pregnant women. The NGO-based HIV counsellors expressed that this was due to a lack of communication and cooperation (teamwork) between both groups.
Post-test counselling [referral] is not really good here—because they [Hospital healthcare workers] don’t refer mothers back to us and we miss out on their post-test counselling,—I think mostly, the barriers between us, we have to talk more, communicate with each other, the Ministry and ourselves. (Interview_ 14, NGO-based HIV counsellor, Hospital A)
Another NGO-based HIV counsellor from Hospital B shared that in her experience, issues can also be resolved through effective communication.
When things don’t work out, we talk [discuss] about it. We have our meetings, or I go straight to the assistant or to the nurse if anything [is problematic]. I’ve been here [for a long time] and they know me so, when I talk to them, they are open. (Interview_36, HIV counsellor, Hospital B)
Furthermore, most of the senior doctors, midwives and NGO-based HIV counsellors in this study reported that regular meetings between healthcare workers from different departments were paramount in improving communication and fostering teamwork.
In this regard, a doctor acknowledged the importance of monthly meetings of the specialised PMTCT team in delivering effective PMTCT services for HIV-positive pregnant women and their infants. Similarly, an NGO-based HIV counsellor and a doctor indicated that teamwork among PMTCT workers was improved by effective communication during regular meetings.
I think one of the strengths in dealing with PMTCT as well as HIV is our HIV core team. We meet every month and discuss over cases. So that’s one of the major strengths [in providing services]. (Interview_52, Doctor, HUB C)
We have monthly meetings and if there are any changes or anything [new comes up], so we ask them [nurses and midwives]. We open it to the floor. If there are new ideas about anything, we bring that up in the meetings and discuss it. (Interview_1, Doctor, Hospital A)
Supportive colleagues
Supportive colleagues were repeatedly mentioned as an enabling factor in the provision of PMTCT services to HIV-positive pregnant women and their infants. Most healthcare workers, including doctors, nurses, midwives and HIV counsellors in this study, stated that their colleagues were supportive in fostering a good working relationship. One of the midwives shared her experience, stating that her colleagues were cooperative while providing care to HIV-positive pregnant women.
My colleagues are very supportive; we all work together and help each other in looking after these cases [HIV-positive mothers]. (Interview_21, Midwife, Hospital B)
The staff are so cooperative and all of us get along very well, as a team, we are having a very good relationship with each other. (Interview_34, Doctor, Hospital B)
The data illustrate that the NGO-based HIV counsellors and government-employed healthcare workers, including doctors, nurses and midwives at Hospitals B and C, had good working relationships and worked together while providing PMTCT services. One NGO-based HIV counsellor expressed that government-employed healthcare workers were supportive and cooperate with them in providing HIV test counselling services to pregnant women.
In terms of working with the Ministry of Health, we get their full support, and they utilise our service [HIV counselling], which we have provided. (Interview_49, HIV counsellor, Hospital C)
However, the data from Hospital A highlight the existence of tension between hospital-employed healthcare workers and NGO-based HIV counsellors while providing HIV testing and counselling services to pregnant women. The predominant factors contributing to this tension include inadequate referral for HIV test counselling, a lack of cooperation and conflict arising from differences in counselling approaches, as discussed in a separate publication. 30
Discussion
This study explored the key contributory factors in establishing multidisciplinary teamwork among healthcare workers across the study sites. Our findings highlighted that the predominant factors enabling multidisciplinary teamwork were the integration of PMTCT services, effective communication and supportive colleagues.
Our findings revealed that healthcare workers considered multidisciplinary teamwork as an important facilitator in the quality PMTCT services provided to HIV-positive pregnant women and their infants across the study sites. In Fiji, most of the hospitals under study have fully adopted a teamwork approach. Our findings aligned with the Fiji Prevention of Parent-to-Child transmission of HIV Policy (2010) and the National Strategic Plan on HIV (2012–2015), both recommended a holistic team approach to PMTCT service provision. 19 These policies and plans have provided uniform guidance on the integration of PMTCT services into the primary healthcare system by utilising a holistic team approach.
However, our findings suggest that the holistic team approach component of the Fiji policy has only been partially implemented in one of the three hospitals we studied (Hospital A). This is due to the tensions between government-employed healthcare workers and NGO-based HIV counsellors, as discussed in a separate publication. 30
Most of the participants emphasised the crucial role of integration in promoting teamwork and enhancing the quality of PMTCT service provision at most study sites. One potential explanation for this observation is the requirement of a multi-stage continuum of HIV care, which required PMTCT workers from different departments to work together in teams. This collaborative effort ensures the provision of coordinated care to HIV-positive pregnant women and their infants.6, 7
In Fiji, PMTCT services were only integrated at the three main hospitals in Fiji. These services were not offered at the sub-divisional level or any other health facilities in the country at the time of data collection. This indicates that PMTCT services were not integrated throughout the Fijian health system. This may be due to the low HIV prevalence; large-scale integration of services was not required at the time of data collection. The integration of PMTCT services on a smaller scale might contribute to the cohesive linkage of PMTCT services across various departments in Fiji. Consequently, it became viable for PMTCT workers to collaborate in teams, ensuring the delivery of quality services.
Our data revealed that effective communication plays an important role in facilitating teamwork among PMTCT workers. Effective communication is a two-way exchange, which is conducive to developing collaborative working relationships among professionals. 31 Studies from other settings have shown that communication32, 33 is essential in facilitating information sharing, resolving conflicts, and building relationships. 32 The respondents in our study considered continuous communication via face-to-face meetings within units and with the other specialised units to be essential in the provision of quality PMTCT services. This has resulted in improved and maintained teamwork, leading to improved service provision.
Further, our research revealed that access to HIV post-test counselling was improved in Hospitals B and C as a result of ongoing communication between the government-employed hospital staff and the NGO-based HIV counsellors. This finding was also confirmed by reviewing the Empower Pacific Report (2015), 34 which indicated that the rates of HIV post-test counselling sessions for Hospitals B and C were significantly higher than in Hospital A. In 2014, approximately 75% of pregnant women received HIV post-test counselling sessions in Hospital B and 73% in Hospital C, whereas only 41% of women received post-test counselling in Hospital A. 34 The significantly high rates of HIV post-test counselling in Hospitals B and C could be due to an effective communication between the nurses and the NGO-based counsellors in these hospitals, as compared to Hospital A.
Supportive co-workers played an important role in developing relationships with other PMTCT workers and facilitating teamwork. Previous research found that support from colleagues and supervisors played an important role in enhancing healthcare workers’ motivation 17 to provide quality care, as well as improving patients’ experience of service provision. 17 Our findings were consistent with previous studies’, showing that supportive colleagues play a significant role in building good working relationships with each other.17, 32
Overall, Fiji has made significant progress in the provision of PMTCT services since the programme commenced in 2005. It is evident that HIV counselling and testing and antiretroviral coverage among pregnant women and infants have improved over the years. 19 Approximately, 98% of pregnant women consented to receive HIV testing in 2013 after they had undergone pre-test counselling, 20 compared to 66% in 2006 19 and 64% in 2003. 26 The linkage of counselling services with antenatal care has likely played a significant role in this increase in pre-test counselling of pregnant women.
One of the reasons behind this success is that PMTCT workers in Fiji have adopted multidisciplinary teamwork, working effectively with each other (partially at Hospital A). Multidisciplinary teamwork among PMTCT workers plays an important role in improvements in PMTCT service provision in Fiji. Although there was a hierarchical system in PMTCT service provision, effective communication and good relationships with each other could have weakened the traditional culture of hierarchy, and therefore, the efforts to provide effective PMTCT services in Fiji were not undermined.
Limitations and Strength
Our study has some limitations that should be considered when interpreting the results. First, we reported the experiences and perceptions of healthcare workers, which may be biased. This could arise when participants respond based on what they think the interviewer wants to hear, leading to bias. However, we attempted to minimise bias by collecting and triangulating data from different levels of healthcare workers, which enabled us to capture experiences from different healthcare workers’ perspectives.
A strength of the study included collecting and triangulating data from healthcare workers at different levels. Further research that encompasses in-depth interviews with healthcare workers from different departments would be beneficial in gaining a better understanding of whether a multidisciplinary team approach exists throughout the Fijian health system. This would also provide greater insight into its implications in the context of the Asia-Pacific Region.
Conclusion
Multidisciplinary teamwork was found to play an important role in PMTCT service provision in the three tertiary hospitals in Fiji (partially at Hospital A). Integration of PMTCT service, effective communication and supportive colleagues were the enabling factors in facilitating successful teamwork and improving the working relationships among healthcare workers. To validate our findings, Fiji’s PMTCT-related policies were reviewed to obtain some useful insights into how PMTCT services were delivered in Fiji. Our findings have confirmed that the teamwork component of Fiji’s National Policy was adopted at the local hospital level at most study sites (though partially at Hospital A). Multidisciplinary teamwork has influenced healthcare workers to collaborate in a coordinated way to ensure high-quality service provision. However, there is a need to improve teamwork among hospital healthcare workers and NGO-based HIV counsellors at Hospital A to ensure streamlined HIV counselling services for women attending antenatal clinics in Fiji.
Footnotes
Acknowledgements
This study is a part of the first author’s thesis to fulfil the requirements for the Doctor of Philosophy at the University of Sydney. We thank the Fiji Ministry of Health, Fiji Ministry of Education and the Suva hospital team for authorising and facilitating fieldwork and data collection. The authors’ special gratitude goes to the study participants for their time and valuable contributions. Finally, we acknowledge that data were collected during the first author’s PhD candidature at the University of New South Wales (UNSW). We thank all the former and the current supervisors for their valuable contributions, with special recognition to the late Professor Joanne Travaglia, who recently passed away. A preprint of this article was previously been published on MedRxiv (
Author Contributions
AR and HW designed the study. AR performed the analysis and interpreted the data, and AA reviewed it. AR prepared the manuscript. AA provided guidance and critical feedback throughout the write-up. AA and HW critically reviewed the draft versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article
Ethical Approval
Ethical approvals were obtained for this study.
Funding
A 1-year study scholarship was provided by the Human Resources for Health Knowledge Hub, University of New South Wales. No other grant was received in the development of this study. The authors received no other financial support for the research, authorship and/or publication of this article.
Informed Consent
All study participants were given a study information sheet and obtained written informed consent from all participants prior to their participation in this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.