
Abstract
HIV is a major health issue globally. Though highly effective antiretroviral therapy has improved the life expectancy, people living with HIV (PLHIV) suffer from many physical and psychological issues. The present study assessed perceived health status, quality of life (QOL) and treatment-seeking behaviour among PLHIV.
The study was carried out among 75 PLHIV attending ART clinic of a tertiary care centre of North India. Convenience sampling technique was used. Ethical approval for the study was obtained from the Institute Ethics Committee. Participants were asked to rate their current state of health as perceived by them on a five-point scale ranging from poor to excellent. QOL was assessed by using WHOQOL-BREF (Hindi version). Treatment-seeking behaviour was assessed by a structured questionnaire developed by researchers.
A total of 45.3% (n = 34) rated it as fair, 22.7% (n = 17) rated it as good 13.3% (n = 10) rated it as poor, 10.7% (n = 8) rated it as excellent and 8% (n = 6) rated it as very good. QOL score was highest in physical health domain with a mean ± S.D. of 12.3 ± 4.1 (median 13) and lowest in the social relationships domain with a mean of 8.6 ± 2.9 (median = 8) (p = .001). Most common reason of going for HIV testing was being symptomatic (n = 21) followed by spouse testing positive for HIV (n = 19).
HIV impacts QOL of the PLHIV and treatment-seeking behaviour varies among the patients. There is a need to develop a multilevel approach involving all the stakeholders including patient, family and society.
Background
HIV/AIDS continues to be a major public health issue globally. It has claimed 40.4 million (32.9–51.3 million) lives worldwide till now with ongoing transmission continuing in all countries across the globe. There were an estimated 39 million (33.1–45.7 million) people living with HIV (PLHIV) worldwide by the end of 2022. In 2022 alone, HIV/AIDS claimed 630,000 lives and 1.3 million new infections were reported in the same year. 1 India has an estimated total prevalence of HIV/AIDS as 0.21 (0.17–0.25) among adults (2021), 2 with 2.4 million people with HIV. A total of 63,000 new infections and 42,000 AIDS-related deaths were reported in 2021. It was estimated that approximately 65% of PLHIV are on antiretroviral treatment. 3 Access to healthcare with effective HIV preventive, diagnostic and treatment services have enabled PLHIV to have long and healthy lives and HIV has become a chronic illness now.1, 4 Though the survival is prolonged, still PLHIV continue to suffer from many physical problems including side effects of therapy like pain and fatigue, etc., mental health issues like depression and social issues like isolation.5, 6, 7 All these things determine their health status and impact the quality of life (QOL) of PLHIV. 8 As per the World Health Organization (WHO), ‘Quality of Life is an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’. 9 The QOL is not only dependent on the physical symptoms, rather it is a multifactorial concept. It has various determinants ranging from personal, physical, mental and sociocultural.10, 11 QOL is also related to and affected by treatment-seeking behaviour. 12 As India has a large population and consequently large number of PLHIV residing in different geographical areas with diverse cultural backgrounds, it becomes imperative to gain a deep insight about the QOL and treatment-seeking behaviour of PLHIV. It will help to identify which particular domain of QOL is worst hit and also identify what are the barriers faced by PLHIV while seeking treatment.
Material and Methods
The study was carried out among PLHIV attending the antiretroviral therapy clinic of the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh. It is one of the Centres of Excellence in HIV care. The study was approved from the Institute Ethics Committee of PGIMER, Chandigarh (INT/IEC/2020/SPL-985). PLHIV of age 18 years and above, on treatment for HIV for at least 1 month and able to understand Hindi language were included in the study. A total of 75 PLHIV were selected to participate in the study by using convenience sampling technique. Sample size calculation was done after taking into account the standard deviation obtained from a pilot study and precision of 80%. The highest standard deviation (3.2) was chosen out of all domains of QOL. The desired sample size came out to be 68 (including 10% attrition). Data were collected from the period of February–September 2022. After obtaining written informed consent, the participants were interviewed using a validated proforma to fill sociodemographic details, personal profile and clinical details. Socioeconomic status of the participants was calculated based on the modified Kuppuswamy socioeconomic scale (2022). 13 Participants are asked to give rating to their current state of health as perceived by them on a five-point scale ranging from poor to excellent. QOL was assessed by using WHOQOL-BREF (Hindi version). It is a standardized instrument given by WHO and its Hindi version is adapted to be used in Indian Health Care settings. 14 It contains a total of 26 items. Out of which 24 items are divided into various domains. In addition to that there are two items from the overall QOL and general health facet. Remaining 24 items are divided into various domains, including physical health, psychological, social relationships and environment. Scoring of WHOQOL-BREF (Hindi version) was done as per instructions and raw scores were transformed that to be equivalent of the WHOQOL 100. Treatment-seeking behaviour was assessed by a structured questionnaire. Statistical analysis was done using parametric or non-parametric test as per the normality and p value less than .05 was adopted as the level of significance.
Results
Sociodemographic Details
In total, 75 PLHIV were selected to participate in the study by using convenience sampling technique. In total, 26 (34.7%) of the study subjects were in the age group of 35 to 44 years followed by 16 (21.3%) in 25–34 years age group. Males were 46 (61.3%) and outnumbered the females who were 29 (38.7%). As per marital status 48 (64%) were married, 18 (24%) were unmarried, 7 (9.3%) were widow/widower and 2 (2.7%) were divorced. In total, 56 (74.7%) of the PLHIV were residing in nuclear families. In total, 54 (58%) belonged to socioeconomic Category IV (upper lower) as per the modified Kuppuswamy socioeconomic scale (2022), 14 (18.7%) belonged to Category V (lower), 11 (14.7%) belonged to Category III (lower middle) and only 6 (8%) belonged to Category II (upper middle). Almost equal numbers of participants belonged to rural (50.7%) and urban areas (49.3%). As per educational status, nearly one-third 34.7 % were educated till senior secondary and 13.3% were illiterate. Maximum, that is, 48 (64%) belonged to the Hindu religion. As per occupation, 3 (4%) were unemployed, 21 (28%) were homemakers, 14 (18.7%) were skilled workers, 14 (18.7%) were labourers, 10 (13.3%) were farmers, 6 (8%) were professional, 5 (6.7%) were students and 1 (1.3%) was business and retired professionals each. As per disease classification according to WHO, 58 (77.3%) participants belonged to Stage 1, 9 (12%) belonged to Stage 2, 7 (9.3%) belonged to Stage 3 and 1 (1.3%) belonged to Stage 4. Maximum duration of the disease was 20 years and minimum duration was 1 year with a median duration of 7 years.
Personal Profile
Out of 75 participants, 11 (14.7%) were smokers and history of alcohol intake was found in 10 (13.3%) individuals. In total, 24 (32%) did not have any known risk factor related to HIV. In 32 (42.7%) subjects the spouse had tested positive for HIV, 9(12%) gave history of IV drug use, 2 (2.7%) gave history of tattooing, 1 (1.3%) had history of blood transfusion in past, 1 (1.3%) had history of intravenous drug use and tattooing both, while 6 (8%) had other risk factors, like parents tested positive, men having sex with men, commercial sex worker, and multiple sexual partners.
Health Status and Quality of Life
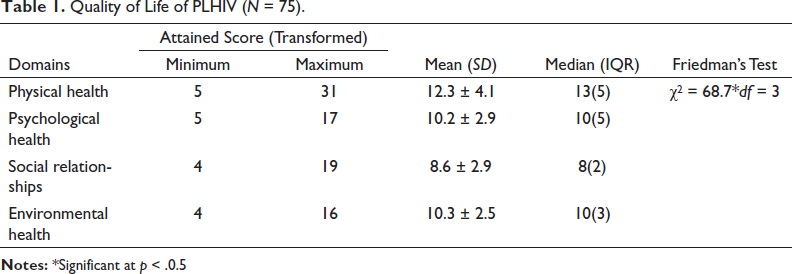
All the subjects were asked to rate their health status on a five-point rating scale and 10 (13.3%) rated it as poor, 34 (45.3%) rated it as fair, 17 (22.7%) rated it as good, 6 (8%) rated it as very good and 8 (10.7%) rated it as excellent. The participants had a relatively better QOL in the physical health domain (mean = 12.3 ± 4.1, median 13), followed by the environmental health domain (mean = 10.3 ± 2.5, median = 10), the psychological domain (mean = 10.2 ± 2.9, median =10) and lowest in the social relationships domain (mean = 8.6 ± 2.9, median = 8) (p < .001) (Table 1). Spearman’s correlation coefficient was calculated between perceived health status and QOL of study subjects. It was found that there was a positive correlation between perceived health status and QOL of PLHIV (r = 0.614, p < .001). However, no statistically significant association was established between QOL and sociodemographic variables (p > .05).
Quality of Life of PLHIV (N = 75).
Treatment Seeking Behaviour
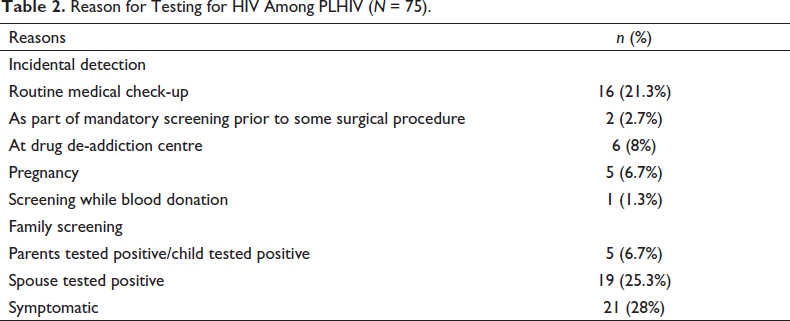
Table 2 summarizes the reason for getting tested for HIV among study participants. There were three types of reasons for undergoing HIV testing among the subjects. The most common reason cited was being symptomatic as 21 subjects (28%) got tested because of symptoms, followed by spouse testing positive for HIV in case of 19 subjects (25.3%). Data show that incidental detection was also common. As 16 (21.3%) subjects came to know their HIV positive status as part of a routine check-up. Other reasons for incidental detection included testing at drug de-addiction centre in case of 6 subjects (8%), during pregnancy in 5 subjects (6.7%), as part of mandatory screening prior to some surgical procedure in 2 subjects (2.7%) and screening while blood donation in 1 subject (1.3%). In total, 5 (6%) subjects underwent testing because any other family member (parent/child) already tested positive. There was no delay in the initiation of the treatment as reported by 100% of the subjects. All the patients (100%) relied on the healthcare workers for information regarding how to proceed for treatment. Family was the support system in seeking treatment among all 75 subjects (100%). Only 2 (2.7%) of the patients were taking home remedies also as alternative treatment along with the ART. A total of 68 (90.7%) reported that they are taking the prescribed treatment regularly as assessed by a recall of 1 month period, rest 9.3% were admitted that they are irregular due to forgetfulness. Maximum, that is, 94.7% (n = 71) reported no difficulty in seeking treatment for HIV. Only 4% (n = 3) patients reported difficulty in travelling for seeking treatment and 1.3% (n = 1) reported fear of revealing their disease status to anyone. In total, 84% (N = 63) of the participants preferred the same hospital as that of the ART centre for the treatment of other ailments also. More than half (65.3%) preferred it because they did not want to reveal their disease status anywhere else.
Reason for Testing for HIV Among PLHIV (N = 75).
Discussion
The present study threw light on the perceived health status, QOL and treatment-seeking behaviour of PLHIV attending the ART centre of a tertiary care hospital of North India. In this study, maximum of the PLHIV were less than 45 years of age and very few belonged to the age group of 65 years and above. A higher number of study subjects were males. These findings are consistent with findings from other studies, which also reported males in higher numbers as study subjects as compared to females.15, 16 In the present study, more than half (64%) were married and this finding is consistent with a study conducted in a North Indian state. 17 Most commonly identified risk factor was spouse testing positive for HIV. Early detection of HIV along with a prompt intervention coupled with ART for the index case in HIV sero-discordant couples can reduce the risk of infection to spouse. 18 Subjects in the present study had better QOL in the physical domain followed by environmental and psychological domains. Only 13% of the participants rated their self-perceived health status as poor and majority of the respondents (77.3%) belonged to WHO Category 1 for HIV/AIDS classification. There was a positive correlation between health status and QOL. These findings are consistent with the fact that early detection of HIV and timely initiation of ART and its adherence have improved the health status and physical QOL of PLHIV.19, 20 Worst QOL was reported in the social domain. Findings are consistent with other studies conducted in Indian settings as well as other parts of the globe in which the respondents had the lowest mean score in the social domain out of all four domains of QOL given by WHO.16, 21, 22 It has been found in various studies that due to their HIV positive status, PLHIV often suffer from both enacted stigma as well as internalized stigma there they tend to limit their social interactions. All these factors impact the social QOL of PLHIV to a great extent.23, 24 The published literature has revealed that social support has been identified as one of the important determinants of QOL among PLHIV. 25 Multilevel interventions focussing on PLHIV as well as targeting all the stakeholders involved like health professionals, family members as well as society are required to improve the QOL of PLHIV. Recent technological advancements including e-health mobile applications can also be utilized to provide preventive, promotive and curative services to target groups. 26 Social QOL can be improved by increasing motivational and emotional support of PLHIV by establishing sustainable and trustable support networks with effective clinical services and referral systems. 27
This study also presented a picture of treatment-seeking behaviour of PLHIV. It was revealed that a significant number of subjects (28%) underwent HIV testing because they experienced various symptoms. Another study from India also reported that 15% of the patients underwent HIV testing because they were sick. 28 A significant proportion was tested as part of family screening when either spouse (in case of 25.3%) or parents/child tested positive already (5.6%). Index testing/partner notification or contact tracing proves to be an effective strategy to find cases among the contacts of PLHIV, who would have otherwise missed HIV testing. This approach allows early identification, timely initiation of ART and reduction of chances of the further transmission of the virus. This also contributes to achievement of 95-95-95 targets by UNAIDS.29, 30 There was no delay in the initiation of the treatment. All the patients reported the healthcare professionals as their source of information regarding treatment. In the published literature, a good professional support in the form of counselling is reported to be an important predictor for treatment seeking and adherence. 31 A total of 92% admitted to taking treatment regularly. This adherence rate is high compared to studies in the literature, 32 it could be attributed to the small sample size of the study as well as self-report data involving recall bias. A maximum of PLHIV reported that they did not find any difficulty in accessing the treatment. However, few reported difficulties in travelling for treatment and few were concerned that no one should come to know about their HIV status. Majority of PLHIV (84%) preferred the same hospital as that of the ART centre for treatment of any other ailments also. The most common reason (65.3%) cited for that was that they do not want to reveal their disease status anywhere else. Similar concerns like confidentiality, fear of disclosure of HIV status to others and difficulty in travelling for treatment were reported in the literature as issues faced by PLHIV while seeking treatment. Effective care and support service along with social sensitization to decrease HIV-related stigma and discrimination will contribute to improve the treatment-seeking behaviour of PLHIV and consequently improving their QOL.33, 34 It is concluded that HIV effects the QOL of PLHIV in all domains; however, the social QOL is the worst hit. Many physical and social issues impact health status, QOL and treatment-seeking behaviour of PLHIV. There is a need to develop a multilevel approach involving all the stakeholders including patient, family and society.
Limitations
Limitations of the study include its small sample size and self-report method of data collection, which may not be free from the recall bias as well as participants’ tendency to give socially desirable responses.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved from the Institute Ethics Committee of PGIMER, Chandigarh (INT/IEC/2020/SPL-985).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from all the participants.