
Abstract
Introduction:
Pulmonary hypertension (PH) is a leading cause of mortality in systemic sclerosis (SSc), yet data from India remain limited. Although right heart catheterisation (RHC) is the gold standard, restricted access necessitates reliance on transthoracic echocardiography (TTE) for diagnosis and follow-up. This study describes the clinical characteristics and echocardiographic features of SSc-associated PH (SSc-PH) and compares isolated PH with PH associated with interstitial lung disease (PH-ILD).
Methodology:
In this retrospective study, patients fulfilling the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria for SSc and diagnosed with moderate- to high probability PH (as per European Society of Cardiology/European Respiratory Society [ESC/ERS] criteria) on TTE between January 2006 and January 2023 were included. Patients were categorised into isolated PH or PH-ILD groups. Clinical worsening was defined as the need for long-term oxygen therapy (LTOT), hospitalisation or worsening New York Heart Association (NYHA) functional class.
Results:
Forty-nine patients met the inclusion criteria, of whom 79.6% were female. Thirty-nine patients had PH-ILD and 10 had isolated PH. Anti-centromere (CENP) antibody positivity was significantly higher in isolated PH. Clinical manifestations were broadly comparable between groups. Echocardiographic markers of severe PH, including right ventricular (RV) dysfunction and right heart dilatation, were more frequent in isolated PH. Serial echocardiography demonstrated improvement in tricuspid regurgitation velocity (TRV), pulmonary acceleration time (PAT) and right heart dimensions in both groups, with greater improvement observed in the PH-ILD group. Rates of clinical worsening were similar, but baseline pericardial effusion was significantly associated with worsening.
Conclusion:
Overall, isolated PH and PH-ILD showed comparable clinical profiles and outcomes, highlighting the utility of echocardiography as a practical diagnostic and monitoring tool for SSc-PH in resource-limited settings.
Keywords
Introduction
Systemic sclerosis (SSc) is a multisystem autoimmune disease in which pulmonary hypertension (PH) is a significant cause of morbidity and the leading cause of mortality. 1 Despite its significance, data on SSc-associated PH (SSc-PH) remain limited from India and other low-resource regions, where prevalence, natural history and treatment outcomes are underreported.
The diagnostic gold standard for PH is right heart catheterisation (RHC). According to the 2022 European Society of Cardiology/European Respiratory Society (ESC/ERS) guidelines, PH is defined as a mean pulmonary arterial pressure (mPAP) > 20 mmHg at rest, with pulmonary vascular resistance (PVR) > 2 Wood units and pulmonary arterial wedge pressure (PAWP) ≤ 15 mmHg. 2
With the emergence of vasodilatory and antifibrotic therapies, timely diagnosis and optimised risk assessment are becoming increasingly important. In cost-constrained settings, however, access to RHC and advanced risk assessment tools is limited. Echocardiography, therefore, remains the mainstay for screening and follow-up, with parameters such as tricuspid regurgitant velocity, right ventricular (RV) size/function and right atrial (RA) enlargement guiding clinical management. Generating region-specific data is crucial for refining strategies for the early detection and management of SSc-PH, particularly where echocardiography-based approaches remain the standard of care.
This study aimed to analyse the clinical profile, echocardiographic findings and clinical outcomes of SSc patients with PH at a tertiary care centre in India.
Methodology
Study Population
In this retrospective study, patients fulfilling the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for SSc3,4 and identified as having intermediate to high probability of PH by transthoracic echocardiography (TTE) between January 2006 and January 2023 were included.2,5,6
Patients with intermediate to high probability of PH, diagnosed on transthoracic echo, were started on therapy for PH. RHC was not performed in any of the patients. PH was defined according to the ESC/ERS guidelines, based on tricuspid regurgitation velocity (TRV) and additional echocardiographic signs suggestive of PH. Specifically, TRV > 3.4 m/s or TRV 2.9–3.4 m/s in the presence of other PH signs (RA/RV enlargement, interventricular septal flattening or shortened pulmonary acceleration time [PAT]) was considered high probability; TRV 2.9–3.4 m/s without additional echocardiographic signs of PH or TRV ≤ 2.8 m/s with other supportive echocardiographic features suggestive of PH was considered intermediate probability of PH. 2
All patients underwent routine high-resolution computed tomography (HRCT) of the chest. Interstitial lung disease (ILD) was diagnosed when HRCT demonstrated typical interstitial changes, as confirmed by a radiologist. Pulmonary function testing was also performed in all participants.
Participants were stratified into two groups: (a) Isolated PH, if they fulfilled the echocardiographic criteria for intermediate/high probability of PH without evidence of ILD and (b) PH with ILD (PH-ILD), if they met criteria for both conditions. Disease onset and duration were defined by the date of onset of the first non-Raynaud’s phenomenon disease manifestation.
Clinical worsening was defined as the occurrence of any of the following during follow-up: Requirement for long-term oxygen therapy (LTOT), hospitalisation for disease-related complications or progression in New York Heart Association (NYHA) functional class.
Patients with overlap connective tissue diseases (e.g., mixed connective tissue disease, lupus, rheumatoid arthritis) and Group 2 PH due to left heart disease, including significant valvular heart disease, were excluded from the study.
This study was submitted to the Research and Ethics Committee, Institutional Review Board (IRB No.: 2411151), Christian Medical College, Vellore, India and was approved on 20 November 2024. A waiver of written informed consent was granted by the IRB in view of the retrospective study design.
Data Collection
Data were collected from medical records and electronic hospital databases. Disease onset and duration were defined by the date of onset of the first non-Raynaud’s phenomenon disease manifestation.
Laboratory Testing
Anti-nuclear antibody (ANA) was detected using indirect immunofluorescence, using the EUROIMMUNE IIF assay, with positivity defined at titres ≥1:100. Anti-topoisomerase I (Scl-70) and anti-centromere (CENP) antibodies were measured using enzyme-linked immunosorbent assay.
Statistical Analysis
Statistical analysis was done using SPSS (IBM SPSS Statistics for Windows, version 21.0. Armonk, NY: IBM Corp). Baseline variables and clinical characteristics were summarised as frequencies (percentages) for categorical variables and mean (standard deviation [SD]) for continuous variables. Continuous variables which were not normally distributed were summarised as median (interquartile range [IQR]). The chi-square test was used to compare categorical variables between the subgroups and the Mann-Whitney test was used to compare continuous variables. p value of < .05 was considered significant.
Results
Demographics
A total of 750 patients with SSc as per ACR/EULAR criteria were screened and 49 patients fulfilled the inclusion criteria; of whom 39 participants (79.6%) were female. Diffuse cutaneous SSc was the most common subgroup (25, 51.1%), followed by limited cutaneous SSc (19, 38.7%) and sine scleroderma (6, 12.2%). 39 patients had ILD as per HRCT criteria along with probable PH as per echo and 10 patients met criteria for isolated PH. Table 1 summarises the baseline characteristics of both groups.
Demographics, Clinical Features and Outcome of Study Patients.
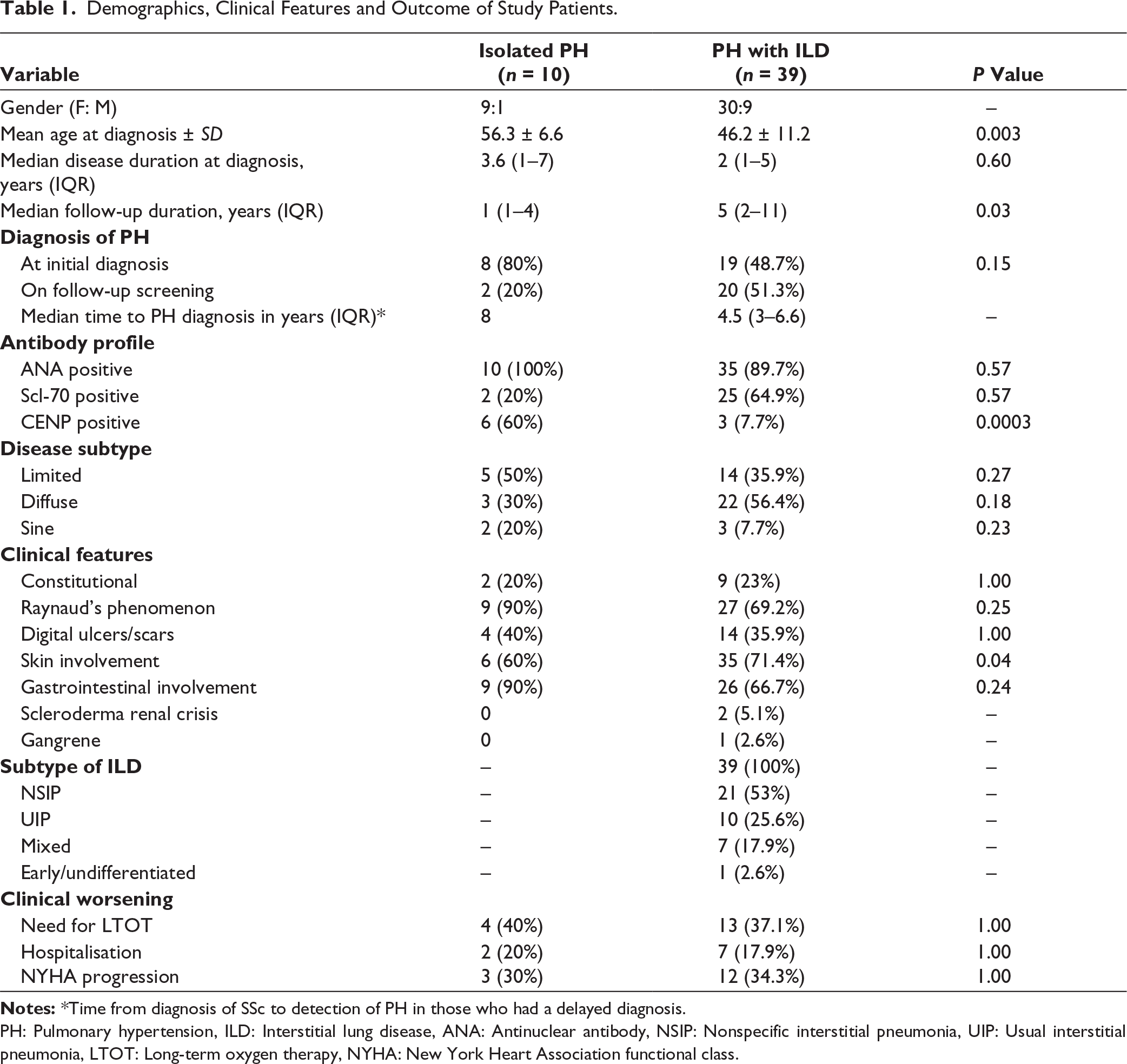
PH: Pulmonary hypertension, ILD: Interstitial lung disease, ANA: Antinuclear antibody, NSIP: Nonspecific interstitial pneumonia, UIP: Usual interstitial pneumonia, LTOT: Long-term oxygen therapy, NYHA: New York Heart Association functional class.
At the time of initial evaluation, 27 patients were diagnosed with PH. During the course of follow-up, 22 patients (two in the isolated PH group and 20 in the PH with ILD group) developed PH. The median time from diagnosis of SSc to development of PH was 4.5 years (IQR: 3–6.6) in the PH with ILD group. In the two cases with isolated PH, the same intervals were 8 and 9 years, respectively.
ANA was positive in all patients with isolated PH and 89.7% of patients with ILD with PH. Scl positivity was more in the PH with ILD group compared to the isolated group, but was not statistically significant (p value .57); however, anti-CENP positivity was significantly associated with isolated PH compared to the PH with ILD group (P < .001). Mean FVC in the isolated PH group was 71.1 and was higher than that of the PH with ILD group, which was 55 (P =.01). Diffusing capacity of the lung for carbon monoxide (DLCO) and the six-minute walk test were not routinely done in all patients.
Clinical Presentation and Treatment
Clinical presentations of Raynaud’s phenomenon (90% vs 69.2%), gastrointestinal involvement (90% vs. 66%), skin involvement (60% vs. 71%) and digital ulcers (20% vs. 23%) were observed in the isolated PH and PH with ILD groups, respectively. Telangiectasias were numerically higher in the isolated PH group (2/10%–20%) compared to the PH with ILD group (2/39–5.1%); however, this did not reach statistical significance (P = .19). Scleroderma renal crisis was encountered in two patients. Nonspecific interstitial pneumonia (NSIP) was the most frequently encountered HRCT pattern for ILD (53%), followed by UIP (25.6%), mixed NSIP and UIP (17.9%); early ILD was reported in one patient.
All patients with ILD were on immunosuppression. Mycophenolate mofetil (MMF) was used in 36 (92.3%) patients; azathioprine was used in three patients and two patients received rituximab injections due to progression of ILD on MMF. Three patients in the isolated PH group were on immunosuppression for diffuse skin involvement (MMF in two patients and methotrexate in one patient). All patients received vasodilator therapy; monotherapy was used in 30% of patients with isolated PH and in 25.6% of patients with PH with ILD (P value 1.00); dual therapy was used in 70% and 74.36% (P value 1). There was no difference in the frequency of vasodilator use between the two groups.
Echocardiography Features
As per the ESC/ERS criteria, one patient in the isolated PH group and nine patients in the PH-ILD group were classified as intermediate probability for PH; nine patients in the isolated PH group and 30 patients in the PH-ILD group were classified as high probability for PH.
Additional findings suggesting poor prognostic features include the presence of pericardial effusion, RA dilatation (RA area > 18 cm 2 ), RV dilatation (mid RV diameter > 35 mm) and RV systolic dysfunction (tricuspid annular plane systolic excursion [TAPSE]) < 1.7 cm.7,8 These findings were compared between the two groups. The prevalence of pericardial effusion (10% vs. 10.2%) was similar in both groups; a higher proportion of patients in the isolated PH group demonstrated RV dysfunction (30% vs. 10.2%, P = .12) and RA and Right Ventricular dilatation (50% vs. 25.6%, P = .13), although these differences did not reach statistical significance.
Echocardiographic parameters were compared with follow-up studies performed at 1–2 year intervals as per the physician’s discretion (Table 2). In the isolated PH group, median TRV decreased from 360 cm/s to 322 cm/s at follow-up, whereas in the PH-ILD group, it declined from 330 cm/s to 274 cm/s. The median change in TRV measurement on follow-up was numerically higher in the PH-ILD group (reduction by 53 cm/s) compared with the isolated PH group (reduction by 17.5 cm/s). (One patient in the PH-ILD had severe tricuspid regurgitation with a TRV value of 175 m/s; as this may not have been reliable, it was excluded from this analysis).
Echocardiographic Parameters at Baseline and at 1–2 Year Follow-up.
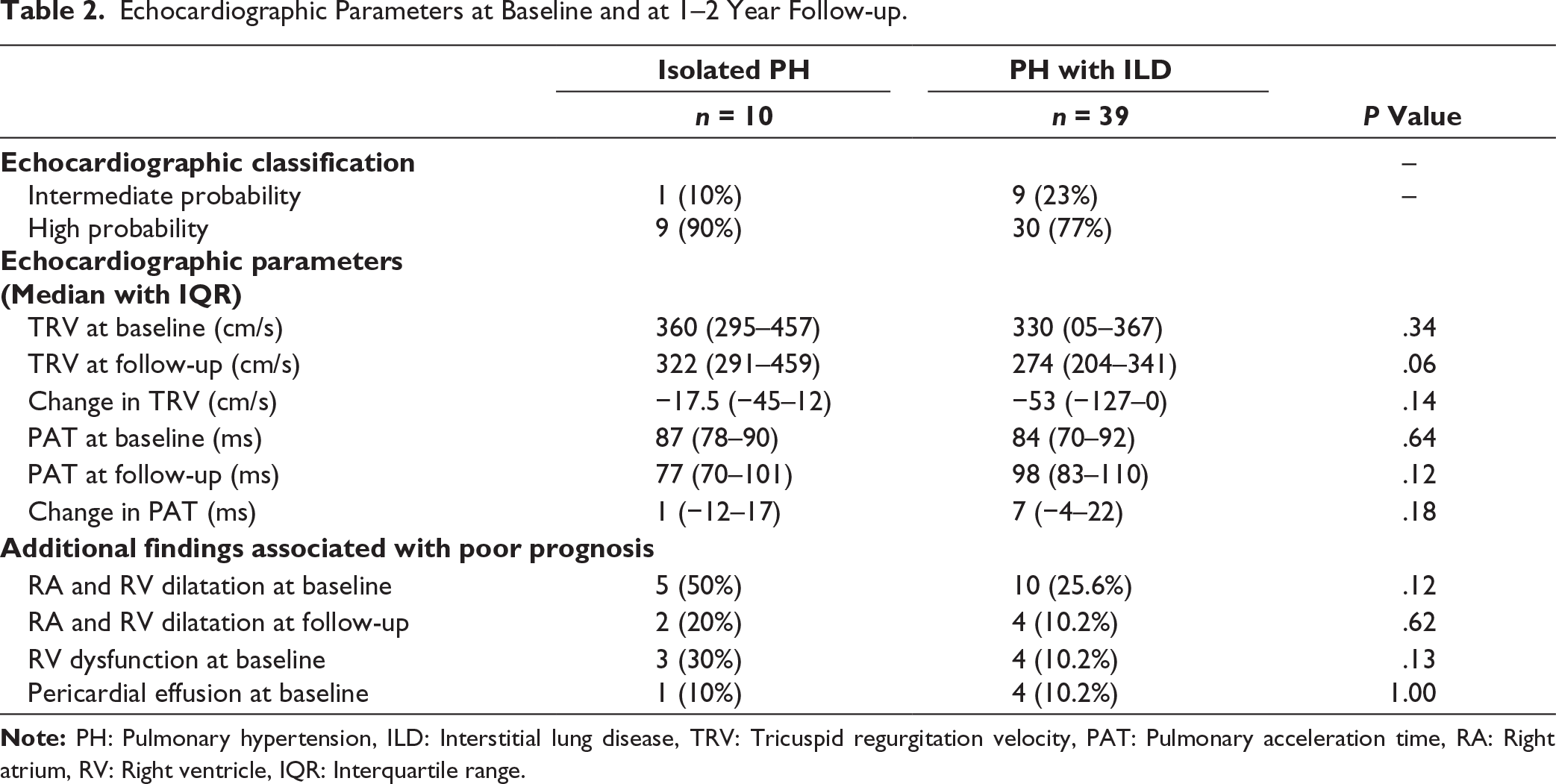
A similar trend was observed for PAT, with a median improvement of 7 ms in the PH-ILD group versus 1 ms in the isolated PH group. The proportion of patients with RA and RV dilatation showed a declining trend in both groups following therapy. Left ventricular systolic dysfunction (EF <55%) was observed in two patients, exclusively within the PH-ILD group.
Outcome
Clinical worsening during follow-up was compared between patients with isolated PH and those with PH associated with ILD, based on the need for LTOT (40% vs. 37.1%), NYHA functional class progression (20% vs. 17.9%) and hospitalisation for disease progression (30% vs. 34.3%). No statistically significant differences were observed between the two groups. Established prognostic factors in PH (Table 3) were analysed among patients who experienced clinical worsening versus those who remained stable. Presence of pericardial effusion at baseline showed a significant association with clinical worsening (P = .04).
Comparison of Poor Prognostic Factors Based on Clinical Worsening.

Discussion
PH is a serious complication of SSc, with a global prevalence of 6.4%. 9 In this single-centre study, TTE was used for diagnosis, longitudinal assessment and treatment modifications. At the index visit, most patients with isolated PH were diagnosed (80%), whereas a proportion of patients with PH-ILD were often identified later (51.3%), likely reflecting the contribution of group 3 PH to the aetiology. In both groups, a diagnostic delay of up to eight years was observed, underscoring the importance of regular screening. The clinical presentation and antibody profile were broadly comparable between patients with isolated PH and those with ILD-associated PH. Notably, telangiectasias were numerically more frequent (20% vs. 5.1%) and anti-CENP antibody positivity was significantly higher in the isolated PH group (P < .001) as described in previous studies as risk factors for PH.10,11
The gold standard for PH is RHC; however, due to its cost, need for expertise and its invasive nature, it is difficult to perform or repeat in daily clinical practice, especially in resource-limited settings. Moreover, the screening algorithms for RHC referral, such as DETECT and Australian Scleroderma Interest Group (ASIG), also warrant additional investigations, adding to the costs.12,13 Transthoracic echo is easy, inexpensive and easily accessible and previous studies have shown its measurements to have high correlation with RHC. In our study, we used parameters, TRV, Right Ventricular Outflow Tract (RVOT) acceleration time/PAT, in accordance with the ESC guidelines for diagnosis of PH and TAPSE for diagnosis of RV dysfunction. Previous meta-analyses have consistently demonstrated the value of echocardiography in the assessment of PH. Kadoglou et al. in a pooled analysis of 17 studies using RHC (mPAP >25 mmHg) as the reference, reported a median echocardiographic sensitivity of 87% (range 40%–98%) and specificity of 86% (range 33%–100%), with PAT, TRV and RV strain showing the strongest correlations. 14 Similarly, Dong et al. highlighted the diagnostic and prognostic relevance of echocardiographic markers, noting systolic pulmonary arterial pressure sensitivity of 0.85–0.88 and RV outflow tract acceleration time sensitivity and specificity of 0.84. Additional parameters, including pericardial effusion, RA area and TAPSE, were associated with adverse outcomes (hazard ratios 1.45–1.70), while RV longitudinal strain emerged as an independent predictor of prognosis (HR 2.96–3.67). 8
Ongoing risk stratification and treatment monitoring in PH are traditionally guided by validated prognostic models such as Registry to Evaluate Early and Long-term Pulmonary Arterial Hypertension Disease Management (REVEAL), REVEAL 2, Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA) and the three-strata ESC/ERS risk assessment tools.15–19 These calculators rely on a comprehensive, multimodal evaluation incorporating functional capacity, circulating biomarkers (NT-proBNP), DLCO and cardiopulmonary exercise testing. While valuable, the application of such strategies in routine practice remains challenging in resource- and cost-constrained settings. Echocardiography parameters such as TRV, TAPSE, RA and RV dimensions and the myocardial performance index, TAPSE/sPAP ratio have been reported as potential markers of therapeutic response to vasodilators and predicting risk in PH.20,21 In the present study, clinical assessment by the NYHA functional class combined with echocardiographic indices was used to optimise vasodilator therapy. On follow-up, improvements were noted in TRV, PAT and RA/RV dilation with numerically greater changes in the ILD-associated PH subgroup compared to isolated PH; whether this observation represents a differential response to PH-directed therapy and whether these parameters may be useful for risk stratification remains to be evaluated in prospective studies.
Prognosis differs by phenotype; an Australian cohort showed the worst outcomes in patients with extensive ILD-PH (HR 5.68, 95% CI 3.51–9.17), followed by PH-only (HR 4.30), extensive ILD-only (HR 3.72) and PH with limited ILD (HR 2.60). 22 In our study, clinical outcomes, including NYHA functional class progression, requirement for LTOT and hospitalisations, were comparable between groups. Assessment of known poor prognostic features in PH was compared in those with and without clinical worsening and found that the presence of pericardial effusion was independently associated with clinical worsening (P = .04), as has been previously identified as an important prognostic marker. 23 Larger prospective studies are required to validate these observations and to better define the prognostic utility of echocardiographic parameters in guiding therapy, particularly in settings where advanced multimodal risk assessment may not be feasible.
Limitations of the study include retrospective design, smaller numbers and variable follow-up periods across patients, which could affect the consistency of longitudinal data. Echocardiography, though a useful non-invasive tool for screening and estimating the probability of PH; it has several limitations. Doppler-derived pulmonary artery pressures depend on adequate tricuspid regurgitation signals and estimation of RA pressure, which may introduce variability. In addition, severe tricuspid regurgitation and suboptimal acoustic windows can underestimate the TRV value. Echocardiography also cannot reliably measure PVR or definitively differentiate the hemodynamic subtype of PH. Therefore, RHC remains the gold standard for the diagnosis and hemodynamic assessment of PH.
In spite of the limitations, this study represents the first Indian cohort analysis evaluating the clinical profile of patients with SSc-associated PH using echocardiography. The findings highlight the role of echocardiography not only as a diagnostic modality but also as a tool for longitudinal assessment. Establishing standardised echocardiographic parameters for follow-up could help with the objective evaluation of therapeutic response and enable treatment individualisation. Future research should focus on prospective, echocardiography-based parameters alongside clinical assessment to monitor and guide therapy. Such approaches will likely provide practical, cost-effective and easily implementable strategies suited to the Indian context.
Conclusion
Our study compared SSc patients with isolated PH and PH-ILD based on echo and found similar clinical profiles and outcomes, except for increased telangiectasias and higher anti-CENP antibody positivity in the isolated PH group. Serial follow-up of echocardiographic parameters such as TRV, PAT and RA/RV size showed improvement in the PH-ILD group. In resource-limited settings, the development of simple echocardiographic and clinically based diagnostic and prognostic tools remains a critical need.
Footnotes
Acknowledgements
We would like to acknowledge the echocardiography and laboratory staff for their technical assistance.
Declaration of Conflicting Interests
The co-authors, John Mathew, is an Associate Editor and Ashish J Mathew is an Editorial Board Member of the Indian Journal of Rheumatology and they were not involved in the decision-making process related to this manuscript. The authors declare no other potential conflict of interest with respect to the research, authorship and publication of this article.
Ethical Approval
This study has been approved by the Instituitional Review Board (IRB Min. No. 2411151 dated 20 November 2024).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
As it is a retrospective study, patient consent has been waived.