
Abstract
Background:
Systemic sclerosis (SSC) is a disorder characterised by fibrosis of skin and visceral organs. The disease in males is different from that in female patients, with early organ involvement and an aggressive course. Very few studies are exclusively on male SSC.
Objective:
To study the clinical, immunological and treatment profile of male SSC patients from Northern India. Materials and methods: 31 male scleroderma patients who met the 2013 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria were included in the study. Their demographic, clinical and autoantibody profiles and treatment protocols were recorded retrospectively from patient files.
Results:
Median age of study population was 38(15) years with a mean duration of disease 60(108) months. Diffuse cutaneous systemic sclerosis (dcSSc) was observed in 19(61%) patients, 10(32%) patients had limited cutaneous systemic sclerosis (lcSSc) and two (6%) patients had sine SSC. Vasculopathy is the predominant manifestation in 28(90%) of the patients. Other systems involved were musculoskeletal in 19(61%), pulmonary 19(61%) and gastrointestinal manifestations in 18(58%) patients. Two patients had scleroderma renal crisis (SRC). Three patients had overlap with other rheumatic diseases. 25(80%) patients were antinuclear antibody (ANA) positive with Scl70 being the common autoantibody. Glucocorticoids were used in 14(52%) of patients. cs DMARDS were used in 27(87.1%) of patients and more than 50% of patients required b DMARDS. One patient had an aggressive course and died in the early phase of illness.
Conclusion:
SSC in males is associated severe organ involvement, ANA negativity and requires aggressive early aggressive immunosuppression to prevent morbidity and mortality.
Introduction
Systemic sclerosis (SSc) is a complex autoimmune disease with multiple pathophysiological mechanisms, such as vasculopathy, endothelial dysfunction and fibrotic mechanisms with multiorgan involvement leading to rapid disease progression 1 SSc is a female predominant disease with sex ratios often cited between 3:1 and 14:1.Though the disease is less common in males, it is the male population that frequently bears the brunt of the disease with severe manifestations. 2 The disease occurs much later in males as compared to females by approximately five years.3,4 Interestingly, however, the mean time from the onset of symptoms till diagnosis is longer in females.5–7
The importance of addressing male SSc lies in the ‘male paradox’: Though the disease is less common in males, they are associated with higher morbidity and mortality. 8 Global registry data, including the EULAR Systemic Sclerosis Trials and Research (EUSTAR) cohort, consistently identify male sex as a strong independent predictor of poor survival.9,10 Men are disproportionately affected by the diffuse cutaneous systemic sclerosis (dcSSc) subtype and are at a heightened risk for severe organ manifestations such as interstitial lung disease (ILD), cardiac arrhythmias and scleroderma renal crisis (SRC) compared to their female counterparts.11–14 Female patients tend to have more calcinosis, pulmonary hypertension and heightened pain perception. 15
The basic pathophysiology behind the aggressive nature of male SSc is a distinct ‘hormonal genetic hit’. While oestrogens generally exert immunostimulatory effects, increasing immunoglobulin-producing plasma cells and enhancing TLR7-dependent interferon production, androgens typically provide immunosuppressive protection by inhibiting IL-1β and IL-6. In men with SSc, a paradoxically elevated oestradiol level stimulates a fibrotic phenotype by inducing M2 macrophage differentiation and inhibiting anti-fibrotic Th1 cells. Furthermore, sex hormones exert differential epigenetic effects: Oestrogens promote Deoxyribonucleic acid (DNA) demethylation, while androgens promote methylation. Coupled with the lack of mosaic immune protection from a second X-chromosome, these sex-linked epigenetic modifications and hormonal imbalances leave men susceptible to a ‘primed’, rapid inflammatory response, resulting in severe cutaneous and visceral involvement.15,16
The current evidence suggests behavioural differences, such as smoking and occupational exposure, may be leading factors linked to poor outcomes in men. Depending on the type of occupation, males are more exposed to silica dust and organic solvents, whereas females are more exposed to substances such as cadmium, lead and mercury.17,18 Other major contributing factors may be late diagnosis or misdiagnosis and an aggressive course of the disease in males. 9
Furthermore, the clinical presentation in men is often complicated by a ‘diagnostic gap’. While the time from the first Raynaud’s symptom to diagnosis may be shorter in men due to rapid symptom progression, they often present with established, irreversible visceral damage. 10 Studies have also suggested differences in treatment response between males and females. Females respond to MMF and oral cyclophosphamide better than males. On the other hand, male patients with SSc show relatively better responses to tocilizumab and nintedanib.19,20 Understanding the unique clinical and serological landscape of male SSc is therefore not merely an academic exercise but a clinical necessity to improve early detection and tailor aggressive therapeutic strategies.
Very few studies exist, especially in Asians, exclusively on male SSC. In this single-centre study, we look into clinical features, including the organ involvement, autoantibody profile and outcome of the male SSC patients from a rheumatology centre in North India.
Methodology
This is a retrospective, case-record-based observational study conducted at a rheumatology centre in the northern part of India between 2017 and 2025. Case files of all the male patients with SSC at this centre were examined. Those who met the 2013 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria were eligible to be included in the study. Data from the case records were transferred to an Excel sheet and analysed. The primary objective was to study the clinical profile, serological and treatment of male SSC. Case records were perused by the rheumatologists and the following data were collected: Symptoms and organ system involvement, serological profile, treatment provided to the patients and outcome of major manifestations. Data were entered into the Excel sheet and checked by another person for correctness. Continuous variables were expressed as median with interquartile range (IQR) or mean with standard deviation (SD). Categorical variables were mentioned as numbers (n) and percentages. Data were analysed using IBM SPSS version 25 software.
Details of Ethics Approval
The investigation was conducted in strict accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical clearance was obtained from the Institutional Ethics Committee, Army Hospital Research and Referral (IEC No. ECR /1990/Inst/DL/2024 registration no. 123/2025 dated 19 September 2025). To ensure patient confidentiality, all clinical and serological data were anonymised and de-identified before analysis. As the study utilised retrospective clinical records, a waiver of informed consent was granted for archived data, while written informed consent was maintained for patients who remained under active follow-up during the data collection phase.
Patient Selection and Inclusion Criteria
The study population was identified through a systematic screening of the institutional electronic medical records and physical registers. The inclusion was limited strictly to male patients aged > 18 years at the time of diagnosis. To ensure diagnostic homogeneity, all included subjects were required to meet the 2013 ACR/EULAR classification criteria for SSC. 21
Patients were excluded if they presented with:
Incomplete medical records regarding primary serological and visceral outcomes.
Data Extraction and Quality Control
A standardised data collection template was developed in Microsoft Excel. Primary data perusal was conducted by two senior rheumatologists to ensure clinical accuracy. To minimise extraction bias and clerical errors, a ‘two-step verification’ protocol was implemented, where a third independent researcher cross-checked the entered data against original case files for 100% of the cohort.
The variables extracted were categorised into:
Demographic profile: Age at presentation, disease duration (defined from the first non-Raynaud’s symptom) and smoking status. Cutaneous phenotyping: Patients were classified into dcSSc, limited cutaneous systemic sclerosis (lcSSc) or sine SSC based on the extent of skin involvement. Skin thickness was quantified using the Modified Rodnan Skin Score (mRSS) across 17 body areas (score 0–51).
22
Vascular manifestations: Presence of Raynaud’s phenomenon, digital ulcers, pitting scars and digital gangrene or loss.
Organ System Assessment and Definitions
The primary objective was to define the visceral disease burden of male SSc. We utilised the following rigorous definitions:
Pulmonary Involvement
ILD was confirmed via high-resolution computed tomography of the chest, characterised by the presence of ground-glass opacities, reticular patterns or honeycombing. Pulmonary function tests, specifically forced vital capacity (FVC) and diffusion capacity for carbon monoxide, were recorded where available.
Cardiac Involvement
Cardiac involvement was conservatively defined as a composite of:
Electrocardiogram (ECG) abnormalities: Including conduction blocks, arrhythmias or ST-T wave changes. Echocardiographic abnormalities: Including left ventricular diastolic or systolic dysfunction and valvular abnormalities. Cardiomyopathy: Specifically looking for dilated cardiomyopathy (DCM) attributed to SSc-related myocardial fibrosis.
Gastrointestinal Involvement
Given the retrospective nature of the study, gastrointestinal (GI) involvement was limited to symptomatic manifestations, including dysphagia, chronic gastroesophageal reflux and early satiety. Objective assessments such as manometry or gastric emptying studies were recorded only in a subset of symptomatic patients.
Scleroderma Renal Crisis
SRC was defined by the sudden onset of severe hypertension (≥140/90 mmHg) and/or a rapid decline in renal function (rise in serum creatinine ≥50% from baseline). 23 The presence of microangiopathic hemolytic anaemia on peripheral smear and hypertensive encephalopathy was also monitored as supporting clinical markers for SRC within the cohort records.
Musculoskeletal Manifestations
The musculoskeletal assessment focused on both inflammatory and mechanical complications. We recorded the presence of arthritis, deformities, acro-osteolysis, myositis (based on proximal muscle weakness and elevated muscle enzymes) and tendon friction rubs. Contractures and joint deformities were documented as indicators of chronic fibrotic progression. Other organ manifestations, including haematological, neurological and constitutional symptoms, were recorded.
Nailfold Capillaroscopy
Nailfold capillaroscopy (NFC) was performed using a high-magnification videocapillaroscope or ophthalmoscope. Morphological patterns were classified into early, active or late patterns. Specific variables analysed included the presence of enlarged/giant capillaries, micro-haemorrhages, capillary loss (drop-out) and neo-angiogenesis (ramified capillaries). 24
Serological Profiling
Antinuclear antibody (ANA) testing was performed using indirect immunofluorescence on HEp-2 cells, with a titer of ≥ 1:80 considered positive. Patterns were reported according to the International Consensus on ANA Patterns (
Statistical Analysis
Statistical processing was performed using IBM SPSS version 25.0. Due to the non-Gaussian distribution of data in this specialised male cohort, continuous variables are expressed as median with IQR (Q1-Q3). Categorical variables are presented as absolute n and percentages. To investigate the association between antibody subsets (e.g., CENP, Scl-70) and clinical phenotypes (lcSSc vs. dcSSc), we employed the Fisher-Freeman-Halton exact test, which is more robust for small sample sizes and tables larger than 2 × 2. Given the exploratory nature of this study, P values were not adjusted for multiple comparisons; however, a P value < .05 was considered the threshold for statistical significance.
Results
Thirty-one male patients with SSC, eligible according to the ACR EULAR 2013 classification criteria, participated in the study. The median age of the study cohort was 38(15) years, with a mean duration of disease of 60(108) months. Nineteen patients (61%) had dcSSc, 10(32%) patients had lcSSc and two (7%) patients had sine SSC. Mean mRSS was 13(16). While Raynaud’s was the predominant symptom, seen in 28(90%) patients, three patients did not have Raynaud’s. Among patients with Raynaud’s, digital ulcers were present in approximately half of the patients. The next common manifestation was mucocutaneous symptoms in 23 patients (74%), with sclerodactyly being the most frequent, followed by puffiness of fingers. While telangiectasias were observed in seven patients, no patient exhibited calcinosis in our study cohort. Constitutional symptoms were observed in 22(71%) patients, with fatigue being the most common symptom, followed by myalgia and weight loss.
Musculoskeletal manifestations were seen in 19 patients (60%). Among musculoskeletal manifestations, arthritis was seen in 13(42%) patients, acro-osteolysis in four patients and myositis in seven patients. Among other major organ manifestations pulmonary involvement and gastrointestinal manifestations were the commonest in approximately 60% of patients. Other organs were also involved with haematological involvement in eight patients, cardiac involvement in five patients, renal involvement in two patients and neurological involvement in a patient. Among pulmonary manifestations, ILD was the leading ailment, followed by pulmonary artery hypertension (PAH). Usual interstitial pneumonia (UIP) and non-UIP patterns were almost the same. Cardiac manifestations included DCM in one patient and echocardiographic abnormalities in three patients, while five patients (including those with DCM and echocardiographic abnormalities) had abnormal ECG. Anaemia was the most common haematological manifestation. SRC was seen in two patients. Five patients had overlap with other rheumatic diseases.
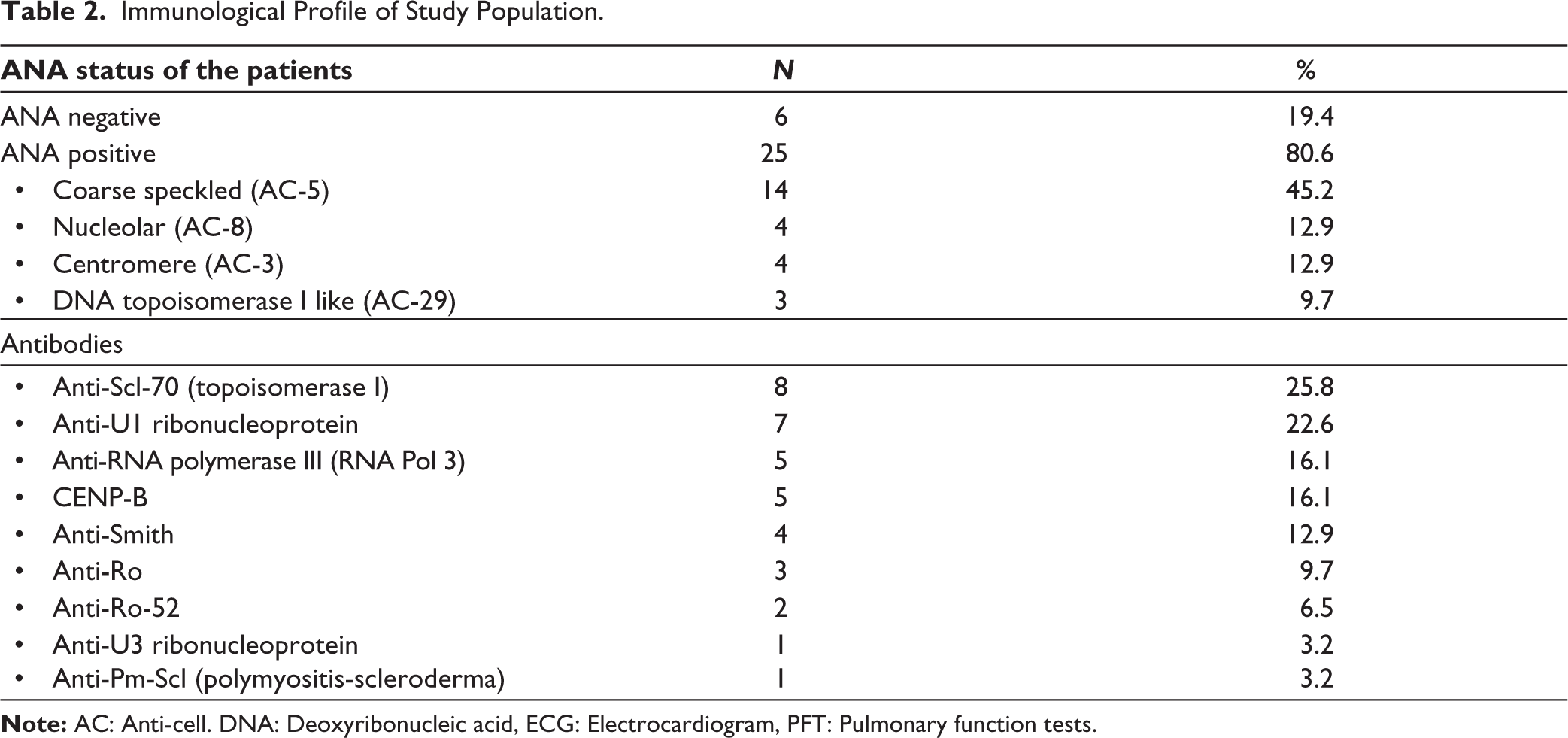
Nail fold capillaroscopy changes were seen in all patients with early NFC pattern in six patients and active and late pattern in 12 patients each. The NFC data of one patient was not available. Demographic profile and clinical features are given in Table 1. Immunological profile revealed ANA negativity in six patients (19.4%). The most common pattern was AC-5 (coarse speckled) in 14 patients (45%), followed by AC-3 (centromere) and AC-8 (nucleolar) in four patients each and the AC-29 pattern in three patients.
Demography and Clinical Characteristics of the Study Population.
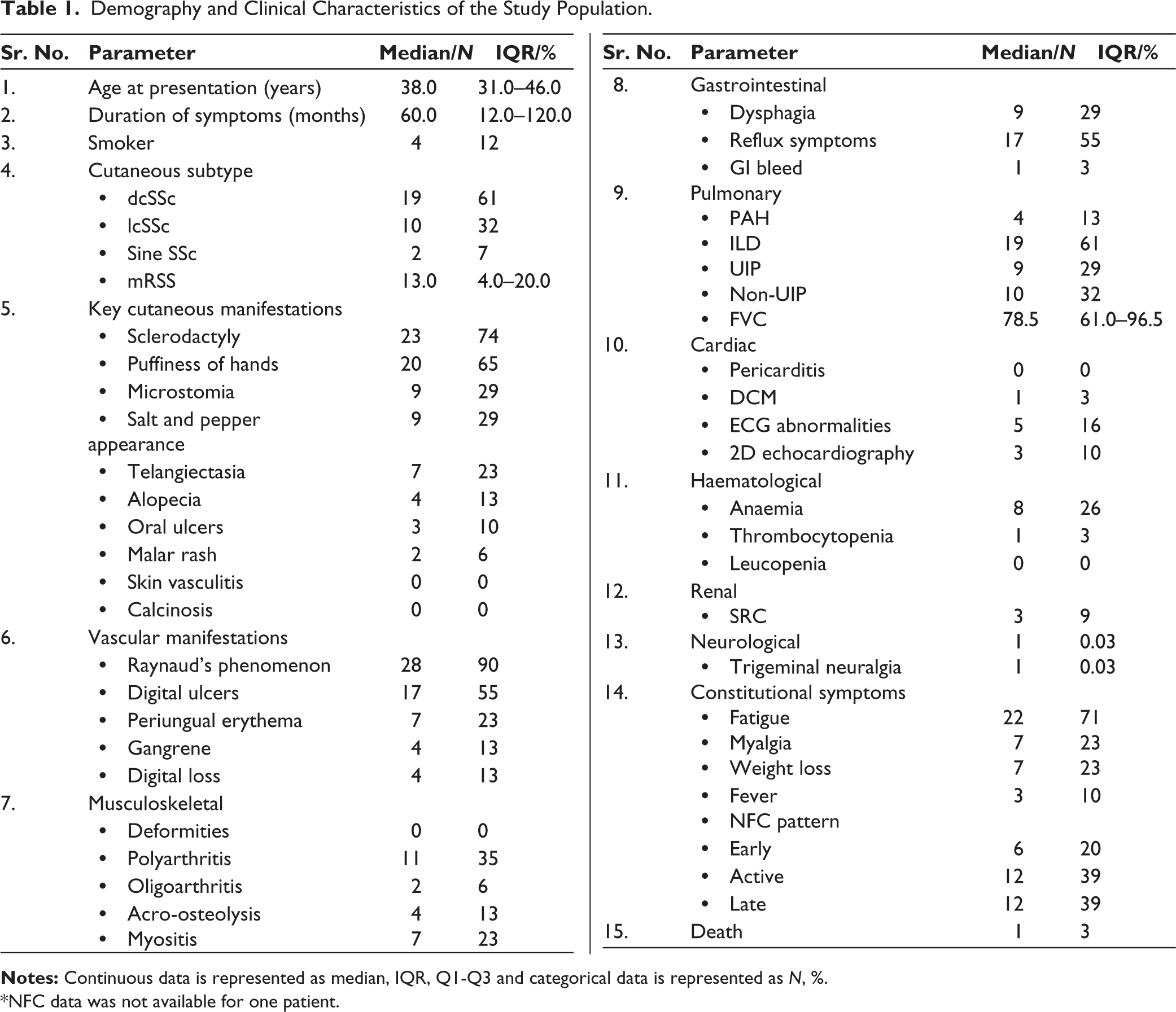
*NFC data was not available for one patient.
Scl-70 (anti-topoisomerase antibody) was positive in eight patients, U1-RNP in seven patients, CENP-B in five patients and RNA polymerase III in five patients (Table 2).
Immunological Profile of Study Population.
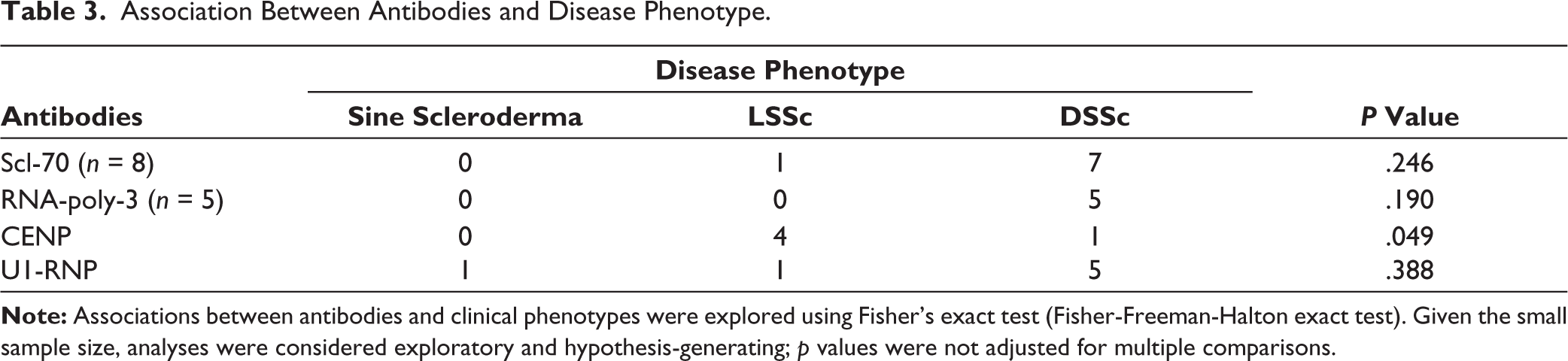
We explored the associations between antibodies and clinical phenotypes using Fisher’s exact test (Fisher-Freeman-Halton exact test) (Table 3). Given the small sample size, analyses were considered exploratory and hypothesis-generating; p values were not adjusted for multiple comparisons. Only the association between CENP and disease phenotypes was found to be significant, with a higher prevalence of LSSc phenotype in the presence of CENP. We also examined the relationship between antibodies and organ system involvement. CENP was significantly associated with a lower prevalence of ILD and fewer constitutional symptoms. All other associations were non-significant.
Association Between Antibodies and Disease Phenotype.
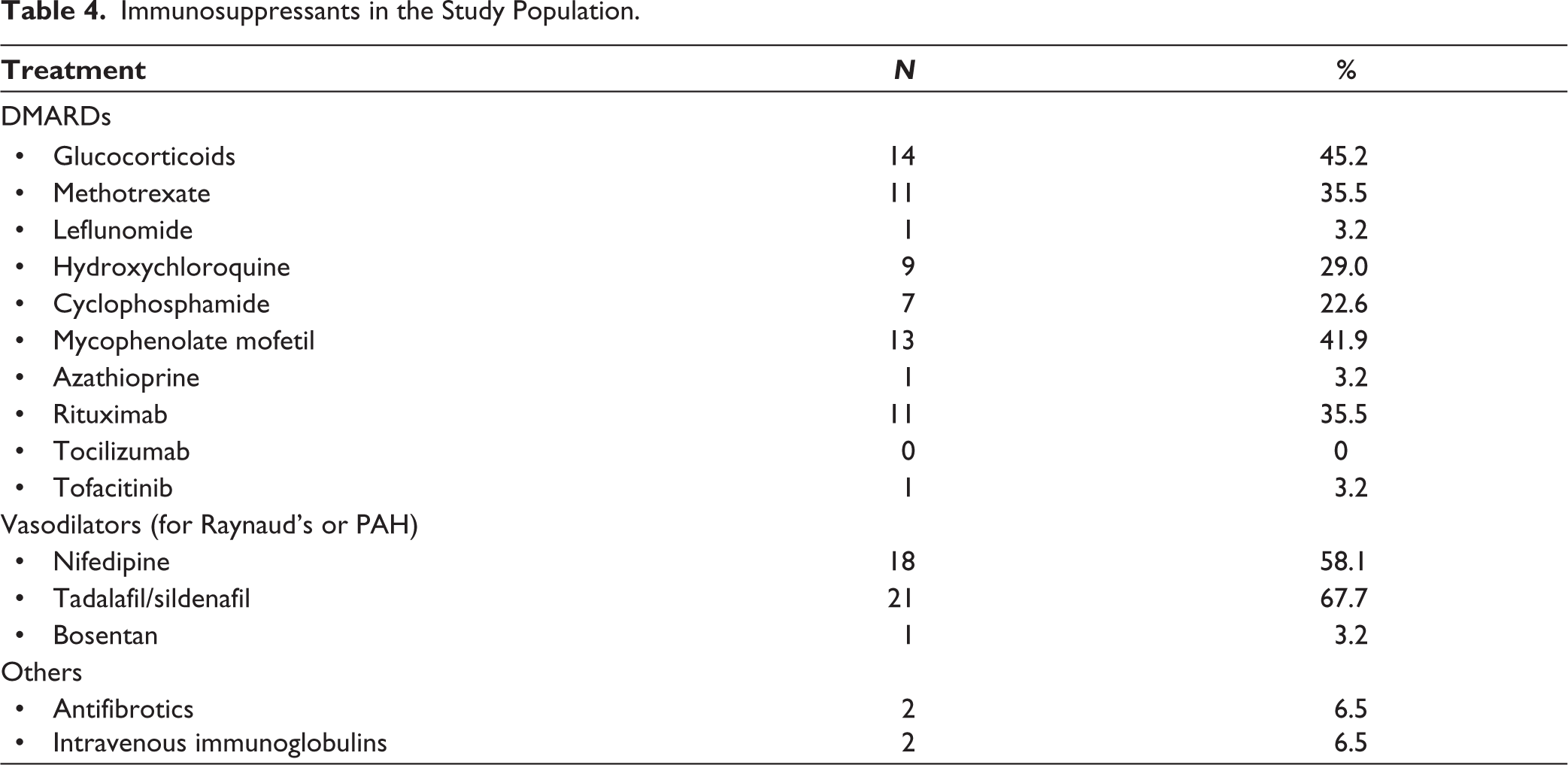
Most of the patients received aggressive immunosuppression. Low-dose steroids were used in 14 patients (45%) primarily for musculoskeletal manifestations (arthritis and myositis). Cyclophosphamide was used in 7(22%) patients and rituximab in 11(35%) patients. Almost all patients were on cs DMARDS and mycophenolate mofetil was commonly used in 13 patients (41%). Intravenous immunoglobulin was used in two patients. More than 50% of the patients received combination DMARDS (cs DMARDS/b DMARDS) at the time or sequentially. More than 90% of patients received vasodilators for Raynaud’s treatment and PPI/H2 blockers. Details of therapy received are given in (Table 4).
Immunosuppressants in the Study Population.
Discussion
In this small study, we tried to determine the clinical, immunological and outcome aspects of a cohort of Indian male patients with SSC. Vasculopathy was the predominant symptom in our cohort. Among non-Raynaud’s symptoms, most patients had mucocutaneous manifestations. Early and severe major organ manifestations were observed with pulmonary, gastrointestinal and muscle involvement. It’s worth noting that two patients had SRC, which is significant in our small cohort. Six patients were ANA negative, which is an important finding in our study. SCL 70, UIRNP and anti-RNA polymerase III were common SSC-specific antibodies. Cs DMARDS and b DMARDS alone or in combination were used in the majority of the patients.
One patient had a fatal outcome despite aggressive immunosuppression in the early course of illness. The patient was a 30-year-old male who presented with diffuse skin thickening, weight loss of 7 kg and postprandial fullness of three months’ duration. He had no Raynaud’s phenomenon. On evaluation, he had mRSS of 21 with salt pepper pigmentation, oesophageal dilation, active pattern on NFC and mild PAH. He had no cardiorespiratory involvement. ANA by IF, ANA blot and SSC auto-antibodies were negative. He was initiated on rituximab 1g two weeks apart. After two weeks of rituximab, he developed new-onset hypertension, painful visual blurring in both eyes and a seizure with a rise in serum creatinine from 0.7 to 2.1 mg/dl. On fundus fluorescent angiography, he had features of retinal vessel wall sheathing, macular oedema on ocular computed tomography and areas of haemorrhages on fundus examination. Despite panretinal photo-coagulation and ranibizumab, his visual symptoms progressed. Renal biopsy showed fibro-intimal proliferation and media thickening in arterioles, causing severe luminal compromise with prominent areas of GBM wrinkling suggestive of hypertensive changes. Four months after the onset of SRC, the disease-complicated with chronic diarrhoea, malnutrition and chronic kidney disease. Patient succumbed to his illness despite plasmapheresis, MMF and ramipril.
We could not find many studies exclusively on male SSC in the literature to compare our findings. In a recent comparative study comparing male and female SSC in the Brazilian population, which comprises 22 males, males had more vasculopathy features with fingertip ulcers and scars. 25 Other studies have shown similar findings. 26 Our study also shows predominant vasculopathy features, with more than 50% of the patients having fingertip ulcers. A study by Royle et al. reports an increased incidence of calcinosis in male SSC, while we could not find any reports of calcinosis in our study.7,27 In another comparative study done in 115 Thai patients (45 male patients), males had more cardiorespiratory dysfunction. 28 In our study, one patient had DCM, while approximately 25% of the patients had ECG and echocardiography abnormalities. PAH and ILD are among the leading causes of mortality in SSc. ILD is disproportionately more common in males than in females, as per existing evidence. Sixty percent of our study population had ILD. 6 Males are more prone to SRC and two of our patients had SRC.6,26 Current evidence does not show any sex disparity relating to gastrointestinal involvement in SSc. However, our cohort showed increased prevalence of GI symptoms as well. This reveals the multifactorial and heterogeneous nature of gastrointestinal involvement in SSc.
Six patients had ANA negativity, which is consistent with the study done by Salazar et al. 29 where 19.6% had ANA negativity in a huge SSC cohort of 3,249 patients. 6 Numerous studies have shown that SSC in males is associated with dcSSc, anti-topoisomerase or anti-RNA polymerase III antibodies and also early deaths.30,31 These clinical and serological findings were similar to those in our study. Our cohort also had one death and high disease activity is also evident from the early and aggressive immunosuppression in these patients.
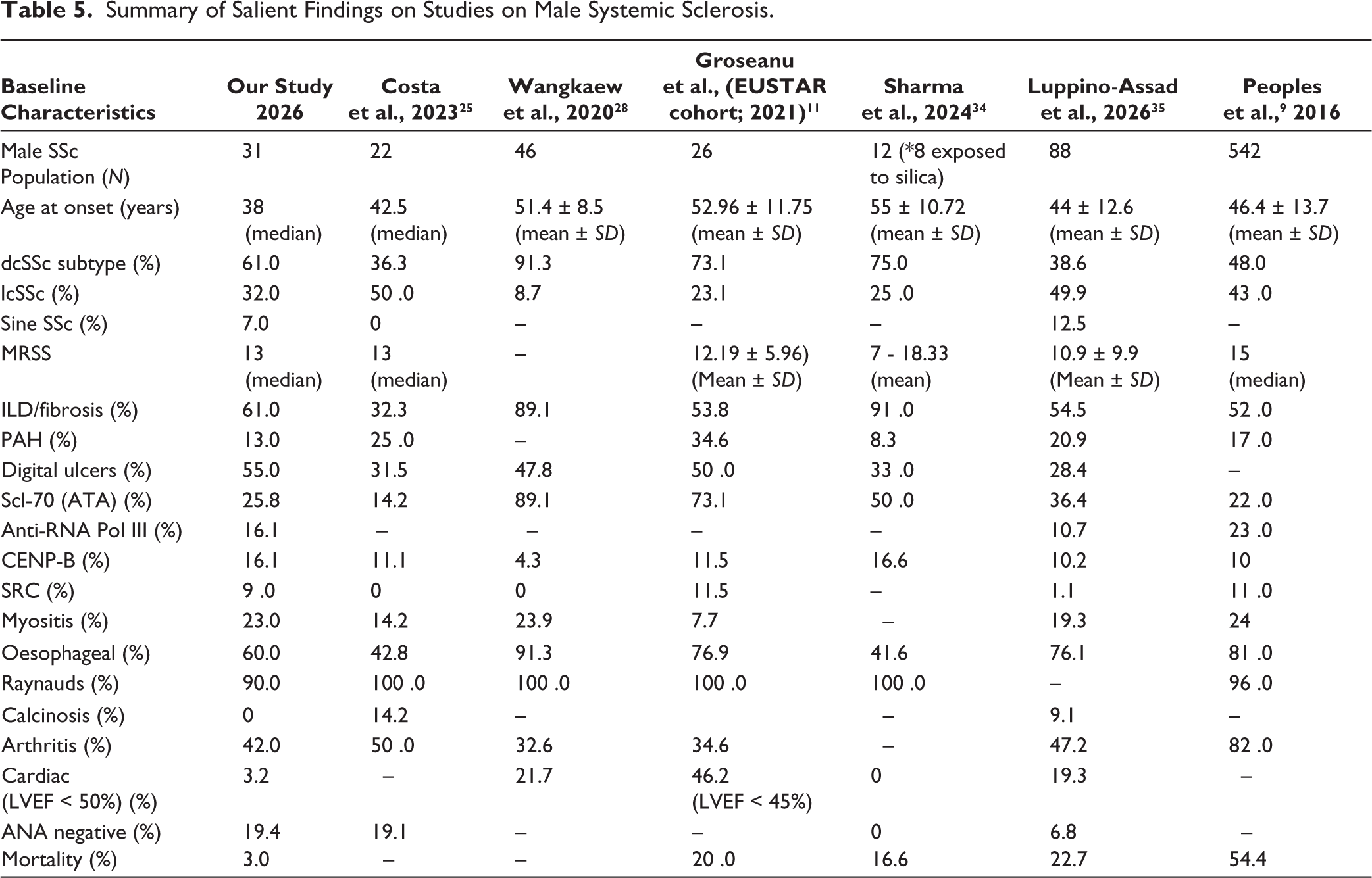
The reasons for the differences in SSC are very vague in the existing literature. Probable contributing factors are increased prevalence of smoking, occupational exposures such as silica and hormonal factors such as high oestradiol levels in elderly males. Other postulated factors are delay in seeking medical attention among men, leading to delayed diagnosis and missing the window of opportunity.32,33 There might be some difference in therapeutic intervention as well. The inflammatory immune signature of bronchoalveolar lavage in females, as compared to the profibrotic nature in males from the SSC lung study cohort, is another striking difference. 19 Salient features on various clinical outcomes in related studies are summarised in Table 5.
Summary of Salient Findings on Studies on Male Systemic Sclerosis.
The strength of our study is that we have done a study exclusively on male patients, which is a relatively less studied domain. Since it was a cross-sectional study, we could not examine the extended follow-up outcome of our cohort.
Conclusion
SSC in males is associated with major organ involvement, with high ANA negativity and requires aggressive early immunosuppression to prevent morbidity and mortality. Large long-term follow-up studies are essential to ascertain these findings and assess the implications of gender in SSc and tailored treatment strategies.
Footnotes
Acknowledgements
Nil.
Authors’ Contribution
The first and second authors (SJ and PS) are the guarantors of the article, had full access to the data, analysis and the decision to publish the study. We affirm that the data is correct and the analysis as decided in protocol has been transparently reported, with any non-prespecified analyses carried out being reported to be so.
Concept design and manuscript drafting: SJ & PS
Data collection and revision: SJ, PS, HJ, KK, RS, AVK, NG, AC, KS, AK, VV, AMN
Data Availability Statement
Requests for sharing the trial data can be addressed to the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Ethics Committee of Army Hospital Research and Referral, IEC Registration no. 123/2025.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Vivek Vasdev is an Associate Editor in the journal and was not involved in the decision-making process related to this manuscript.
Policy of Data Sharing
Data will be shared on receiving reasonable requests.