
Abstract
Dear Editor,
Distinguishing disease flare from infection in febrile patients with systemic lupus erythematosus (SLE) remains challenging because management differs substantially. Although biomarker-based models have been proposed, their routine applicability, particularly in resource-limited settings, is challenging. The relative dissociation between erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) in interferon-driven immune-mediated inflammation provides a biologically plausible basis for differentiating flare from infection in SLE. 1
Mehta et al. evaluated 168 febrile SLE patients across four Indian centres and developed a composite model incorporating age, total leukocyte count, CRP, anti-dsDNA, complement levels, neutrophil to lymphocyte ratio, and neutrophil activation indices, achieving an area under the curve (AUC) of 0.88 in the derivation cohort and 0.83 in validation cohorts. A lower ESR:CRP ratio was associated with infection. 2 In a Western multicentre cohort, Amarnani et al. showed that models integrating ESR:CRP ratio, leukocyte parameters, CRP, and additional biomarkers outperformed individual markers, although implementation may be difficult in many settings. 3 Prior studies have also highlighted the diagnostic relevance of discordance between ESR and CRP in febrile SLE. 4
We conducted a prospective cross-sectional study at a tertiary care centre in Eastern India between January 2021 and June 2022. Adults aged ≥18 years fulfilling the 2019 EULAR/ACR classification criteria for SLE and presenting with documented fever >38°C were eligible. Patients with pregnancy, malignancy, chronic infection such as tuberculosis, or those having concurrent flare and infection were excluded. Flares were classified as major or minor using the SELENA-SLEDAI Flare Index.
Sixty-five patients were enrolled. Forty (62%) had flare (major 12; minor 28), and 25 (38%) had infection. Infection was defined by a site-specific clinical presentation supported by microbiological confirmation or radiological evidence, together with documented clinical response to antimicrobial therapy. Infections were predominantly bacterial (17), followed by viral (6) and fungal (2). The lower respiratory tract was the most frequent site (8/25, 32%), commonly due to Streptococcus pneumoniae or influenza A. Urinary tract infections accounted for six cases (24%), largely attributable to Escherichia coli. Bacteraemia occurred in four patients (16%), mainly Staphylococcus aureus or gram-negative bacilli. Four patients (16%) had meningitis, fungal, or other infections. Three (12%) had skin or soft tissue infections, most commonly S. aureus.
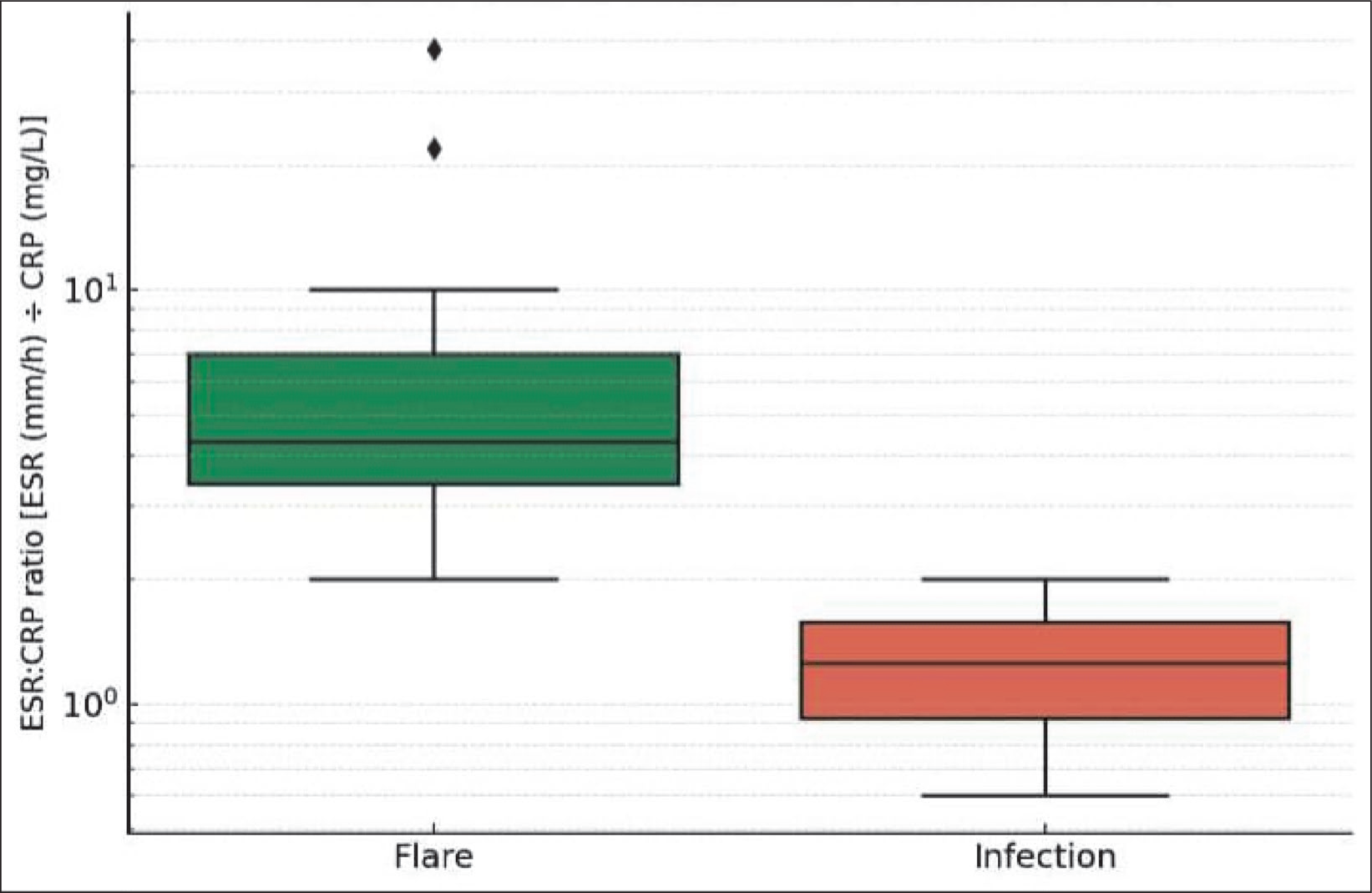
Continuous variables are presented as median (interquartile range). Compared with flare, infection was associated with higher CRP (56.4 vs. 8.8 mg/L), procalcitonin (6.8 vs. 0.05 ng/mL), total leukocyte count (13.9 vs. 6.6 × 10⁹/L), and neutrophil percentage (83% vs. 67%), and with a lower ESR:CRP ratio. Flares showed higher anti-dsDNA titres (182 vs. 20.6 IU/mL) and lower complement levels (C3: 82 vs. 112 mg/dL; C4: 7.4 vs. 15.8 mg/dL). The median ESR:CRP ratio was higher in flares than infections [3.7 (1.8–35.4) vs. 1.0 (0.7–1.5); P < .001] (Figure 1). On receiver operating characteristic analysis, the ESR:CRP ratio showed good discrimination for flare (AUC = 0.89; 95% CI 0.81–0.97). A cutoff >2 yielded a sensitivity of 82% (95% CI = 63%–93%) and specificity of 88% (95% CI = 69%–97%). The ESR:CRP ratio correlated positively with disease activity (Spearman’s ρ = 0.78; P < .001).
Box and Whisker Plot Showing Distribution of the ESR:CRP Ratio in Febrile SLE, Comparing Flare and Infection Groups. Values Are Plotted on a Logarithmic Y-axis as the Erythrocyte Sedimentation Rate (ESR, mm/h) Divided by C-reactive Protein (CRP, mg/L). Boxes Represent the Interquartile Range with the Horizontal Line Indicating the Median; Whiskers Extend to 1.5 × IQR, and Points Denote Outliers. Flare (n = 40) Shows Markedly Higher Ratios Compared with Infection (n = 25), Illustrating Clear Group Separation Despite Some Skewness.
A previous study by Emily Littlejohn et al. showed that an ESR:CRP ratio <2 was suggestive of infection and a ratio >15 was indicative of lupus flare. 5 Our study identifies an optimal data-driven ROC-derived cutoff of >2 in our cohort, demonstrating good discriminative performance and offering a simple, clinically actionable threshold. This may be particularly relevant in resource-constrained settings where access to advanced biomarkers is limited.
Our study had several limitations. First, the sample size was modest, and fewer variables were included than in previous multivariable models, which may limit generalisability. Hence, it requires validation in independent populations. Second, patients with concurrent flare and infection were excluded. Hence, applicability in overlapping complex real-world scenarios is limited and requires further evaluation. Third, subgroup analyses by infection type were limited by small numbers. Hence, larger multicentre studies are needed to confirm these findings. Nevertheless, the consistent performance of the ESR:CRP ratio in this independently recruited cohort supports its role as a potential single, low-cost, and universally available marker that can be readily derived from routine laboratory parameters without additional financial burden. In contrast to more specialised investigations, this ratio has the potential to serve as a pragmatic triage tool in everyday clinical practice, particularly in resource-limited settings where access to advanced biomarkers may be constrained. Facilitating early differentiation between flare and infection, it may aid timely clinical decision-making and guide appropriate therapeutic strategies even before more sophisticated diagnostic modalities become available.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
This study was reviewed and approved by the Institutional Ethics Committee (Reg. No.-ECR/287/Inst/WB/2013/RR-19), Medical College, Kolkata, 88, College Street, Kolkata 700073, West Bengal, India, with Ref. No. MC/KOL/IEC/NON-SPON/997/01/2021 dated January 22, 2021. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.