
Abstract

To the Editor,
Rheumatoid arthritis (RA) is associated with accelerated atherosclerosis, often mediated by metabolic syndrome (MetS). While the RA-MetS link is globally recognised, comparative data from South India—a region with a high baseline burden of Type 2 diabetes and the ‘Asian Indian Phenotype’—remains scarce. We conducted a prospective comparative study to estimate the burden of MetS in RA patients compared to age-matched healthy controls in a tertiary care centre in Kerala.
We enrolled 89 RA patients and 89 healthy controls. Inclusion criteria for the disease cohort comprised patients aged 30-60 years fulfilling the 2010 ACR/EULAR classification criteria for RA, 1 while controls were age- and sex-matched apparently healthy individuals attending a wellness clinic. Exclusion criteria for both groups included the presence of other autoimmune diseases, overlap syndromes, malignancy, chronic kidney disease, chronic liver disease, or chronic infections. MetS was defined using the NCEP ATP III (2005) criteria. 2 Written informed consent was obtained from all individual participants included in the study. The study was approved by the Institutional Human Ethics Committee, KIMSHEALTH Institutional Human Ethics Committee, document submission number Ref: KIMS/IHEC/FM-02/2021 and approved on 8/1/2021.
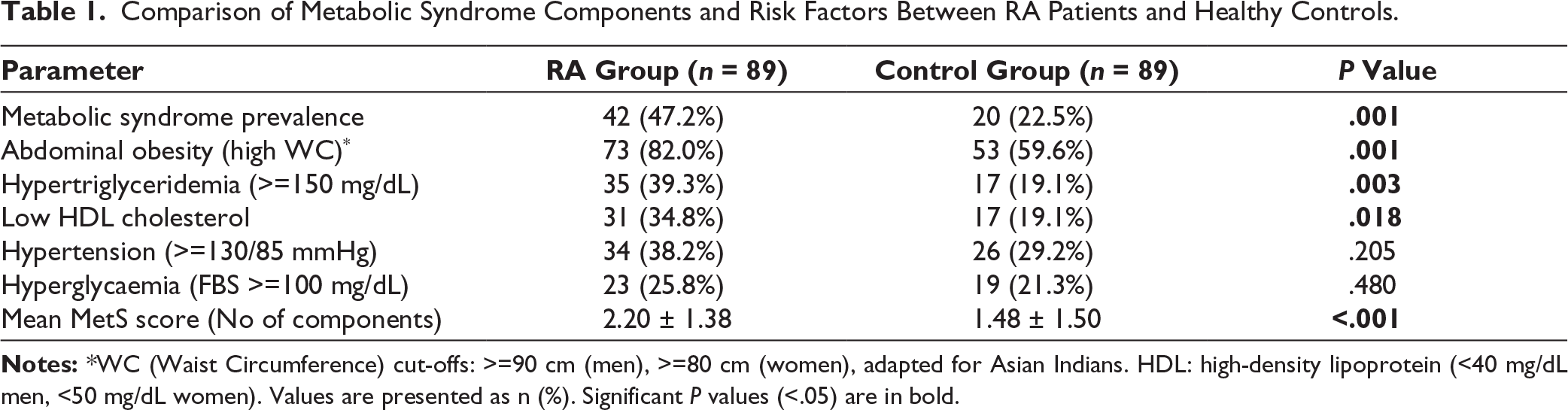
The prevalence of MetS was significantly higher in the RA group (47.2%, n = 42) compared to the control group (22.5%, n = 20) (P = .001). This prevalence is notably higher than the 31.6% reported in a comparable North Indian cohort, 3 reflecting the distinct metabolic high-risk status of the Kerala population. The metabolic profile was driven primarily by abdominal obesity and dyslipidaemia (Table 1). A striking 82% of RA patients had central obesity compared to 59.6% of controls (P = .001). This aligns with the concept of ‘rheumatoid cachexia’, where systemic inflammation drives muscle wasting while promoting visceral fat deposition. 4 Furthermore, RA patients exhibited the characteristic ‘lipid paradox’, with significantly higher triglycerides (P = .003) and lower HDL (P = .018) despite comparable LDL levels. Within the RA cohort, MetS was strongly associated with increasing age (P = .004) and higher BMI (P = .003). Interestingly, we found no significant association between corticosteroid use and MetS (P = .124). While steroids are traditionally linked to metabolic derangements, our findings support the hypothesis that controlling high-grade inflammation may offset the metabolic side effects of low-dose glucocorticoids. 5 Disease activity (RAPID3) did not correlate with MetS (P = .286), suggesting that metabolic risk accumulation may proceed independently of acute articular symptoms.
In conclusion, nearly half of the RA patients in this South Indian cohort suffer from MetS, a rate double that of the healthy population. The alarming prevalence of central obesity necessitates that waist circumference and lipid screening be integral to routine rheumatology practice in this region to mitigate cardiovascular mortality.6,7
Comparison of Metabolic Syndrome Components and Risk Factors Between RA Patients and Healthy Controls.
Footnotes
Acknowledgements
The authors express gratitude to the staff of the Wellness Clinic for their assistance in data retrieval and to the Department of Rheumatology for facilitating patient recruitment.
Data Availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Human Ethics Committee (Ref: KIMS/IHEC/FM-02/2021).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from all individual participants included in the study.