
Abstract

A 61-year-old male presented with a two-month history of progressively worsening dysphagia, initially for solids and later for liquids, eventually becoming unable to swallow saliva. He reported significant weight loss, recurrent oral ulcers, and a firm right submandibular swelling. Concurrently, he developed progressive proximal muscle weakness affecting all limbs, with difficulty rising from a seated position, climbing stairs, turning in bed, and performing routine activities.
Clinical examination revealed classic dermatologic signs of dermatomyositis (DM), including Gottron’s papules and mechanic’s hands. Proximal muscle power was markedly reduced (upper limbs 4/5, lower limbs 1/5). Additional findings included mild pallor, glossitis, and reduced mobility. The Manual Muscle Testing-8 (MMT-8) score was 62/80, indicating severe disease. Establishing an MMT-8 baseline is essential for monitoring therapeutic response to corticosteroids, IVIG, immunosuppressants, and treatment of an underlying malignancy in paraneoplastic DM.
Laboratory tests showed elevated AST (111 IU/L), ALT (59 IU/L), CPK (865 IU/L), LDH (450 IU/L), and ferritin (848 ng/mL). ANA blot was positive for Ro-52, while anti-TIF1-γ antibody level was strongly elevated (130 U), indicating a high likelihood of associated malignancy. MRI of the neck revealed a well-defined heterogeneously enhancing nodule in the right submandibular gland. PET-CT demonstrated an FDG-avid lesion measuring 2.1 × 1.9 cm (SUVmax 4.7) adjacent to the gland, with no evidence of distant metastases.
FNAC from a right level IB lymph node showed malignant pleomorphic cells with hyperchromatic nuclei and tumour giant cells, consistent with metastatic poorly differentiated carcinoma. The patient underwent right submandibular gland excision with neck node dissection. No chemotherapy or radiotherapy was given. A PEG tube was placed due to severe dysphagia. These findings confirmed paraneoplastic DM secondary to submandibular gland carcinoma, a rare association.
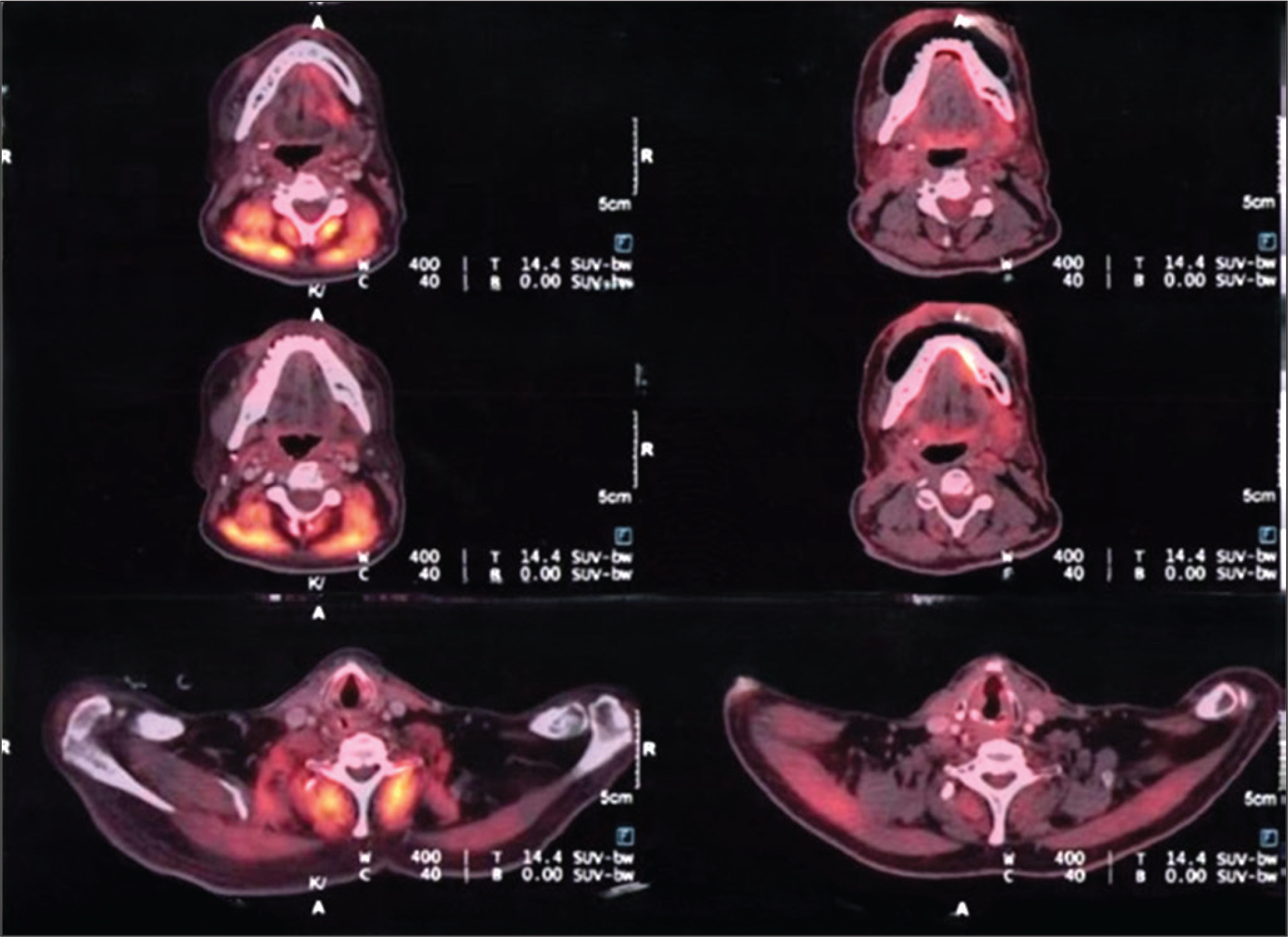
He received pulse methylprednisolone (1.5 g over three days), followed by IVIG (25 g/day for five days) and two rituximab infusions (1 g each, given 15 days apart). Maintenance therapy included monthly IVIG, rituximab every three months (contrary to the usual practice of six-monthly rituximab in order to achieve adequate clinical response), and daily Wysolone with hydroxychloroquine, following recommendations from the ProDERM trial (2021) and EULAR guidelines. Gradual improvement in bulbar symptoms and limb strength allowed PEG removal and initiation of physiotherapy. On follow-up, upper limb strength improved to 4/5, with modest gains in the lower limbs, and cutaneous manifestations remained in remission. The MMT8 score that was 62/80 initially became 78/80 after treatment. CPK was 1930 IU/L, LDH 136 IU/L on follow-up. A repeat PET-CT one year later showed complete resolution of previous abnormal FDG uptake in the paraspinal muscles (Figure 1).
PET Scan Images Showing Muscle Involvement Before and After Treatment with Rituximab and IVIg.
DM is an idiopathic inflammatory myopathy characterised by proximal muscle weakness and typical skin findings. In adults over 50, 15%–25% of cases are paraneoplastic. Anti-TIF1-γ antibodies are strongly linked to malignancy, with cancer detected in up to 60%-80% of seropositive individuals, making comprehensive cancer screening essential.
IVIG plays a major therapeutic role in moderate to severe or refractory DM. The ProDERM trial demonstrated significant improvement in 79% of patients receiving monthly IVIG, supporting its use alongside corticosteroids and immunosuppressants.
This case emphasises the importance of prompt malignancy evaluation in older adults with DM, particularly when symptoms are rapidly progressive. Although uncommon, submandibular gland carcinoma should be considered a potential underlying malignancy. Early tumour management combined with immunomodulatory therapy can substantially improve outcomes in paraneoplastic DM.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Consideration
The case report titled ‘A rare presentation of paraneoplastic dermatomyositis with severe bulbar involvement secondary to submandibular gland malignancy’ has been reviewed and approved by the Institutional Ethics Committee of Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
The study was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments (as revised in 2013).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the patient for publication of clinical details and images. The patient understands that identifying information will not be disclosed and that consent cannot be revoked after publication.