Assessment of Coronary Artery Abnormality in Children with Multisystem Inflammatory Syndrome at 1 Year of Follow-Up
Akanksha
PGIMER Chandigarh, India
Introduction: Multisystem inflammatory syndrome in children (MIS-C) is a hyperinflammatory condition temporally linked to COVID outbreak. Coronary artery abnormalities (CAAs) affect 13–26% of patients at initial presentation. Mid to long term outcomes of these CAAs are unknown, this study aimed to do follow-up assessment of these CAAs, 1 year after diagnosis.
Methodology: This is an observational study, conducted in the Paediatric Allergy Immunology Unit, Advanced Paediatrics Centre, PGIMER, Chandigarh, between July 2023 - Dec 2024. In this study, 24 children with MIS-C who had CAAs at presentation, or had severe disease during the acute phase, were enrolled and observed at least 1 year of follow-up. Children who fulfilled the criteria were enrolled; clinical details were recorded and patient underwent TTE and CTCA at the same day. CAAs were assessed according to AHA guidelines. None of the patient required sedation as a part of the procedure. This study was approved by the Institutional Ethics Committee (IEC). None of the adverse effects were encountered during study.
Results: In this study, mean age at diagnosis was for 24 enrolled patients was 7.4 ± 3.1 years, with a median follow-up interval of 30 (12–40.7) months. At follow up mean age was 10.1 ± 3.1 years. At diagnosis 50% of children had CAA. At follow-up regression rate of these CAAs was 54.1%. Regression for small aneurysms is 78.5%, for medium aneurysms is 50%, and 1 giant aneurysm detected at diagnosis, regressed to a medium aneurysm at follow-up.
Conclusions: This study concludes that 54% of CAAs regress in children with severe initial presentation with MIS-C and that assessment of coronary artery status was comparable in both CTCA and TTE, yet CTCA, with radiation optimisation techniques, demonstrated a clear advantage. This study also sheds light on the mid to long-term fate of CAAs at approximately 2.5 years of follow-up in children with MIS-C. To the best of our knowledge, this is the longest duration of a follow-up study conducted on children with MIS-C, the only study conducted using both TTE and CTCA for the assessment of CAAs.
Keywords: Multisystem Inflammatory Syndrome in Children (MIS-C), Coronary Artery Abnormalities (CAAs), CT Coronary Angiography (CTCA), Transthoracic Echography (TTE), Follow-up
OPO2
Intraarticular Triamcinolone vs Subcutaneous Inj. Adalimumab (TNF-inhibitor) in Inflammatory Knee Osteoarthritis: an Open Label Randomized Clinical Trial
1Department of Clinical Immunology and Rheumatology, Institute of Postgraduate Medical Education and Research (IPGMER), Kolkata, India. 2Department of Radiology, Institute of Postgraduate Medical Education and Research (IPGMER), Kolkata, India.
Introduction: Emerging evidence suggests that inflammatory cytokines like TNF play a critical role in OA pathogenesis and symptom persistence. This study evaluates the efficacy of subcutaneous Adalimumab (ADA)versus intra-articular corticosteroid in inflammatory knee OA with inadequate response to conventional therapies.
Materials and Methods: This open-label, randomized controlled trial was conducted at the Department of Clinical Immunology and Rheumatology, IPGMER, Kolkata, from February 2024 to April 2025 after IEC approval and CTRI registration. A total of 74 symptomatic primary inflammatory knee osteoarthritis patients (age 40–75) were randomized 1:1.
Group A (n = 37): Adalimumab (ADA) 40 mg SC every 4 weeks × 3 doses
Group B (n = 37): Single intraarticular Triamcinolone (IACS) 40 mg
Results:
Primary Outcome: At 12 weeks, mean WOMAC pain scores were 46.2 ± 14.2 (ADA) vs 60.4 ± 6.9 (IACS), p = 0.213 (NS). However, both groups showed significant within-group pain reduction from baseline (p < 0.001).
Secondary Outcomes: At 4 and 6 weeks, IACS showed superior pain relief (p < 0.01). By week 12, ADA showed sustained and greater pain reduction.
OARSI/OMERACT Response at 12 Weeks: High improvement was observed in 27% of patients in the IACS arm and only 2.7% in the ADA arm. moderate response was seen in 61.8% of the IACS group and 79.4% of the ADA group.
Safety: Both treatments were well-tolerated. Minor infections occurred in 3 ADA patients; 3 IACS patients reported increased post-injection knee pain.
Predictors of non-response: Higher Kellgren–Lawrence grade predicted poor response. Fibromyalgia showed a trend toward association with non-response (OR = 3.86, p = 0.068).
Conclusion: Intraarticular Triamcinolone provided rapid but short-lived symptom relief in inflammatory knee osteoarthritis, whereas subcutaneous Adalimumab demonstrated a slower onset yet more sustained improvement in pain, stiffness, function, and patient global assessment.
1Department of Clinical Immunology & Rheumatology KGMU, Lucknow, India.
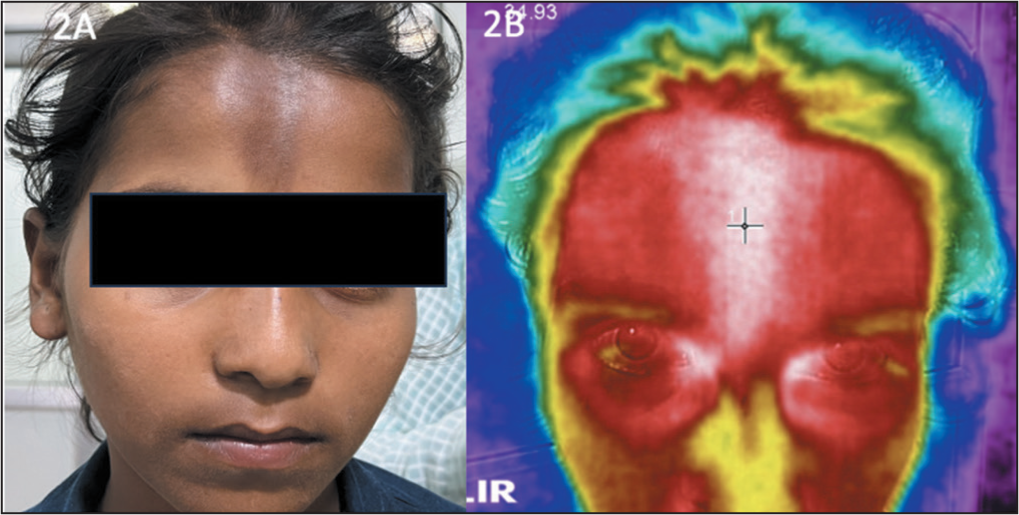
Introduction: This pilot study investigates the potential of Infrared Thermography (IRT) to differentiate active disease from damage in localised scleroderma by correlating temperature measurements with LoSCAT (Localised Scleroderma Cutaneous Assessment Tool) indices, addressing LoSCAT’s limitations in detecting subtle changes.
Methods: In this study, 63 lesions from 25 patients with localised scleroderma were assessed using both the LoSCAT and IRT. Two independent examiners conducted the evaluations. Each lesion was scored for activity (erythema, skin thickness, new/enlarged lesions) and damage (dyspigmentation, dermal atrophy, subcutaneous atrophy) according to LoSCAT. The mean temperature (T mean) of each lesion was recorded, and the correlation between LoSCAT scores and T mean was analyzed using Spearman’s correlation coefficient.
Results: The assessment revealed a total of 26 active sclerotic lesions, 23 dyspigmented lesions, 9 dermal atrophy lesions, and 5 subcutaneous atrophy lesions. 22 out of 26 sclerotic lesions (84%) exhibited increased temperature, while 16 out of 23 dyspigmented lesions which were marked as damage (70%) showed increased temperature. Additionally, 5 out of 9 dermal atrophy lesions (56%) and 3 out of 5 subcutaneous atrophy lesions (60%) had increased temperature.
Conclusion: IRT revealed active inflammation in many sclerotic and dyspigmented lesions classified as damage by LoSCAT, indicating the tool’s limitations in distinguishing activity from damage in localised scleroderma. An integrated disease assessment tool combining clinical evaluation and advanced imaging like IRT is needed for accurate disease monitoring and management in localised scleroderma.
Figure 1B. Infrared Thermography Image Showing Increased Temperature over the Thickened Skin Indicating Activity.
Figure 2B. Infrared Thermography Image Showing Increased Temperature over the Dyspigmented Skin Indicating Activity.
OPO4
Repeat Renal Biopsy-Guided Evaluation of Nephron Number Changes Following Induction Therapy in Lupus Nephritis: A Prospective Study
Jagan Babu K L1, Augustine Jose1, Sreejith Parameswaran1, Srinivas BH1, Ananthakrishnan Ramesh1, Sathiya1, Kalaiselvi1, Chengappa Kavadichanda1, Molly Mary Thabah1and Vir Singh Negi1
1Department of Clinical Immunology and Rheumatology, JIPMER, Puducherry, India. 1Department of Pathology, JIPMER, Puducherry, India. 1Department of Nephrology, JIPMER, Puducherry, India. 1Department of Radiology, JIPMER, Puducherry, India.
Introduction: Lupus nephritis (LN) is a major predictor of end-stage renal disease (ESRD) in systemic lupus erythematosus (SLE). Despite clinical remission, nephron function and reserve may remain compromised. Total nephron number, and single-nephron glomerular filtration rate(snGFR) have emerged as critical markers for assessing renal health, but their changes post-induction therapy in LN remains underexplored.
Methods: This prospective study included 52 SLE patients and 35 healthy controls meeting KDIGO living donor evaluation criteria. CT urography and renal biopsies were performed for SLE patients with proteinuria to estimate cortical volume, non-sclerotic glomeruli (NSG), and GSG densities using stereological models. From these data, nephron numbers, otherwise known as non-sclerotic glomeruli (NSG), globally sclerotic glomeruli (GSG) density, and single-nephron glomerular filtration rate(snGFR) were assessed at baseline for all SLE patients and healthy controls, and after six months of induction therapy for class III, IV, V and mixed LN patients. The snGFR was calculated by dividing total GFR by nephron number.
Results: Among 52 SLE patients, 39 completed 6-month follow-up with repeat renal biopsy and CT urography. At baseline, LN patients had nephron numbers comparable to healthy controls. However, within six months, LN patients experienced significant nephron loss(median reduced to 1,628,084) and an increase in snGFR(baseline 51.96µL/min to 73.97µL/min, p < 0.001), reflecting compensatory hyperfiltration. A subgroup analysis of class III, IV, mixed LN (n = 28) showed significant nephron loss(p < 0.001), increased GSG density(p = 0.013), and a rise in snGFR from 51.08 to 73.99µL/min (p < 0.001). In contrast, class V LN(n = 11) had significant reduction in total NSG but non-significant increase in snGFR, suggesting a less pronounced hyperfiltration response
Conclusion: These findings underscore the need for individualized, more aggressive therapy to preserve nephron function and minimize glomerular damage in LN. Heightened snGFR indicate dynamic compensatory responses of nephron function, thus there is a potential role of snGFR and GSG metrics as markers for therapeutic response and long-term renal outcomes.
Introduction: Assessing disease activity in SLE is challenging due to multisystem involvement. We evaluated the performance and responsiveness of three validated indices—SLEDAI-2K, Easy BILAG, and SLE-DAS—against the Physician Global Assessment (PGA) in an inception cohort of SLE.
Methods: Baseline and 6-month follow-up data of our centre was extracted from the Indian SLE inception cohort for research database on 24-Feb-2025. Data included clinical & lab features, SLEDAI-2K, PGA (0–3 scale), and Easy BILAG grade. BILAG grades were converted to numerical values. SLE-DAS was calculated. Using PGA as the reference, the performance of other instruments was assessed. The PGA assessment was conducted independently of the other scores. Spearman’s rank correlation, Cohen’s weighted kappa and Confidence intervals were calculated.
Results: 291 patients (95% female, mean age 28.2 ± 11.1 years) were included. At baseline, median (IQR) scores were: PGA 1.0(0.5-1.8), SLEDAI-2K 12(9-18), SLE-DAS 14.7(9.3-24.2), and Easy BILAG 18(9-29). PGA showed a strong correlation with SLEDAI-2K (ρ = 0.720), Easy BILAG (ρ = 0.654), and a moderate correlation with SLE-DAS(ρ = 0.565).
The interinstrument agreement between PGA and SLEDAI-2K(κ = 0.225) and Easy BILAG(κ = 0.213) instruments was fair. However, there was only slight agreement between PGA & SLE-DAS(κ = 0.166). Change in PGA at 6 months correlated strongly with change in SLEDAI-2K(ρ = 0.669), and moderately with change in Easy BILAG(ρ = 0.595) and SLE-DAS(ρ = 0.472).
Conclusions: All three instruments were sensitive to change. SLEDAI-2K had the best performance. However, performance differed with the grade of activity, which suggests that a single instrument may not be ideal in all patients.
Clinical Features at Baseline.
Manifestations
N (%)
Fever
134 (46.0%)
Mucocutaneous
Rash
120 (41.2%)
Alopecia
188 (64.6%)
Mucosal ulcers
120 (41.2%)
Musculoskeletal
Arthritis
43 (14.8%)
Myositis
22 (7.6%)
Hematologic
Leukopenia
43 (14.8%)
Thrombocytopenia
57 (19.6%)
AIHA (active/past)
34 (11.7%)
Serositis
Pleuritis
18 (6.2%)
Pericarditis
17 (5.8%)
Renal
Proteinuria
131 (45.0%)
Active sediments
77 (26.4)
Class III/IV LN
21 (7.2%)
Neuropsychiatric
Seizure
12 (4.1%)
Psychosis
1 (0.34%)
Organic brain syndrome
3 (1.03%)
Vasculitis
6 (2.01%)
Gastrointestinal
32 (11%)
Ophthalmic
5 (1.7%)
Serological
Raised Anti-dsDNA
231 (79.4%)
Hypocomplementemia
206 (70.8%)
Change in PGA, SLEDAI-2K, Easy BILAG, and SLE-DAS at 6 Months.
OPO6
Reactive Arthritis Transcriptomics: Enriched Enterobacteriaceae-related Pathways in Synovial Fluid and in Blood is Associated with Drug-Free Remission
Avarna Agarwal1, Phanidhar D1, Sarthak Verma1, Subham R Nayak2, Prakashini MV1, Prasanta Padhan1, A. Rajkumar Patra2,Ramnath Misra1and Sakir Ahmed1
1Department of Clinical Immunology and Rheumatology, Kalinga Institute of Medical Sciences, Bhubaneswar. 2Department of Microbiology, Kalinga Institute of Medical Sciences, Bhubaneswar.
Introduction: In reactive arthritis (ReA) approximately a half of patients achieve drug-free remission (DFR), while others develop chronic disease. We aimed to identify baseline transcriptomic biomarkers predictive of drug-free remission (DFR) in ReA and undifferentiated peripheral spondyloarthritis (pSpA).
Methods: Fifty-seven patients meeting Braun criteria for ReA or ASAS criteria for pSpA (excluding IBD- or psoriasis-related disease) were enrolled. RNA sequencing was performed on baseline whole blood (n = 14) and synovial fluid (SF, n = 10). DFR was defined as symptom-free status without medications at 3 months. Differentially expressed genes (DEGs) were analysed with DESeq2, and pathway enrichment with KEGG (clusterProfiler in R). Selected DEGs were validated by qPCR (n = 14; external n = 5) using SYBRGreen-TaqMan.
Results: Of 57 patients [75% male, median age 32 (IQR 12–40)], 52% (n = 30) achieved DFR. ReA and pSpA had statistically similar transcriptomics profiles. Four DEGs in whole blood were associated with DFR: upregulated CFD, MYOM2, CYP1B1 and downregulated CACNA1l (Figure 1A). KEGG pathways enriched in DFR included endocytosis, shigellosis, and viral responses (Figure 1B). SF transcriptomics did not yield significant DEGs but showed similar pathway enrichment. In qPCR validation, CFD and CYP1B1 showed lower ΔCT values in DFR versus chronic patients but did not reach statistical significance (p = 0.2 and p = 0.055, respectively).
Conclusion: Baseline whole blood transcriptomics can predict DFR in ReA. Enrichment of microbial and viral pathways in DFR, despite absence of live pathogens, suggests a role for pathogen-associated molecular patterns (PAMPs) in disease resolution. The role of CFD and CYP1B1 needs to be elucidated.
Comparison between Whole Blood Transcriptome Profiles of Patients with Chronic Reactive Arthritis and those with Drug-Free Remission. (A) Volcano Plot Showing Differentially Expressed Genes and (B) Showing The Top 15 Enriched Pathways (Kegg).
OPO7
A Comparative Study to Evaluate The Efficacy of Tofacitinib and Adalimumab in Treating Axial Spondyloarthritis: An open Label Randomized Controlled Trial
1Department of Clinical Immunology and Rheumatology, IPGMER, Kolkata.
Introduction: Axial spondyloarthritis (axSpA) is a chronic inflammatory disorder of the spine causing pain, stiffness, and impaired quality of life. Biologic TNF inhibitors and oral JAK inhibitors have proven efficacy, but direct comparative data are scarce. This study evaluates the efficacy and safety of tofacitinib versus adalimumab in active axSpA.
Methods: 49 patients with active axSpA (BASDAI ≥4 and/or ASDAS-CRP ≥2.1) unresponsive to NSAIDs were randomized to receive adalimumab 40 mg biweekly subcutaneously or tofacitinib 5 mg twice daily orally for 16 weeks. Primary outcome was ASAS20 response at week 16. Secondary outcomes included ASAS40, ASAS5/6, ASAS PR, BASDAI50, ASDAS improvements, pain scores, NSAID consumption, and ASQoL. Clinical and laboratory assessments were done at baseline, 4, 8, 12 and 16 weeks. Safety and adherence were monitored.
Results: Both groups were well matched in terms of most demographic, clinical and laboratory characteristics at baseline, except for a higher proportion of smokers and marginally higher ASDAS-CRP in adalimumab arm. At 16 weeks, ASAS20 response was achieved by 100% patients in the adalimumab group and 81.8% in the tofacitinib group (p = 0.065), demonstrating non-inferiority. Adalimumab showed significantly better outcomes in ASAS5/6 (95% vs 59.1%, p = 0.007), BASDAI50 (100% vs 77.3%, p = 0.031), ASDAS clinically important improvement (100% vs 77.3%, p = 0.031), spinal pain reduction (2.0 vs 3.45 p = 0.021). NSAID score (0.47 vs 3.81, p = 0.005). Both drugs were generally well tolerated, with only mild adverse events.
Conclusion: Tofacitinib is a safe and effective oral option, non-inferior to adalimumab by primary endpoint of ASAS20 response in active axSpA, but adalimumab offers broader, faster improvements in secondary outcomes, including quality of life and NSAID reduction. Larger studies are warranted to guide therapeutic positioning.
Patient-Led Joint Assessment in RA: A Step Toward Remote Disease Monitoring in India
Sri Lakshmi S1, Sandeep Kansurkar2and Kavita Krishna2
1Kauvery Hospital, Chennai, India. 2Bharati Vidyapeeth Medical college and hospital, Maharashtra, India.
Background: This study aimed to assess the ability of patients with rheumatoid arthritis (RA) to examine their own joints for tenderness and swelling and compare the findings with clinician assessments. Sixty-two RA patients over 18 years attending our outpatient department between October and December 2022 were included. An instructional manual with pictorial guides in English and the local language was provided. If needed, attendants assisted in comprehension. After successful pilot testing on ten patients, the same manual was used uniformly. Patients marked tender and swollen joints, scored pain, difficulty, and global assessment. A blinded rheumatologist subsequently conducted an independent joint evaluation. Figure 1: sensitivity and specificity of joint examination by patient
Methodology: This study aimed to assess the ability of patients with rheumatoid arthritis (RA) to examine their own joints for tenderness and swelling and compare the findings with clinician assessments. Sixty-two RA patients over 18 years attending our outpatient department between October and December 2022 were included. An instructional manual with pictorial guides in English and the local language was provided. If needed, attendants assisted in comprehension. After successful pilot testing on ten patients, the same manual was used uniformly. Patients marked tender and swollen joints, scored pain, difficulty, and global assessment. A blinded rheumatologist subsequently conducted an independent joint evaluation.
Results: A total of 559 and 499 joints were identified as either tender or swollen by clinician and patient, respectively. The sensitivity of patient-reported joint counts was 86.02%, with specificity of 95.62%. For swollen joints, sensitivity was 89.2% and specificity 96.2%; for tender joints, sensitivity was 85.04% and specificity 93.8%. Self-assessment was more accurate in proximal joints like shoulders (specificity 91.95%) and elbows (96.18%), while distal joints were better assessed by clinicians. CDAI scores showed strong correlation between clinician and patient (rho = 0.99). Intraclass correlation coefficients were 0.810 (total), 0.880 (swollen), and 0.770 (tender), indicating good reliability.
Conclusion: This study shows that with proper training; patient self-assessment of joints is a reliable alternative for teleconsultation. It is especially accurate for detecting swollen joints, supporting its use in remote monitoring. These findings advocate integrating self-assessment into telemedicine to improve access and continuity of care in rheumatoid arthritis.
Sensitivity and Specificity of Joint Examination by Patient.
Correlation between Total Number of Joints Examined by Patient Vs Clinician; 2B: Correlation between Swollen Joints Examined by Patient vs Clinician; 2C: Correlation between Tender Joints Examined by Patient Vs Clinici.
OPO9
Cardiovascular Risk Burden across Inflammatory Arthritis: A Cross-Sectional Study from National Hospital of Sri Lanka
1Department of Rheumatology, National Hospital of Sri Lanka, Colombo, Sri Lanka.
Introduction: Cardiovascular (CV) morbidity is a major contributor to adverse outcomes in patients with inflammatory arthritis (IA), including rheumatoid arthritis (RA), ankylosing spondylitis (AS), and psoriatic arthritis (PsA). Data from South Asia remain limited. This study aimed to assess the prevalence of CV risk factors among IA patients and compare findings across diagnostic groups.
Methods: A cross-sectional study was conducted on 150 consecutive patients attending the Rheumatology Department, National Hospital of Sri Lanka. Demographics, diagnosis, disease activity (mild, moderate, severe), and CV risk factors (hypertension, diabetes, dyslipidemia, obesity, smoking, prior cardiac events) were recorded. Descriptive statistics and comparative analyses (chi-square and ANOVA) were performed.
Results: Of 150 patients (mean age 52.3 ± 11.2 years; 68% female), 75 had RA, 40 AS, and 35 PsA. Hypertension was the most prevalent risk factor (46%), followed by dyslipidemia (38%), diabetes (32%), and obesity (28%). Smoking was noted in 18% (predominantly males). RA patients exhibited significantly higher rates of hypertension and diabetes compared to AS and PsA (p < 0.05). Overall, 62% of the cohort had ≥2 CV risk factors. The prevalence of CV risk factors exceeded rates reported in the general Sri Lankan population, aligning with global IA trends.
Conclusion: Cardiovascular risk factors are highly prevalent among Sri Lankan patients with IA, particularly in RA. RA patients exhibited significantly higher rates of hypertension. Proactive screening and risk reduction strategies are critical to improving long-term outcomes.
1Department of Clinical Immunology and Rheumatology, Bharati Vidyapeeth (DTU) Medical College and Hospital, Pune, Maharashtra - 411043.
Introduction: Post-viral arthritis (PVA) is a common sequela of arboviral infections such as chikungunya virus and dengue virus, particularly during epidemics. While most cases resolve within weeks, a significant proportion may progress to persistent arthritis. This study aimed to identify predictors of persistence and assess the role of hydroxychloroquine (HCQ) in treatment.
Methods: We conducted a prospective cohort study during a 2024 epidemic in Western India. Adults presenting with new-onset arthritis following a febrile illness were enrolled. Demographic, clinical, and serological data were collected. Patients were followed up at six and ten weeks. Persistence was defined as continued joint symptoms requiring corticosteroids at follow-up. Statistical analysis was performed using chi-square tests and receiver operating characteristic (ROC) curve analysis.
Results: Of 178 enrolled patients, 151 completed six-week follow-up; 53 (35.1%) had persistent arthritis. Elevated erythrocyte sedimentation rate (ESR >31 mm/hr) and rheumatoid factor (RF) positivity were significantly associated with persistence (p < 0.05). Hydroxychloroquine use did not significantly influence recovery rates (p > 0.99). At ten weeks, 41 of 49 patients with prior persistence had recovered. Recovery was more likely in dengue virus–positive patients compared to chikungunya virus–positive patients (p = 0.030).
Conclusion: One-third of patients with PVA developed persistent arthritis beyond six weeks. Elevated ESR and RF positivity may predict persistence. Hydroxychloroquine did not confer additional benefit.
1Department of Clinical Immunology and Rheumatology, Bharati Vidyapeeth Medical College, Pune, India.
Introduction: Connective tissue diseases (CTDs) are chronic autoimmune disorders characterized by the pathological production of autoantibodies, with anti-nuclear antibodies (ANAs) recognized as crucial biological markers for their diagnosis and for monitoring disease activity. While the detection of serum ANA (SerANA) by indirect immunofluorescence (IIF) remains the established gold standard, its reliance on invasive venipuncture poses practical challenges for frequent assessment. Saliva, an easily accessible and non-invasive biofluid, notably mirrors systemic physiological states and thus presents a promising and patient-friendly alternative for ANA detection.
Methods: This hospital-based cross-sectional study was designed to evaluate the diagnostic and monitoring utility of salivary ANA (SalANA) detection via IIF in a cohort of 74 patients definitively diagnosed with various connective tissue diseases, alongside 30 healthy control individuals. Patients were systematically classified based on current established criteria, such as the 2019 ACR/EULAR criteria for Systemic Lupus Erythematosus. Disease activity for each patient was carefully assessed and categorized as either ‘active’ or ‘stable’. Saliva samples were meticulously collected using Salivette→ devices, while serum was obtained through standard venipuncture. Both biological fluids underwent simultaneous ANA assay using EuroImmun ANA 100T (HEp-2/Primate Liver) kits, with fluorescence patterns interpreted according to the internationally recognized ICAP nomenclature. Statistical analyses, including chi-square tests and Spearman’s rho correlation, were employed to determine associations and relationships between variables. This project was supported by a research grant from the Indian Rheumatology Association (IRA/2023/12).
Results: The study found that all 74 recruited CTD patients were SerANA-positive, and among these, a substantial (i.e. 52) 70.27% also exhibited SalANA positivity. This translated to a high specificity of 93.33% for SalANA in differentiating CTD patients from healthy controls. Quantitative analysis revealed a moderate, yet statistically significant, correlation between SalANA and SerANA titers (Spearman’s rho = 0.43, p = 0.002), with an even stronger correlation observed for immunofluorescence intensities (Spearman’s rho = 0.54, p < 0.001). Furthermore, there was a remarkably high observed agreement (96.2%) in fluorescence patterns between salivary and serum ANA. Crucially, SalANA positivity demonstrated a significant association with active disease status within the patient cohort (p = 0.022), and specific ANA patterns, notably the homogenous pattern, were significantly linked to the presence of renal involvement (p = 0.02).
Conclusion: In conclusion, salivary ANA testing by IIF exhibits significant diagnostic and monitoring potential for connective tissue diseases, particularly in systemic lupus erythematosus. It demonstrates a compelling correlation with traditional serum ANA assays regarding titers, intensities, and critical fluorescence patterns. Moreover, SalANA shows promise in differentiating between active and stable disease states and identifying specific clinical manifestations like renal involvement. This non-invasive diagnostic approach could serve as a valuable and convenient adjunct to conventional serum assays, thereby enhancing patient management, especially in scenarios where frequent or difficult blood sampling is a concern.
1Department of Internal Medicine, Postgraduate Institute of Medical Education andResearch, Chandigarh (India). 2Department of Paediatrics, Advanced Paediatrics Centre, Postgraduate Institute of MedicalEducation and Research, Chandigarh (India). 3Department of Immunopathology, Postgraduate Institute of Medical Education andResearch, Chandigarh (India).
Introduction: Systemic sclerosis (SSc) is a complex autoimmune disease characterised by widespread fibrosis, vasculopathy, and immune dysregulation. Despite recent advances, the molecular mechanisms underlying SSc pathogenesis remain poorly defined.
Materials and Methods: Seven adult-onset SSc patients and their controls were recruited. Whole blood miRNA (84 miRNAs involved in human fibrosis) and their targeted mRNA (TGF-β1, CCL5, CXCL9, CCL19, CCL2, Smad1, TLR 7 and 9) transcripts were identified by miScript miRNA PCR Array and RT2 Profiler PCR Array using RT-qPCR.
Results: Fourteen miRNAs showed significant differential expression in SSc patients compared to controls. Of these, six were upregulated (miR-145-5p,miR-150-5p,miR-18a-5p,miR-195-5p, miR-223-3p,miR-29c-3p), and eight were downregulated(miR-211-5p,miR-217,miR-31-5p,miR-328-3p,miR-335-5p,miR-382-5p,miR-449a,miR-661)(Figure 1). DIANA-Mir Path v3.0 Pathway analysis revealed enrichment in TGF-β signaling, cytokine–cytokine receptor interaction, ECM-receptor interaction, PI3K-Akt, mTOR, and Epstein-Barr virus infection pathways (Figure 2). Ingenuity Pathway Analysis predicted miRNA–mRNA interactions, including miR-145-5p, miR-18a-5p, and miR-449a targeting TGFβ1 (Figure 3). Gene expression validation showed upregulation of TGFβ1 (5.49-fold; p < 0.04), TLR7 (5.97-fold; p < 0.01), TLR9 (3.61-fold), Smad1 (5.96-fold; p < 0.005), CCL5 (7.13-fold; p < 0.03), CXCL9 (3.75-fold), and CCL19 (3.18-fold). CCL2 showed no significant change (1.10-fold) (Figure 5).
Conclusion: The differentially expressed miRNA and their putative mRNA targets (hsa-miR-145-5p, hsa-miR-18a-5p, hsa-miR-449a-TGFβ1 gene) in associated pathways may provide diagnostic biomarkers and point to therapeutic targets for SSc.
Gene Expression Profile of 84 miRNAs.
Bar Diagram Presenting fold change in mRNA Expression of TGF-β1, TLR7, TLR9, Smad1, CCL19, CCL5, CXCL9, and CCL2 Genes in SSc Patients, Denoted as Group 1 and Healthy Controls. (*p < 0.05, **p < 0.01, ***p < 0.001).
OPO13
Neuroenteroimmune Regulator BST1gene Polymorphism rs4273468 (A/G) is Associated with Fibromyalgia in A Dominant/Recessive Model
Junior Research Fellow, SGPGIMS, Lucknow. Associate Professor, Christian Medical College, Vellore. Senior Research Fellow, SGPGIMS, Lucknow. Professor, SGPGIMS, Lucknow
Introduction: Oxytocin secreting parvocellular neurons suppress pain through projections to brain and spinal cord besides endocrine action. Optogenetic activation of Oxytocin neurons relieved pain in a rodent Fibromyalgia model. Hence, we studied SNPs rs4273468, rs3796863 and rs1556314 in genes BST1 (CD157), CD38 and TRPM2 genes involved in hypothalamic Oxytocin secretion.
Methods: Patients diagnosed as Fibromyalgia using ACR1990 and/or ACR2016 criteria and consenting to genetic study were included. Healthy subjects with no widespread pain or connective tissue disease or medical comorbidity were taken as controls. DNA was extracted by phenol-chloroform method. Genotyping was done by TaqMan real time PCR. All continuous variables among baseline characteristics are expressed in mean (SD) and comparison by one way ANOVA while Fisher’s exact test was used for frequency tables. Odds Ratios and confidence intervals were estimated using Logistic Regression using a recessive minor allele (G) model using STATA14
Results: 118 FMS patients (88% female) of age of onset 35 (± 9.6) years and 118 healthy controls (78% female) of age 34.7 (± 10.9) years were included. Clinical features and comorbidities of patients are given in Table 1. Of the 118 patients, 74 were classified Fibromyalgia by both ACR2016 and ACR1990 criteria while 33 and 11 subjects were classified by ACR2016 and ACR1990 alone respectively. All three SNPs were in Hardy Weinberg equilibrium. BST1 rs4273468 (A/G) polymorphism was associated with Fibromyalgia in a dominant-recessive model with Odds Ratio of 17.06 (2.54-730.4, P < 0.001). CD38 rs3796863 and TRPM2 rs1556314 did not show any association.
Conclusion: This is the first study showing association of BST1/CD157 with Fibromyalgia. This SNP rs4273468 has previously been associated with Idiopathic Restless Leg Syndrome. BST1 involved in stem cell function, neuroinflammation and gut health requires further study.
Reference: Huang Y, Wang P, Luo Q, Ma J. Association of BST1 polymorphism with idiopathic restless legs syndrome in Chinese population. Sleep Breath. 2021 Dec;25(4):1987-1993
Keywords: Fibromyalgia, BST1, CD157, rs4273468
Clinical Features of FMS Subjects.
Clinical feature
FMS (n-118)
1990 ACR (n-11)
1990 + 2016 ACR (n-74)
2016 ACR (n-33)
p-value
Female
104 (88%)
11 (100%)
64 (86%)
29 (87%)
0.6
Age (years)
40.6 (± 10.3)
40 (± 11.8)
39.7 ( ± 10.4)
42.9 ( ± 9.4)
0.3
Age at onset (years)
35 ( ± 9.6)
34 ( ± 10)
34.3 ( ± 9.8)
36.9 ( ± 9)
0.4
WPI
14.6 ( ± 3.6)
12.9 ( ± 4.6)
15.5 ( ± 3)
12.9 ( ± 3.6)
< 0.01
SSS
7.8 ( ± 2.5)
2.7 ( ± 1.4)
8.6 ( ± 2.1)
7.9 ( ± 1.7)
< 0.01
TP
12.3 ( ± 5)
13.6 ( ± 2)
15.1 ( ± 2.3)
5.5 ( ± 3.4)
< 0.01
OSA (STOP BANG)
38 (32%)
1 (9%)
23 (31%)
14 (42%)
0.1
CFS
44 (37%)
1 (9%)
33 (44%)
10 (30%)
0.06
PTSD
19 (16%)
0
15 (20%)
4 (12%)
0.2
RLS
13 (11%)
0
8 (10%)
5 (15%)
0.4
Genotype Analysis.
Gene
SNP
Patients
Controls
PValue
BST1
rs4273468
AA
AG
GG
AA
AG
GG
P = 0.001
49
68
1
44
58
15
CD38
rs3796863
GG
GT
TT
GG
GT
GT
P = 0.844
54
47
17
54
50
14
TRPM2
rs1556314
GG
GT
TT
GG
GT
TT
P = 0.220
1
32
85
5
26
87
OPO14
Exosomes and CX3CR1+T Cell Subsets as Molecular Markers for Disease Progression in Systemic Sclerosis
Josna Joseph1*, Abarna R2, Manna Sera Jacob1, Sandhya Rani B3, Reka K4, Phaneendra D5and John Mathew1*
1Department of Clinical Immunology & Rheumatology, CMC Vellore, Tamil Nadu, India. 2Department of Pathology, CMC Vellore, Tamil Nadu, India. 3Centre for Stem cell Research, CMC Vellore, Tamil Nadu, India. 4Department of Biostatistics, CMC Vellore, Tamil Nadu, India. 5Department of Hematology, CMC Vellore, Tamil Nadu, India.
Introduction: Exosomes and miRNAs are involved in pathogenesis of Systemic Sclerosis(SSc), but their role in disease progression is not much known. Since the pathogenesis of SSc involve lymphocyte infiltration and fibrosis, the role of circulating CX3CR1 + T cells which are capable of homing to different organs needs to be investigated.
Methods: Exosomes were isolated, characterised for their size (Nanosight/TEM) and surface markers (CD9/CD81by flow cytometry) and quantitated from serum (Exostep) of diffuse Systemic Sclerosis patients (n = 23) who met the classification criteria and compared with that of healthy controls (HC)(n = 10). Circulating Cx3CR1+ T cell subsets were analysed from whole blood by flow cytometry and miRNA 21 and 483 were quantitated by droplet digital (dd) PCR from patients and HCs. The measured parameters were statistically compared between patients and HCs and correlation analysed with clinical profile, mRSS, disease onset and no. of organs involved.
Results: The isolated Exosomes are of < 150nm in size meeting ISEV guidelines. Exosome levels are significantly higher in the diffuse SSc patients (M = 81.5) than HC (M = 63.2), whereas correlation could not be observed between exosome counts and mRSS. There was increased expression of miR21 in SSc patients when compared to the controls. There is difference in CX3CR1+ T cell population (%) between SSc patients and HC. Among the T cell subsets, CD8 effector memory cells and CD8 Terminally differentiated T cells (TEMRA) expressed CX3CR1 the most when compared to CD4 T cell subsets.
Conclusion: Exosomes and regulatory miRNA levels may be a potential indicator of disease progression and organ involvement in Systemic Sclerosis. CX3CR1 expressing effector memory CD8T cells and CD8 TEMRA cells are crucial in SSc pathogenesis by homing to different organs and manifesting the pathological changes.
Keywords: Exosome, SSc, CX3CR1, TEMRA, CD8 T cells, miRNA
OPO15
A Single-Centre Retrospective Study of ANCA-Associated Vasculitis Presenting as Diffuse Alveolar Hemorrhage: Patient Characteristics, Serology, and Outcomes
Background/Aims: Diffuse alveolar hemorrhage (DAH) is a life-threatening complication of ANCA-associated vasculitis (AAV), often presenting with hemoptysis, dyspnea, and respiratory failure. It significantly increases morbidity and mortality. This study evaluates the demographics, clinical features, serological profiles, treatment approaches, and outcomes of patients with AAV-related DAH.
Methods: This retrospective observational study included adult patients diagnosed with AAV per 2022 ACR/EULAR criteria from August 2017 to January 2025, following ethics approval. DAH diagnosis was based on clinical signs, diffuse alveolar infiltrates, hemoglobin drop, hypoxia, and bronchoalveolar lavage when feasible. Data collected included demographics, clinical features, ANCA serology, Birmingham Vasculitis Activity Score (BVAS), treatment details, and outcomes. Statistical analysis used Student’s t-test and Chi-square test, with p < 0.05 as significant. Induction and maintenance therapies were analyzed, along with the incidence of relapse and mortality. Patients were followed for a median duration of 42 ± 7.2 weeks.
Results: Of 160 AAV patients, 39 (24.4%) developed DAH. Mean age was 47.5 ± 18.6 years; 61.5% were male. c-ANCA and PR3 positivity were predominant (71.8% and 76.9%). Renal involvement was seen in 82.1%, with rapidly progressive renal failure in 53.1%. Most received cyclophosphamide (79.5%) or rituximab (17.9%) for induction; one died before treatment. Plasmapheresis was used in 10.3%. Maintenance therapy included rituximab (59.3%) and azathioprine (34.3%). Mortality occurred in 17.9%, and 23% experienced relapse. Median BVAS was 21 ± 7.1. Upper respiratory (53.8%), ophthalmic (20.5%), and musculoskeletal (17.9%) involvement were also observed.
Conclusion: DAH occurred in nearly one-fourth of AAV patients, with high morbidity and 17.9% mortality. Most patients had renal and upper airway involvement. Prompt diagnosis and aggressive immunosuppression—including cyclophosphamide, rituximab, and plasmapheresis—improved outcomes. Continued monitoring is essential due to significant relapse risk and treatment-related complications.
Diffuse Alveolar Haemorrhage (n = 39)
%
N
Mean Age years (+/- SD)
47.5( ± 18.6)
Male gender
24
61.54%
ANCA IFA
c-ANCA
28
71.79
p-ANCA
9
23.07
Atypical ANCA
2
5.12
ANCA LIA
Anti Proteinase-3
30
76.92%
Anti Myeloperoxidase
9
23.08%
Renal
32
82.05%
Nephritic syndrome
5
15.36%
Nephrotic Syndrome
1
3.1%
RPRF
17
53.12%
Nephritic-Nephrotic
1
3.1%
Asymptomatic haematuria
8
25%
Skin Rash
10
25.64%
Digital infarct
3
7.69%
Arthritis
7
17.9%
Upper Respiratory tract
Paranasal sinus
10
25.64%
Conductive hearing loss
3
7.69%
Sensorineural hearing loss
4
10.25%
Subglottic stenosis
1
2.56%
Otitis media
3
7.69%
Myocarditis
1
2.56%
Scleritis/Episcleritis
7
17.9%
Inflammatory pseudotumour
1
2.56%
keratitis
1
2.56%
Induction
CYC
31
79.48%
RTX
7
17.95%
Maintenance
N = 32
RTX
19
59.37%
AZA
11
34.37%
LTF
2
6.25%
OPO16
Clinical and Laboratory Characteristic of RA-ILD Patients: Single Centred Study
1Medanta- The Medicity, Gurugram, Haryana, India. 2Kolhapur Rheumatology Center, Maharashtra, India.
Introduction: Rheumatoid arthritis-associated interstitial lung disease (RA-ILD) is a significant extra-articular manifestation of RA with substantial morbidity. This study aims to characterize the demographic, clinical, serological, radiographic, and therapeutic features of RA-ILD patients at a single tertiary care center.
Methods: This retrospective observational study included 80 RA-ILD patients diagnosed using ACR/EULAR 2010 criteria, with ILD confirmed by clinical, HRCT, and/or PFT findings between 2022 and 2025. These patients were compared to 821 RA patients without ILD. Data on demographics, disease duration, DAS28, serological markers (RF, ACPA, ANA), inflammatory markers (CRP, ESR), extra-articular manifestations, comorbidities, radiological features, PFTs, and treatment patterns were analyzed. Statistical significance was determined using p-values, with p < 0.05 considered significant.
Results: RA-ILD patients were older (62.38 ± 9.80 vs 54.89 ± 12.01 years, p < 0.0001) and had longer RA duration (10.86 vs 8.64 years, p = 0.0002). They had slightly higher disease activity (DAS28-ESR, p ≈ 0.03), lower RF positivity (70% vs 86.6%, p < 0.001), but similar ACPA and ANA levels. Inflammatory markers, joint deformities (26.25% vs 2.43%), extra-articular manifestations, osteoporosis, and comorbidities were more frequent. HRCT showed UIP and NSIP patterns. Restrictive PFTs and greater biologic/tsDMARD use were noted.
Discussion: RA-ILD is associated with older age, longer disease duration, higher inflammation, more deformities, and greater extra-articular involvement. RA-ILD patients have distinct serological and radiological profiles and are more likely to require advanced therapies. These findings underscore the need for vigilant screening for ILD in RA patients, especially those with risk factors, to facilitate early diagnosis and optimize management.
1Medanta The Medicity, Gurugram, Haryana, India. 2PGIMER, Chandigarh. 3St. Johns Bangalore, India. 4KD Hospital, Ahmedabad. 5MGIMS, Maharashtra.
Background: Rheumatology Clinical Trial Network, funded by BIRAC (Ref: BT/NBM0257/05/19), was established to create a GCP-compliant framework for efficient, cost-effective clinical trials in rheumatology. Led by Medanta, Gurgaon, it collaborates with five leading institutions: MGIMS (Maharashtra), CARE (Kerala), SJNAHS (Bangalore), KD Hospital (Ahmedabad), and PGIMER (Chandigarh).
Objective: To strengthen clinical trial infrastructure and develop a unified rheumatology disease registry to facilitate high-quality research and industry collaborations.
Methods: A gap assessment evaluated site resources, equipment, and processes, with gaps addressed through SOP development, equipment procurement, manpower training, and EC registration. A web-based Health Plug Registry was implemented for standardized patient data entry. Network activities included four investigator meetings, site monitoring, remote audits, and World Bank visit (May 2023). A dedicated website was launched to engage stakeholders.
Results: The network enrolled 14,339 patients across major rheumatologic conditions: RA (7,515), SLE (1,720), Psoriatic Arthritis (927), Spondyloarthritis (1,912), Sjogren’s Syndrome (576), Systemic Sclerosis (714), ANCA-associated Vasculitis (317), Aortoarteritis (308), and Myositis (350). Currently, 25 sponsored and two investigator-initiated trials are ongoing. Three milestone registry reports were submitted (Jan 2022, Dec 2022, Sep 2023). Eight publications highlight key findings, including DMARD therapy in rheumatoid arthritis, anti-synthetase syndrome, and renal involvement in ANCA-associated vasculitis.
Conclusion: CTN-Rheumatology has established a robust platform for rheumatology research, with significant patient enrolment and active trials. The Health Plug Registry supports real-world evidence generation, while publications underscore the network’s scientific impact. Future efforts will expand trial portfolios and global partnerships.
Effect of Birth Trauma on Magnetic Resonance Imaging (MRI) Of Sacro-iliac Joints in Early Post-Partum Period: A Case Control-Study
Shyamashis Das
Institute of Neurosciences Kolkata, Kolkata, India.
Introduction: Imaging of sacro-iliac joint (SIJ) during postpartum may show bone marrow edema (BME), which may be confused with sacroilitis. This study aimed to estimate the prevalence of SIJ BME among postpartum women and determine whether this BME following childbirth can be differentiated from sacroiliitis of patients with axial-spondyloarthritis (ax-SpA).
Methods: In this prospective observational study, subjects were recruited in four groups - (1) women having uncomplicated term vaginal delivery (VD) of singleton fetus with cephalic presentation, (2) women underwent elective cesarean (CS) section, (3) nulliparous healthy females (NP), and (4) patients of ax-SpA respectively. Pregnant women after delivery having low backache with Visual Analogue Score (VAS) score (0-10 scale) ≥3 were included.
SIJ MRI was done within 7 days of childbirth in VD and CS group and following recruitment in NP and ax-SpA group. MRI images were examined by a blinded rheumatologist and a blinded radiologist separately.
Results: Total 68 women including 24 VD, 24 CS and 20 NP and 20 ax-SpA were recruited. Prevalence of BME suggesting of ‘acute sacro-ilitis’ was 32.4% among postpartum women with low back ache. Both VD group and CS group significant inflammatory changes in MRIs of SIJs when compared with healthy controls (p-value for VD < 0.01, p-value for CS < 0.01). No significant difference was found in Imaging findings of SIJs including BME, sclerosis, synovial effusion, erosions, capsulitis, sclerosis between VD and CS groups. The κ value for interobserver agreement for BME in MRI of postpartum women was 0.80 (SE 0.13, 95% CI 0.542 to 1.000). However, mean SPARCC score to assess sacroiliac joint inflammation was significantly more in the spondyloarthritis group compared with the postpartum women group (22 ± 12.5 vs. 7 ± 7.5, P < 0.0001)
Conclusion: BME in MRI of SIJ in postpartum women may be mis-interpreted as sacroiliitis. Pregnancy, as a state of altered physiology, itself may cause postpartum inflammatory changes in SIJ MRI irrespective of mode of delivery.
OPO19
Prevalence of Oral Manifestations In Systemic Sclerosis Patients and Their Association With Clinical and Serologic Profile – A Case Control Study
Dr. R N Tejaswini1, Vijaya Prasanna Parimi1, Dr. Pradeep S. Anand1, Dr. Vineetha Shobha2, Dr. Padmanabha Shenoy3, Dr. Geetabali4, Dr. Ramaswamy Subramanian5, Dr. Mahabaleshwar Mamadapur5, Dr. Shinie Razil Goveas6, Dr. Biswarup Sengupta7, Dr. Caseena8, Dr. Sakshi Das9and Dr. Anitha Subbappa10
DrNB Resident, Department of Clinical Immunology & Rheumatology, ESIC Medical College and Super Specialty Hospital, Sanathnagar, Hyderabad. HOD, Department of rheumatology, St Johns medical college, Bangalore. Director, Centre for rthritis and Rheumatism, Kochi. Prof. & HOD, IPGME&R, Kolkata. Professor and Head, Dept of Clinical Immunology and Rheumatology, JSS Medical College, JSS Academy of Higher Education and Research, Mysuru. Assistant Professor Department of dental surgery St John’s medical College hospital Bangalore. Associate Professor and Head of the Department, Department of Dentistry, IPGME&R, Kolkata. Department of Dentistry, Centre for arthritis and rheumatism, Kochi. MDS, Senior Resident, Department of Dentistry, ESIC Medical College, Hyderabad. Reader, Dept of Periodontology, JSS Dental College & Hospital, JSSAHER.
Introduction: Systemic sclerosis (SSc) is a chronic autoimmune disease with widespread vascular and fibrotic changes. Orofacial manifestations—affecting up to 80%—include microstomia, xerostomia and periodontal disease, impairing oral function, hygiene and social well-being. Often overlooked compared to visceral involvement, these features warrant systematic evaluation and patient education for prevention and management.
Methodology: A case-control study involving 111 SSc patients and matched healthy controls was conducted at five centers in India to assess prevalence and clinical–serologic associations of oral manifestations. Standardized questionnaires captured demographics, medical history and SSc disease duration. Patients were classified as limited, diffuse or sine scleroderma. A rheumatologist assessed Modified Rodnan Skin Score; xerostomia inventory, mouth handicap questionnaire. Hand function was assessed using the Indian Cochin Hand Function Scale. Medsger’s score evaluated disease severity. Relevant laboratory, imaging and serology data were recorded. A trained periodontist examined SSC patients and matched healthy controls for dental indices (DMFT, probing depth, attachment loss).
Results: Of 111 SSc patients, 65.8% had limited and 34.2% diffuse cutaneous disease. SSc patients had significantly reduced mouth opening (22.5 vs. 39.3 mm), fewer teeth (21.3 vs. 25.9), higher gingival bleeding (56.7% vs. 32.3%), greater periodontitis prevalence (73.9% vs. 41.4%), deeper probing depth (5.13 vs. 3.45 mm) and more clinical attachment loss (4.36 vs. 2.01 mm). Sites with attachment loss ≥3 mm (72.5% vs. 55.6%) and ≥5 mm (36.3% vs. 18.8%) were more frequent in SSc (all p < 0.05), while oral hygiene scores showed no significant difference. No significant serological associations were found.
Conclusion: Orofacial manifestations in SSc cause significant functional impairment yet remain under-recognized. Early detection, patient education, and clinician awareness about prevention and dental hygiene are essential to improving quality of life in this chronic multi-systemic disease.
Introduction: Palindromic rheumatism is a rare, episodic arthritis marked by sudden joint pain and swelling that resolves fully between attacks. Its variable course, overlap with other diseases, and lack of validated criteria cause diagnostic challenges. This study evaluates and compares existing diagnostic frameworks for PR in a defined patient cohort.
Method: A cross-sectional observational study was conducted at Dr Shenoy’s CARE Clinic, Kochi, over a one-year period (2023–2024). The study enrolled 402 participants, including 302 patients diagnosed clinically with PR and 100 control patients with other diseases who had intermittent joint symptoms. Baseline demographic data, clinical features, and serological markers such as rheumatoid factor (RF), anti-CCP antibodies, and ANA were recorded. Radiographic findings were also noted where applicable. Diagnostic performance of each criterion set was assessed using sensitivity, specificity, positive predictive value, negative predictive value, and ROC curve analysis. Cohen’s kappa statistics were used to assess agreement between criteria.
Results: Among 402 participants, PR cases were predominantly female (70.5%) with a mean age of 46.8 years, and 64.6% were RF or anti-CCP positive, challenging its traditional seronegative label. González-López criteria had perfect sensitivity (100%) but very poor specificity (14%). Pasero and Barbieri criteria showed high specificity (85%) but very low sensitivity (13.9%). Hannonen criteria had moderate sensitivity (48.3%) and low specificity (36%), while Guerne and Weisman criteria showed similar sensitivity (45.7%) with slightly higher specificity (50%). ROC analysis showed poor diagnostic performance for all frameworks (AUC 0.43–0.57), indicating no existing criteria balance sensitivity and specificity effectively.
Conclusion: Current diagnostic criteria for PR lack the optimal balance of sensitivity and specificity. The González-López criteria were highly sensitive but poorly specific, whereas the Pasero and Barbieri criteria missed most cases. Findings support PR as frequently seropositive rather than merely a precursor to RA. There is an urgent need for validated, consensus-based criteria incorporating clinical and serological features.
ROC Analysis And AUC Interpretation of PR Diagnostic Criteria.
OPO21
Subclinical Synovitis And Enthesitis in Patients With Psoriasis: A Pilot Study Evaluating the Utility Of Musculoskeletal Ultrasound
Meera S N1, Christy P1, John Mathew1, Vineeth Abraham3, Madhavi K3, Dharshini S2, Dhincy Peter2and Ashish Jacob Mathew1
1Department of Clinical Immunology and Rheumatology, Christian Medical College, Vellore. 2Department of Dermatology, Venereology and Leprosy, Christian Medical College, Vellore. 3Department of Radiology, Christian Medical College, Vellore.
Introduction: Indian data on psoriatic disease is limited, with psoriasis affecting 0.44–2.8% of the population, more commonly in males. There is growing evidence of the increased risk in PsO patients with subclinical arthritis and enthesitis for developing PsA. This pilot study explored the extent of subclinical musculoskeletal findings in psoriasis patients.
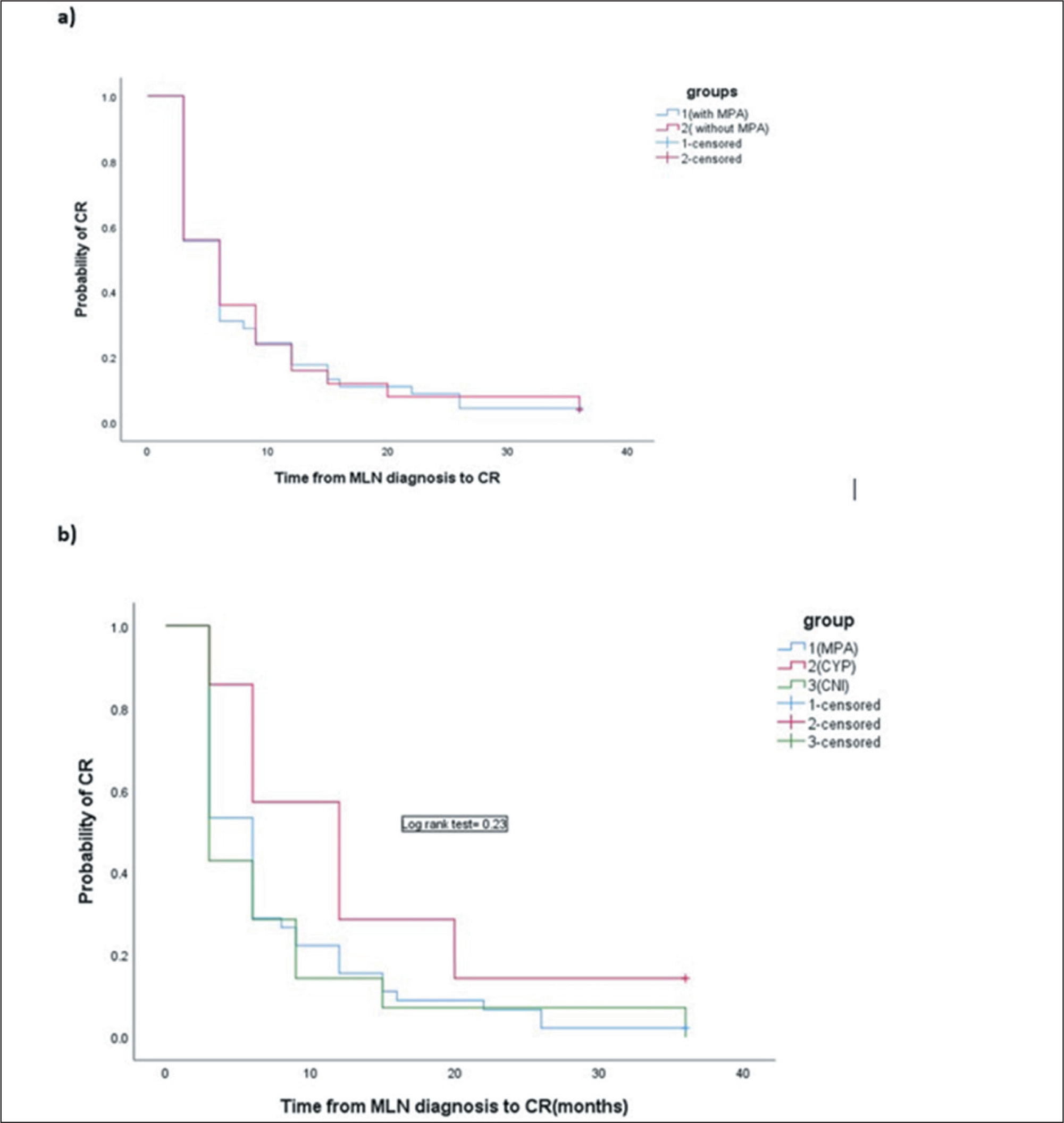
Methodology: This was a prospective observational study conducted in a tertiary care centre in South India. The study population included consecutive adults with PsO who were DMARD-naive, attending combined dermatology-rheumatology clinics at Christian medical College, Vellore, India from November 2024 to May 2025. Demographic and clinical variables, including the extent of involvement of skin disease (PASI), were evaluated in all the patients. Consenting individuals were subjected to a comprehensive clinical examination of the skin, musculoskeletal system and a standardized unbiased ultrasound examination of pre-specified joints and entheses of the upper and lower limbs by an experienced radiologist in musculoskeletal ultrasonography.
Results: A total of 35 patients with psoriasis who provided infomed consent were recruited into this study. 54% (19) were females. Mean DLQI score of participants were 6.6 (7.2). Mean TOPAS 2 score was 4 (1)Subclinical enthesitis and synovitis were noted in 12 (34%) of patients by musculoskeletal ultrasound. The most frequent sites of synovitis in ultrasound were DIP joints of hand followed by feet and knees. Enthesitis was noted in achilles tendon the most followed by plantar fascia and supraspinatus insertion. Mechanical enthesophytes were noted in achilles tendon in 6 (16%) patients. Tenosynovitis was noted in flexor tendons of hands.
Baseline Characteristics of Patients included in the study.
Baseline characteristic
Mean age (SD)
44.9(15)
Males, n(%)
16 (46%)
Mean duration of skin psoriasis in months (SD)
52months(42)
Family history of psoriasis, n(%)
3 (8%)
Family history of inflammatory arthritis, n(%)
1 (2%)
Smoking, n(%)
2 (5%)
History of alcohol use, n(%)
2 (5%)
Dyslipidemia, n (%)
5 (14%)
Diabetes mellitus, n(%)
7 (20%)
Hypertension, n(%)
9 (25%)
History of arthralgia, n(%) Mean duration of arthralgia (SD)
15 (43%) 4months (12)
Mean Body mass Index (SD)
25 (4.2)
Presence of Nail psoriasis, n(%)
16 (45%)
Scalp involvement, n(%)
19 (54%)
Mean PASI score (SD)
4.3 (5.8)
Mean Body surface area involvement (SD)
16 (23)
Musculoskeletal Ultrasound Findings.
N (%)
Synovitis
7 (20%)
Tenosynovitis
2 (5%)
Enthesitis
6 (14%)
Bony erosion
1 (3%)
Conclusion: ubclinical enthesitis and synovitis were noted in 12 (34%) of patients by musculoskeletal ultrasound. Longitudinal studies have confirmed that psoriasis patients with subclinical ultrasound findings later develop overt PsA. This approach may help prevent or delay the progression from subclinical to clinical disease, especially in high-risk individuals without joint complaints.
Mycophenolic Acid in Pure Membranous Lupus Nephritis: Does Hypoalbuminemia Impact Renal Outcomes?
Illiasul Ibad1, Ruchika Goel1, John Mathew1, Vinoi George David2, Sanjeet Roy3, Suceena Alexander2, Santosh Varughese2and Ashish J Mathew1
1Department of Clinical Immunology and Rheumatology. 2Department of Nephrology. 3Department of General Pathology, Christian Medical College, Vellore.
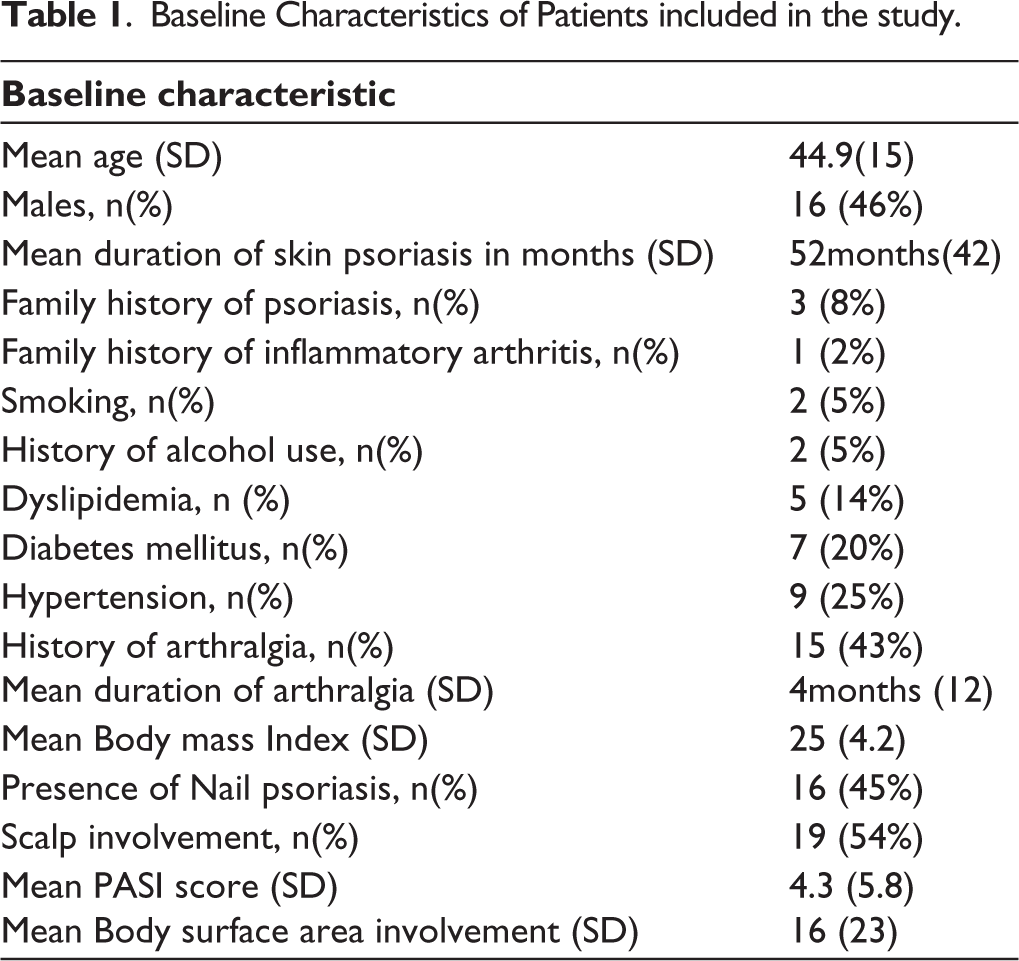
Background: Mycophenolic acid (MPA), a highly protein-bound drug, may exhibit reduced efficacy in hypoalbuminemic states due to increased free drug clearance via rapid metabolism or urinary protein-bound excretion. This study evaluated whether baseline hypoalbuminemia (≤2.5 g/dL) affects MPA efficacy in inducing complete renal remission in patients with pure membranous lupus nephritis (MLN).
Methods: Patients with biopsy-proven pure MLN, fulfilling the SLICC criteria, between January 2008 and July 2023 were included. Patients were grouped by induction regimen (MPA or non-MPA: cyclophosphamide, calcineurin inhibitors, azathioprine) and serum albumin level (≤2.5 or >2.5 g/dL). Primary outcomes were complete renal remission (CR) at 6 and 12 months, time to CR, relapse, and long-term renal survival. CR was defined by 24-hour proteinuria ≤500 mg/day with stable renal function per EULAR/ERA-EDTA criteria. Disease activity was assessed using SLEDAI. Kaplan–Meier curves and subgroup analyses were performed to assess the impact of albumin and treatment regimen on outcomes.
Results: Of 1100 lupus nephritis patients, 107 (9.7%) had pure MLN. After exclusions, 70 patients [60 (86%) women; median follow-up: 72 months (IQR 30–144)] were included. Forty-five received MPA; others received non-MPA therapy (cyclophosphamide: 7, CNI: 14, azathioprine: 4). Time to CR was similar across groups (median 6 months, p = 0.97). In the MPA group, severe hypoalbuminemia (≤2.5 g/dL) was associated with lower CR at 6 months (p = 0.033), not observed in the non-MPA group (p = 0.168). CKD was more common with non-MPA therapy (p = 0.014). MPA led to earlier CR in those with proteinuria ≤1000 mg/day.
Conclusion: In pure MLN, severe hypoalbuminemia adversely impacts the short-term efficacy of MPA. Although MPA, CYC, and CNI were similarly effective in achieving CR, MPA was associated with lower CKD progression. Baseline serum albumin should be considered when selecting induction therapy, particularly when using MPA.
Kaplan Meier Estimates Probability of CR In Different Time Periods and According to Different Treatment Regimen.
Treatment Response Variables and Long-Term Outcomes in MPA and Non- MPA Group.
OPO23
Antibodies to Type I and Type III Interferons at Diagnosis Predispose to Serious Infections on Follow up in an Inception Cohort of SLE (INSPIRE) from India
1Department of Clinical Immunology and Rheumatology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow. 2Department of Rheumatology, All India Institute of Medical Sciences, Lucknow.
Introduction: Patients with systemic lupus erythematosus (SLE) are susceptible to serious infections. Autoantibodies to cytokines can cause serious infections like COVID19, tuberculosis or other intracellular infections. We describe antibodies to type I, II and III interferons(IFNα, ω, γ & λ) as a cause for infections in an inception cohort of SLE(INSPIRE).
Methods: Newly diagnosed SLE (SLICC 2012 criteria) within 6 months of disease onset were enrolled in the INSPIRE cohort from 2018-2023. We developed ELISAs for antibodies to IFN α, ω, γ and λ. Baseline sera retrieved from the biobank were tested for these antibodies. Antibody titres were expressed as optical density (OD) and the 95th percentile of antibody titres in healthy-control population was used to develop cutoffs for positivity. Outcomes studied were infections in the initial 2 years of follow up. Serious infections were those that led to hospitalisation or mortality.
Results: 313 patients of SLE(294 females, mean age 27.7 ± 10.2 years) were enrolled from 2 centres in North-India. 59 healthy controls were also enrolled. Antibodies to IFN-α, ω, γ, λ were present in 73(23.3%), 18(5.5%), 18(5.5%) and 30(9.6%) patients respectively. In contrast, 3(5.08%) healthy controls had antibodies to IFN-α, IFN-ω, IFN- γ and IFN-λ each.
There were 107 infections (31 were serious infections). Antibodies to IFN-α were associated with serious infections(OR 2.79,1.29-6.04), tuberculosis(OR 3.46,1.03-11.68), viral infections(OR 2.64,1.23-5.68) and Herpes zoster(OR 3.1,1.2-8.02). Antibodies to IFN-λ were associated with associated with serious infections(OR 2.93,1.1-7.83) Antibodies to IFN-ω and IFN-γ were not associated with infections.
Conclusion: Antibodies to IFN-α are the most common anti-interferon antibody in an Indian inception cohort of SLE and predispose to serious infections, especially viral infections, Herpes zoster and tuberculosis in the initial 2 years of follow up.
Dynamic Expression of Alpha-1-Antichymotrypsin in Kidney Biopsies from Patients with Lupus Nephritis
Ram Raj Singh1,2,3,4, Meiying Wang1, Jonathan Zuckerman4and Asmaa Abu-Maziad1,5
1Department of Medicine, Division of Rheumatology, 2Molecular Toxicology Interdepartmental Program. 3Jonsson Comprehensive Cancer Center. 4Department of Pathology and Laboratory Medicine. 5Department of Pediatrics, Division of Pediatric Nephrology, University of California at Los Angeles (UCLA), Los Angeles, CA 90095, USA.
Introduction: Mechanisms of kidney disease progression in lupus nephritis (LN) is not understood. We performed quantitative proteomics of LN kidney biopsies and identified the proteinase inhibitor alpha-1-antichymotrypsin (ACT) among the most differentially expressed proteins. We analyzed its expression in different classes of LN to begin to understand its role in LN.
Methods: 85 archived formalin-fixed and paraffin embedded kidney specimens were obtained from UCLA Pathology Core Laboratory. All patient biopsies fulfilled the 2003 International Society of Nephrology/Society of Renal Pathology classification of LN. Surveillance transplant kidney biopsies with no detectable pathology were used as normal controls. Patients and controls were matched for age. Renal biopsy slices were incubated with anti-ACT antibody, followed by incubation with the anti-rabbit secondary antibody. The expression of ACT was visualized with 3,3′-diaminobenzidine. Images were captured using a light microscope (Zeiss Corporation, Germany).
Results: In control tissues, ACT showed a weak staining in the cytoplasm and brush border in proximal tubules, peritubular capillaries, and a minimal staining in glomerular endothelial cells. ACT showed an intense staining in the cytoplasm and brush border of proximal tubule and some distal tubule epithelial cells in 82% LN biopsies. In the glomeruli, ACT staining started to increase in class I/II, and then decreased in class III/III+V/IV/IV+V. In class VI, ACT levels increased again and were significantly higher as compared with controls and LN classes III/III+V/IV/IV+V. In class VI, both glomeruli and tubular presented a strong ACT staining.
Conclusion: The dynamic expression of ACT across six classes of LN provides a rationale for investigating its role in LN kidney disease progression. ACT’s differential overexpression in proximal tubule cells vis-a-vis other renal cell types might imply its possible contribution to LN pathology through its effects on renal tubular epithelial cells.
Keywords: Lupus Nephritis, Biomarker, Kidney
OPO25
Temporal Trends in Symptom Onset and Diagnostic Delay in Sjögren’s Disease: Insights from the Indian Sjögren’s Disease Registry
Anu Sreekanth1, Kriti Kishor2, Alli Sasi Preyatham3, Kunal Chandwar4, Sourabh Malviya5, Mohith Kumar Reddy6, Debanjali Sinha7, Rajnish K Singh8, Prakashini Mruthyunjaya9, Rakesh Solanki10, Mamadapur Mahabaleshwar11, Abhishek Patil12, Parthajit Das13, Sumanth Madan14, Kavitha Mohanasundaram15, Ajit Nalawade16, Maria K Eldho1, Minu Mohan1, Manju Mohanan1, Veena Ramachandran3, Matam Sri Anusha3, Abilash Krishnan V2, Avarna Agarwal9, Sarthak Verma9, Prasanta Padhan9, Sakir Ahmed9, B N Shivaprasad11, Able Lawrence4, Ramaswamy Subramanian11, Pradeepta Sekhar Patro14, Amita Aggarwal4, Deepak K Gautam8, Shyamashis Das7, Vikneswaran Gunaseelan3, Sarath Chandra Mouli Veeravalli6, Padmanabha Shenoy D1, Sapan C Pandya10, Pulukool Sandhya3for Indian Sjögren’s Disease Registry
1Centre for Arthritis and Rheumatism Excellence Kochi,Kerala. 2King George’s Medical University, Lucknow. 3Narayana Health City, Bengaluru. 4Sanjay Gandhi Postgraduate Institute of Medical Sciences,Lucknow. 5Ojas Centre for Arthritis and Autoimmune Rheumatic Diseases,Indore. 6KIMS Hospitals, Secunderabad. 7Institute of Neurosciences, Kolkata. 8BHU, Varanasi. 9KIMS Bhubaneswar. 10RheumaCARE, Ahmedabad. 11JSS Medical College Mysore. 12Manipal hospital Old Airport Road Bangalore. 13Apollo Gleneagles Hospital, Kolkata. 14 SUMS Bhubaneswar. 15Saveetha Medical College Chennai. 16Coherence Pain & Arthritis Clinics, Pune.
Introduction: The unclear natural history of Sjögren’s disease (SjD) could contribute to diagnostic delay. It is proposed that sicca symptoms typically appear first, followed by extraglandular manifestations and, rarely, lymphoma. Leveraging data from the Indian SjD Registry(ISDR), we mapped the diagnostic journey of the patient from the onset of first symptoms to diagnosis.
Methods: The ISDR consists of prospectively enrolled physician-diagnosed adult SjD patients from September 2023. A structured proforma captured the initial symptoms, diagnostic features and timelines. Those who fulfilled either of the AECG or ACR/EULAR criteria were included. IBM SPSS V21, was used for statistical analysis.
Results: Of 802 patients, 494[92.7% women, median age at diagnosis 46 years] were included. Initial presenting manifestations were non-sicca(79.7%), dry eyes(12.3%), dry mouth(6.1%), both sicca symptoms(1.9%). The median (IQR) time from onset of non-sicca to dry eyes and dry mouth was 2.9(1.6-6.5) and 3(1.1- 6.9) years, respectively. The overall diagnostic delay from initial symptoms was 3.2 (0.9,7.7) years, which was longer with non-sicca vs sicca onset (3.6 (1, 8.1) vs 2 (0.7, 4.9) p = 0.009).
Conclusion: Non-sicca is the most common initial manifestation of SjD preceding sicca by ~3 years. The median time to diagnosis was 3.2 years. Compared to sicca, the onset with non-sicca was associated with significant diagnostic delay.
Therapeutic Impact on Tear and Salivary Flow in Sjögren’s Disease: A Decade-Long Single-Centre Cohort Analysis
Vishad Viswanath1,2, Veena V Nair3, Neethi Suresh4, Arya A5 and Malu B S5
1Department of Rheumatology and Clinical Immunology, IRIS, Thiruvananthapuram and Kollam, Kerala, India. 2Department of Paediatric Endocrinology, IRIS, Thiruvananthapuram, Kerala, India. 3Medical Officer, Department of Rheumatology and Clinical Immunology, IRIS, Thiruvananthapuram and Kollam, Kerala, India. 4,5Staff Nurse, Department of Rheumatology and Clinical Immunology, IRIS, Thiruvananthapuram and Kollam, Kerala, India.
Introduction: Schirmer’s test and unstimulated whole salivary flow (USWSF) objectively assess glandular involvement in Sjögren’s Disease. Their longitudinal course and therapeutic modification remain incompletely defined.
Methods: We analysed 148 patients meeting ACR EULA 2016 criteria with baseline and follow-up Schirmer’s or USWSF (2015–2025). Inclusion required ≥2 recordings. A subgroup of patients with baseline Schirmer’s ≥5 mm in either eye or USWSF ≥0.20 mL/min was separately analysed. We compared baseline vs. last and baseline vs. average follow-up. Treatment effects (hydroxychloroquine, methotrexate, low-dose steroids, pilocarpine) were tested using Mann–Whitney U with multiplicity-adjusted p-values.
Results: Mean baseline Schirmer’s was 8.21 ± 3.45 mm (RE) and 8.34 ± 3.51 mm (LE); baseline USWSF was 0.234 ± 0.082 mL/min. Average Schirmer’s was 8.89 ± 3.67 mm (RE) and 9.02 ± 3.74 mm (LE); average USWSF was 0.247 ± 0.085 mL/min. Measurements per patient: Schirmer’s 3.2; USWSF 2.9. Pilocarpine improved average USWSF overall (p = 0.012) and in USWSF ≥0.20 mL/min subgroup (p = 0.009). Methotrexate increased average RE Schirmer’s overall (p = 0.021) and in Schirmer’s ≥5 mm subgroup (p = 0.017).
Conclusion: Pilocarpine enhanced salivary flow and methotrexate improved tear production in selected subgroups, suggesting targeted therapy can modify objective glandular function in Sjögren’s Disease.
Outcomes of Immunosuppression in Myositis-associated ILD based on Radiological Phenotypes among a Large Indian Cohort
Akshay1, Ashish J Mathew1, John Mathew1, Leena R V2, Aparna Irodi2and Ruchika Goel1
1Department of Rheumatology, Christian Medical College Vellore, India. 2Department of Radiology, Christian Medical College Vellore, India.
Introduction: Despite the clinical relevance of Interstitial lung disease (ILD) in Myositis patients, data on the long-term treatment outcomes and prognosis of Myositis-associated ILD remain limited. Outcomes of ILD has been previously linked to antibody subtypes. However, the influence of immunosuppressive therapies on the diverse radiological subtypes remains unexplored.
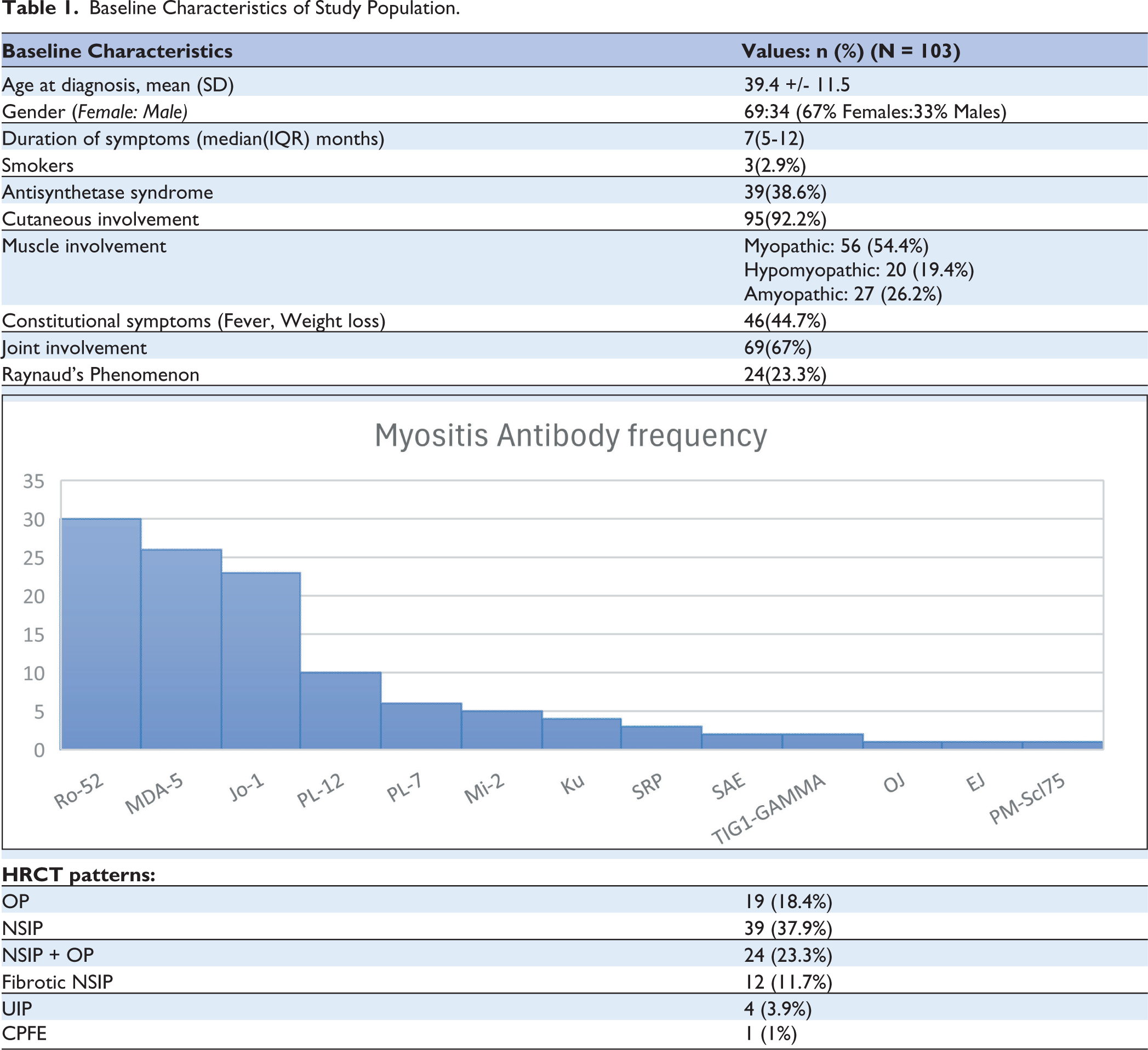
Methods: Electronic medical records of patients with Connective-Tissue-Disease(CTD) associated-ILD in our clinics between 2010 till date were screened. Among 14362 patients with CTD-associated ILD, 249 Dermatomyositis with ILD were identified and 103 patients with complete data were included. Clinical, laboratory, imaging and treatment data at index and follow-up visits were recorded. The patients were characterized by clinical presentation, antibody type, and chest imaging. Immediate outcomes were analyzed at 6 months, and long-term outcomes at the last visit for those with at least 6 months of follow-up. ILD progression was defined by FVC decline(≥10%) or radiological progression. Data was analyzed using SPSSv21.
Results: Among 103 DM-associated ILD patients(Table-1), 38.6% had antisynthetase syndrome. MDA5 and Jo-1 antibodies correlated with OP(76%) and NSIP(65%) patterns respectively. Treatment included Mycophenolate(n = 84), cyclophosphamide(n = 10), azathioprine(n = 7). Over 34(6-220)months median follow-up, 7.3%, 8.7%, and 11.9% patients had FVC decline at 6, 12, and last follow-up. Only 4.3% on mycophenolate had FVC worsening vs. 33% on azathioprine/cyclophosphamide (p = 0.034). Follow-up imaging showed 52.9% progression, 23.5% stability, and 29.4% regression. Presence of consolidation was associated with improvement(p = 0.011), while predominant fibrosis predicted progression(56%). Worsening of imaging findings linked with early FVC decline (30.4% vs 3.3%, p = 0.015). NSIP had the highest progression rate(62.5%), while OP had least(29.5%,p = 0.06).
Conclusion:.Over half of DM-ILD cases had follow-up radiological progression, however antibody subtype did not predict ILD progression. The presence of consolidation and fibrosis on CT impacted the progression of ILD in our cohort of myositis-associated ILD. Mycophenolate was associated with better outcomes than azathioprine or cyclophosphamide.
Radiological Phenotypes according to Antibody Subtype.
OPO28
Anti-Nuclear Antibody Indirect Immunofluorescence Patterns In Systemic Lupus Erythematosus: Clinical Associations, Correlation With Autoantibody Profile And Identification Using Artificial Intelligence
1Department of1Rheumatology & 5Biochemistry, All India Institute of Medical Sciences (AIIMS), New Delhi. 2Centre for Biomedical Engineering, Indian Institute of Technology (IIT), Delhi. 3Department of Clinical Immunology & Rheumatology, Sanjay Gandhi Post-graduate Institute of Medical Sciences (SGPGIMS), Lucknow. 4Department of Clinical Immunology & Rheumatology, Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER), Puducherry.
Introduction: Antinuclear Antibody test performed by Indirect Immunofluorescence is considered as the standard diagnostic test for Systemic Lupus Erythematosus (SLE) . Clinical significance of doubling dilutions, autoantibody correlation and use of Artificial Intelligence (AI) for identifying IIF patterns for ANA at various dilutions in SLE remains unexplored.
Methods: SLE patients (n = 363) were enrolled. Serum samples taken prospectively at baseline, 3 years and 5 years were tested for ANA IIF patterns at doubling dilutions (1:80 to 1:10240) and autoantibodies to dsDNA, Nucleosomes, Histones, Sm, RnP, Ro, La, Scl-70, Ribosomal-P protein were tested using ELISA (all Euroimmune, Germany). Based on the end titre positivity, IIF patterns were classified as low intensity positive (from 1:80 to 1:640 dilution) and high intensity positive (from 1:1280 to 1:10240). Correlation of ANA positivity with disease activity and specific autoantibodies was done. Automatic classification of ANA patterns (classified as ICAP patterns) was done using AI.
Results: Mixed IIF patterns are the commonest patterns and Fine speckled is the commonest individual IIF pattern. Higher intensity ANA positivity is associated at baseline with higher SLEDAI, lower complement levels, higher total number of autoantibodies, higher prevalence of autoantibodies to dsDNA, Nucleosomes, Histones, Sm, RnP and La (p < 0.05 for all) and their higher titres (p < 0.05 for all). At follow up, prevalence of mixed patterns decreases significantly. Except for autoantibodies to Ro and La, all specific autoantibodies decreased significantly at 3 and 5 years. The best performing AI model achieved a classification accuracy of 80% for ANA IIF patterns.
Conclusion: High titre ANA IIF positivity in SLE patients is associated with higher numbers and higher titres of specific autoantibodies with a good correlation with higher disease activity. Except antibodies to Ro and La, all specific autoantibodies decrease on follow-up. AI model can identify ANA patterns in SLE with good accuracy.
1Department of Rheumatology, 2Nuclear Magnetic Resonance. 3Nephrology & 4Biochemistry All India Institute of Medical Sciences (AIIMS), New Delhi.
Introduction: The treatment for Lupus Nephritis depends on the the histopathological class. No differential markers exist for different classes for diagnosis and prognosis. Serum Metabolomic profile may shed light on immunopathogenic mechanisms of proliferative (PRLN) and membranous LN (MLN) and biomarkers to assess the effect of treatment.
Methods: Renal biopsy proven patients with active LN (PRLN n = 21 & MLN n = 8) and 15 healthy controls (HC) were recruited. Mixed histopathological classes were excluded in order to assess the impact of individual classes. Disease activity was assessed at baseline and after 6 months of treatment using SLEDAI. Fasting serum samples from all the patients (at 2 time points) and HC (single sample) were collected. One dimensional CPMG experiments of serum samples were carried out at 700 MHz NMR spectrometer (Agilent, U.S.A.). Concentration of metabolites was determined using Chenomx NMR Suite 9.0 software and compared between groups using SPSS 20.0 software.
Results: PRLN patients (median rSLEDAI = 8) showed significantly decreased levels of glucose, acetate, glycolytic intermediates (lactate and pyruvate), TCA cycle intermediates (succinate and citrate), amino acids (leucine, isoleucine, valine, glycine, glutamate, proline, arginine) and ketone bodies (β-hydroxybutyrate, acetate and acetoacetate) compared to HC at baseline. The levels of these metabolites increased significantly after treatment in PRLN patients showing a dynamics towards those of HC (Figure 1). On the contrary, no metabolic alterations were seen in MLN group as compared to HC at baseline and the profile remained unaffected following therapy at 6 months also.
Conclusion: These metabolic alterations provide insight into biochemical mechanisms associated with development of PRLN as compared to MLN. Our results suggest impaired glycolysis, TCA cycle and increased utilization of ketone bodies and amino acids as energy source in PRLN. These findings have implications as immunopathogenic, diagnostic and response markers for PRLN.
Partial least Squares-Discrimination analysis (PLSDA) Score Plot of (A) Patients with PRLN (SA,∘) & MLN (SB, ∆) and; (B) Patients with PRLN at baseline (SA_B,∘) & after Therapy (SA_F,∆).