
Abstract
Mixed connective tissue disease (MCTD) is a rare autoimmune overlap syndrome. Neurological manifestations are underreported and not previously synthesised systematically. This review aims to identify and describe the spectrum, clinical presentation, diagnostic approaches, management, and outcomes of neurological manifestations in patients with MCTD reported in case reports and case series and observational studies. We did a systematic review and narrative synthesis with a total of 40 articles, out of which there were 34 case reports, one case series, two case-control studies, two cross-sectional comparative studies and one retrospective study. These articles together included a total of 149 patients. In the case reports and case series, the most common manifestation was trigeminal neuralgia, reported in 11, followed by Posterior reversible encephalopathy syndrome was reported in five cases, four cases of neuromyelitis Optica, two cases of transverse myelitis, two cases of encephalopathy, one case each of various forms of neuropathy and dropped head syndrome, subarachnoid haemorrhage, haemorrhagic stroke, sagittal sinus thrombosis, normal pressure hydrocephalus, arachnoiditis, aseptic meningitis and psychosis. To enhance patient outcomes, clinicians must continue to be on the lookout for a variety of Neuropsychiatric and Neuromuscular symptoms in MCTD.
Keywords
Introduction
Mixed connective tissue disease (MCTD) is an autoimmune disorder characterised by overlapping features of systemic lupus erythematosus (SLE), systemic sclerosis, rheumatoid arthritis and polymyositis, with high titres of anti-U1 RNP antibodies. 1 MCTD is still an underrecognised entity with only a few hundred cases recorded in each region. Prevalence studies of MCTD are still lacking in many regions. One study by Dernie et al. looked for the prevalence of MCTD and found that there were only 421 recorded cases from case records in the UK. 2 A study done on the Norwegian population showed that the incidence of multiple CTDs was 2.1 per million per year, and it is 3.3 times more common in females than in males. 3
The aetiology of MCTD is not known, but a few cases have been reported after exposure to vinyl chloride. U1-RNP complex is an intranuclear protein that is involved in the conversion of pre-mRNA to mature RNA. It constitutes three specific proteins, A, C and 70kDa, to which the anti-U1 RNP antibody binds. The main target antigen of the anti-RNP antibody is the 70kDa antigen. 4 The involvement of T cell receptors and HLA molecules in the generation of anti-U1-RNP shows the genetic association of MCTD with HLA-DR4 and DR2 phenotypes. 5
MCTD usually presents initially with nonspecific symptoms like arthralgia, myalgia, low-grade fever, and Raynaud’s phenomenon, which is the most common skin change. Other features like hand oedema, acrosclerosis, calcinosis cutis, telangiectasia and vasculitis of digits are other cutaneous manifestations. 6 Joint involvement is more severe than seen in SLE, and inflammatory myopathy often manifests as myalgia and is a rare presenting complaint of MCTD. Pulmonary involvement is common in MCTD and can be seen in up to 85% and includes pleural effusion, pulmonary arterial hypertension, interstitial pulmonary processes, pulmonary vasculitis and pulmonary thromboembolic phenomenon. 7 Cardiac involvement is seen in about 40% of the patients, and Pericarditis is the most common cardiac manifestation. 8 Central nervous system manifestation is usually rare in MCTD, and mild involvement in the form of trigeminal neuralgia, psychosis, convulsions, peripheral neuropathy and headache can be seen in about 25% of the patients. 9 Gastrointestinal involvement is seen in the form of oesophageal hypomotility, dilatation, and Gastric oesophageal reflux disease, and rarely protein-losing enteropathy. 10
Overlapping criteria for the diagnosis of MCTD have been published by Sharp, Alarcon-Segovia, Kasukawa and Kahn.1,11–13 A comparison study determined that MCTD was best identified with the Alarcon-Segovia criteria, which have 62.5% sensitivity and 86.2% specificity. 14 Although these criteria were traditionally used, in 2019, a consensus criterion was released, and at present, it is the most sensitive and specific criterion, with a sensitivity of 90.6% and a specificity of 98.4%. 15 In spite of all these available criteria, it is still unclear whether MCTD is a separate illness or a condition that overlaps with other connective tissue disorders. 6
The neurological manifestations of MCTD are less frequently reported than the other manifestations, and to date, proper evidence is lacking to describe them. Some manifestations are so rare that only a few cases have been reported so far. We conducted this systematic review to look back and collect all the available evidence of neurological manifestations that have arisen secondary to the MCTD so that we can have a consolidated picture of all the evidence in one place.
Materials and Methods
Objective of the Study
The objectives of the study are to systematically identify and describe the spectrum, clinical presentation, diagnostic approaches, management and outcomes of neurological manifestations in patients with MCTD reported in case reports, case series and observational studies.
Declaration and Protocol
This systematic review was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 16 This protocol is registered with PROSPERO, and the registration ID is CRD420251087558.
Inclusion and Exclusion Criteria
The following inclusion criteria were adopted:
Study types such as case reports, case series and observational studies. Patients of any age diagnosed with MCTD based on established criteria—Alarcón-Segovia, Kasukawa, or other authors’ criteria. Reported neurological manifestations attributable to MCTD. Articles in the English language.
The following exclusion criteria were adopted:
Review articles, editorials and letters without patient data. Unpublished research. Conference presentations. Articles with no participants stated in the study. Animal studies. Studies in which neurological involvement was due to other confirmed causes and not due to MCTD.
Search Strategy
Information Sources
The following databases will be systematically searched from the available date to May 2025:
PubMed/MEDLINE. Europe PMC. DOAJ. Reference lists of included articles.
Search Terms
Search strategy for PubMed, Europe PMC and DOAJ is provided in Supplementary File S1.
Study Selection
Two independent reviewers, RAV and RD, screened the titles and abstracts. Full texts of potentially eligible studies will be retrieved. Discrepancies were resolved by consensus and consultation with a third reviewer, RE. The process is documented in a PRISMA 2020 flow diagram (Figure 1).
PRISMA Flow Chart. Page et al., 2021. 16
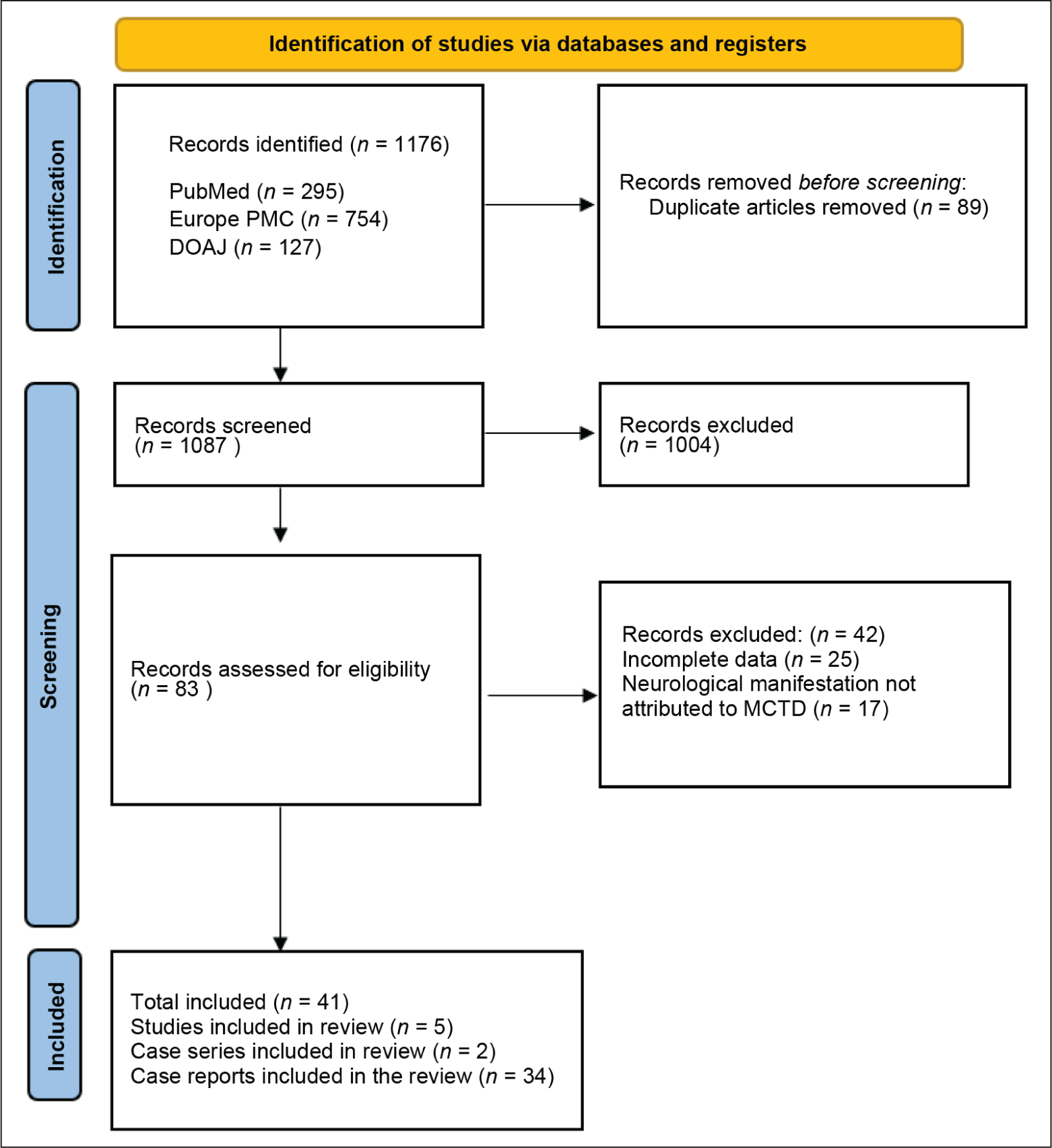
We identified a total of 1,176 articles, out of which 295 were from PubMed, 754 from Europe PMC, and 127 from DOAJ. Eighty-nine duplicates were removed, and the remaining 1,087 articles were screened. 876 articles were excluded in screening, and the remaining 83 were assessed for eligibility, out of which 25 were removed because of incomplete data, and 17 were removed because the neurological manifestation was attributed to causes other than MCTD. Finally, a total of 41 articles were included.
Data Extraction and Synthesis
Data were extracted from eligible articles into a data extraction sheet based on the PRISMA guidelines; the following criteria were collected from each study: First author, year of publication, Type of publication, Patient demographics (age, sex), Neurological manifestation, Diagnostic investigations, Treatments administered, Clinical outcomes, and follow-up. These relevant data were used to do a qualitative synthesis
Quality Analysis
We used the Joanna Briggs Institute’s critical appraisal tools to assess the quality of included papers.17,18 Selected studies were examined for inclusion criteria, sample size, description of study participants, and setting. Two reviewers independently assessed the methodological quality of each paper. Quality assessments were done with different tools based on different study designs. Risk of bias was low for 26, moderate for 6, and high for two case reports out of 34 included case reports. Meanwhile, the case series by Silva SA et al. and Maikap D et al. scored eight on a scale of 1–10 and is of moderate risk.
The detailed results of the quality assessment are provided in Supplementary file S2
Results
Quality Analysis
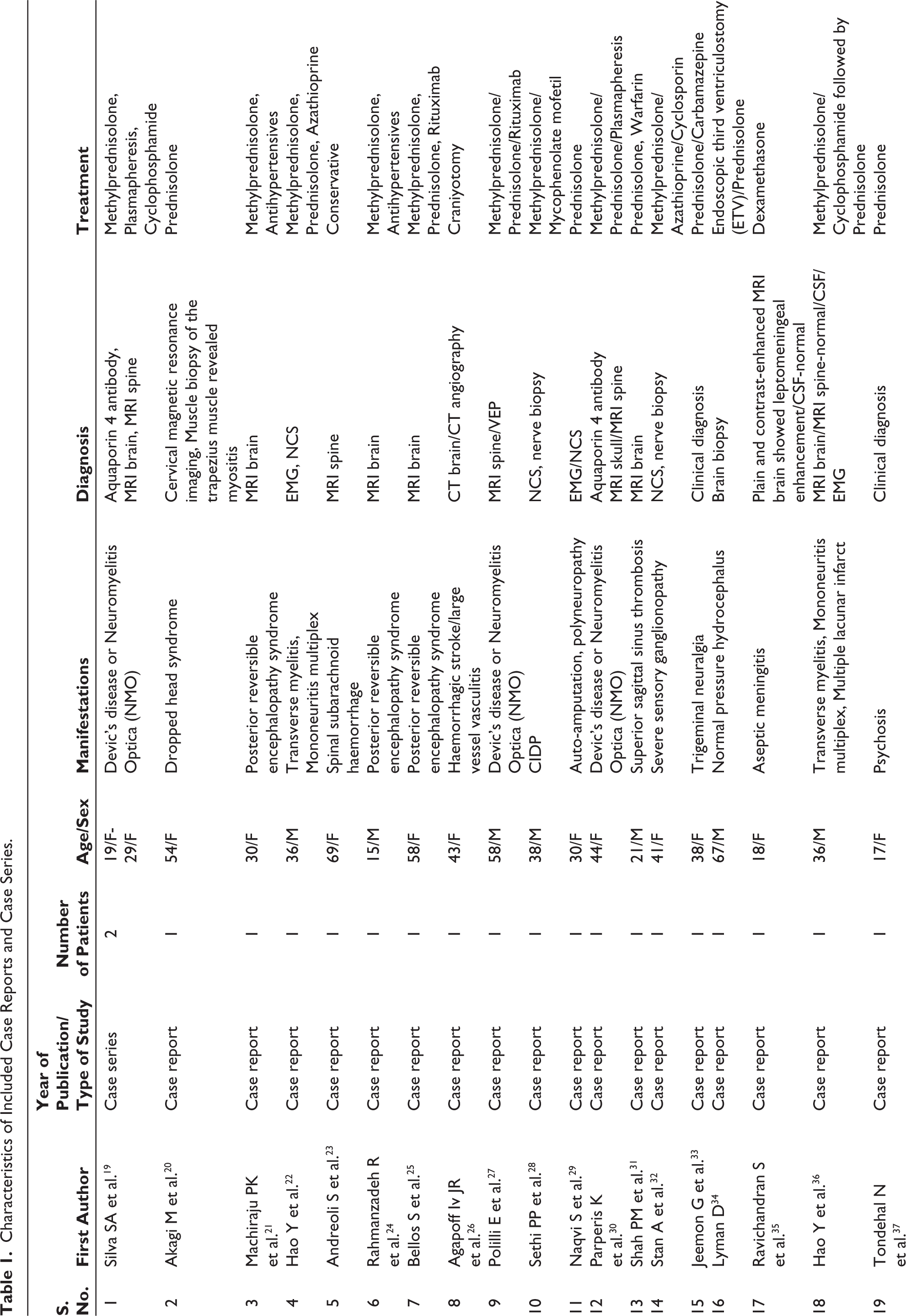
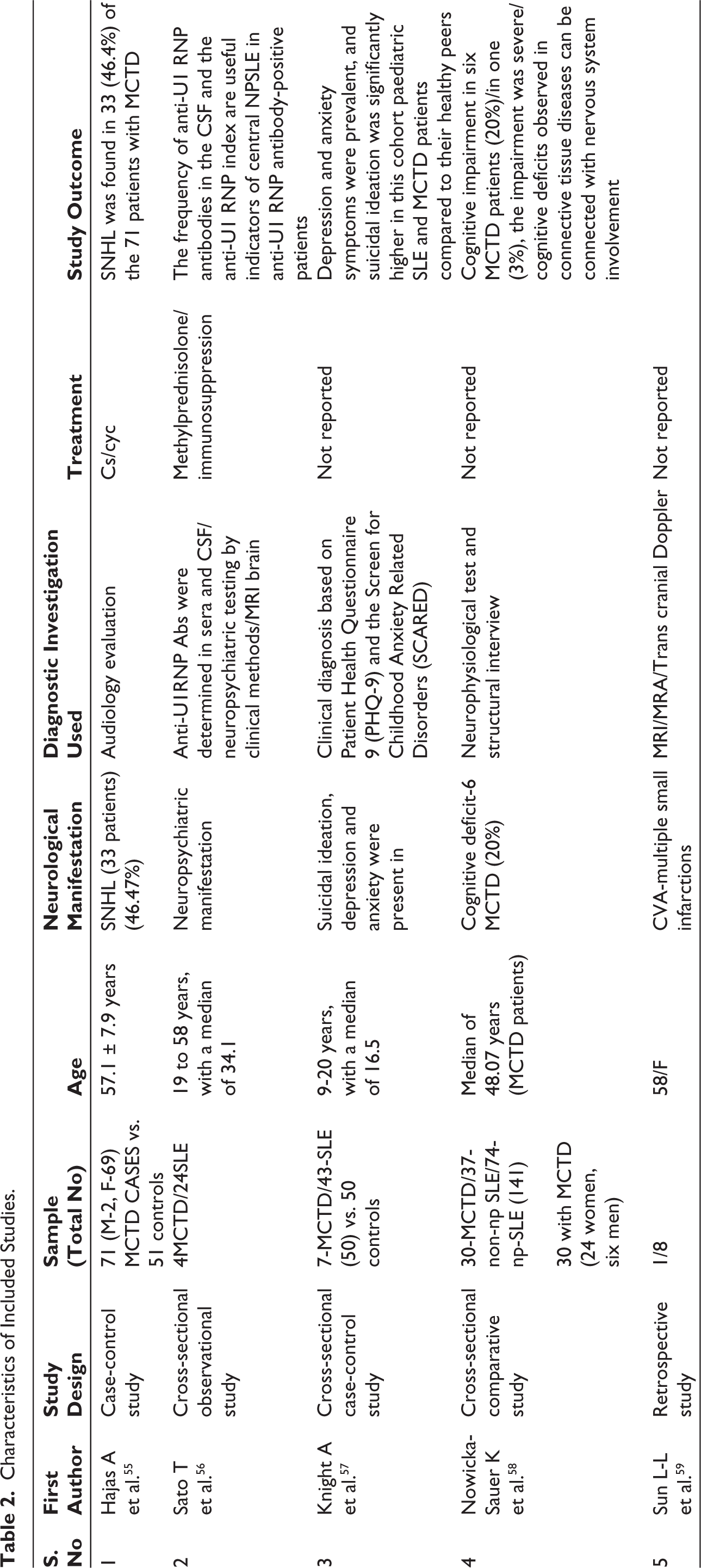
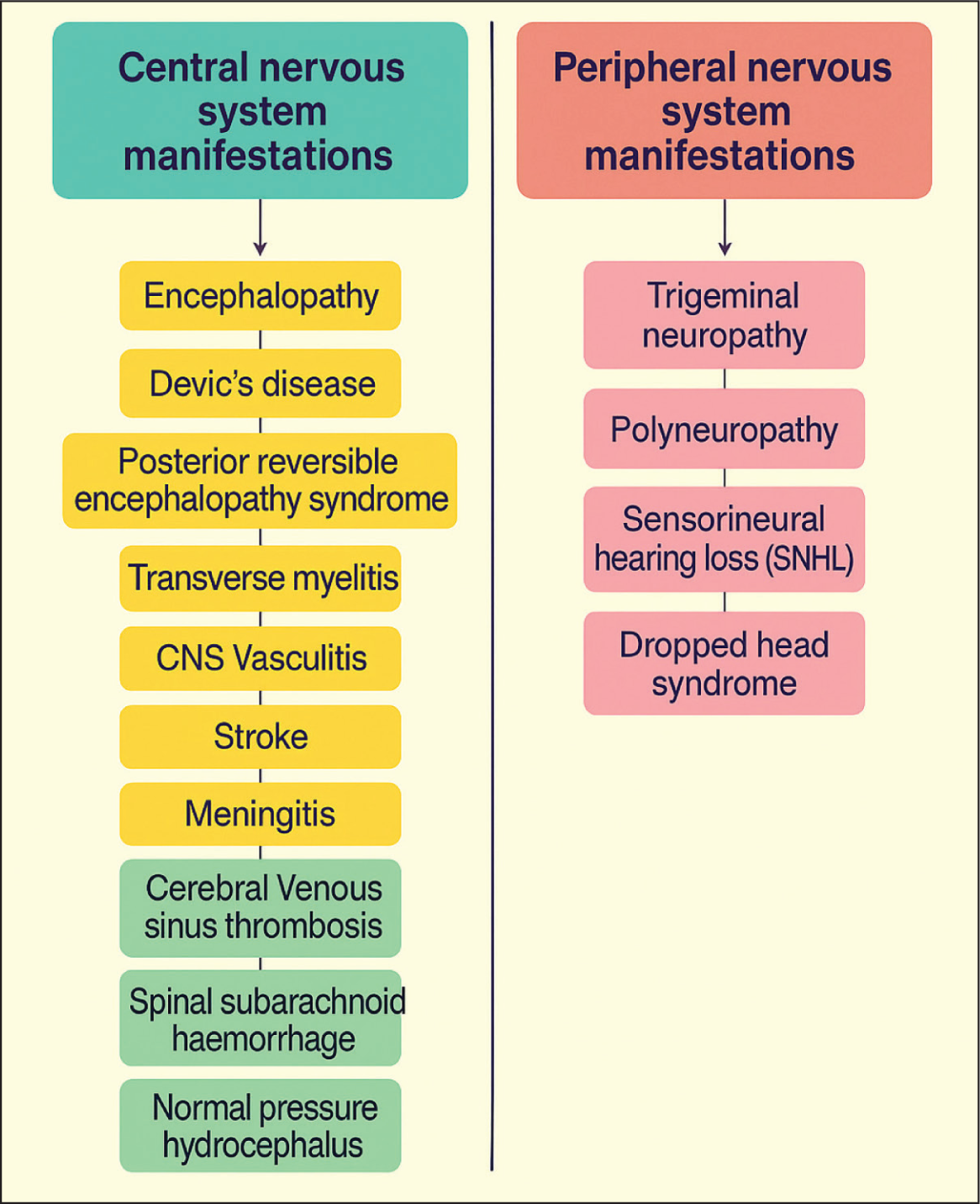
In our systematic review, we included a total of 41 articles (Tables 1 and 2), out of which there were 34 case reports, two case series, two case-control studies, two cross-sectional comparative studies, and one retrospective study. These articles together included a total of 151 patients. In the case reports and case series the most common manifestation was trigeminal neuralgia reported in 13, followed by posterior reversible encephalopathy syndrome reported in five cases, four cases of neuromyelitis Optica, two cases of transverse myelitis, two cases of encephalopathy, one case each of various forms of neuropathy like CIDP, polyneuropathy, sensory ganglionopathy, and dropped head syndrome, sub arachnoid haemorrhage, haemorrhagic stroke, sagittal sinus thrombosis, normal pressure hydrocephalus, arachnoiditis, aseptic meningitis and psychosis (Table 1). In a case-control study by Hajas A et al., 71 MCTD patients were compared with 51 healthy subjects, and the presence of SNHL was found in 33 out of 71 patients, which was 46.47%. In a cross-sectional comparative study by Nowicka-Sauer K et al., 30 patients with MCTD were studied, and it was found that 6 (20%) patients were having a cognitive decline. In a retrospective study by Sun L-L et al., out of eight patients studied for the probable mechanism of CVA, one was a case of MCTD. In a cross-sectional case-control study for studying depression and anxiety by Knight A et al., out of 50 cases studied, seven were MCTD patients, and the remaining 43 were SLE patients, and compared them with 50 controls, and it was found that suicidal ideation, depression and anxiety are more prevalent in the cohort of MCTD/SLE. In a cross-sectional observational study by Sato T et al., 24 SLE patients and 4 MCTD patients, all of them with neuropsychiatric manifestations, were included in the study and evaluated for levels of anti-U1RNP Abs in serum and CSF. It was found that the anti-U1RNP index showed 64% sensitivity and 93% specificity for central neuropsychiatric manifestations. The neurological manifestations observed in our study are summarised in Figure 2.
Characteristics of Included Case Reports and Case Series.
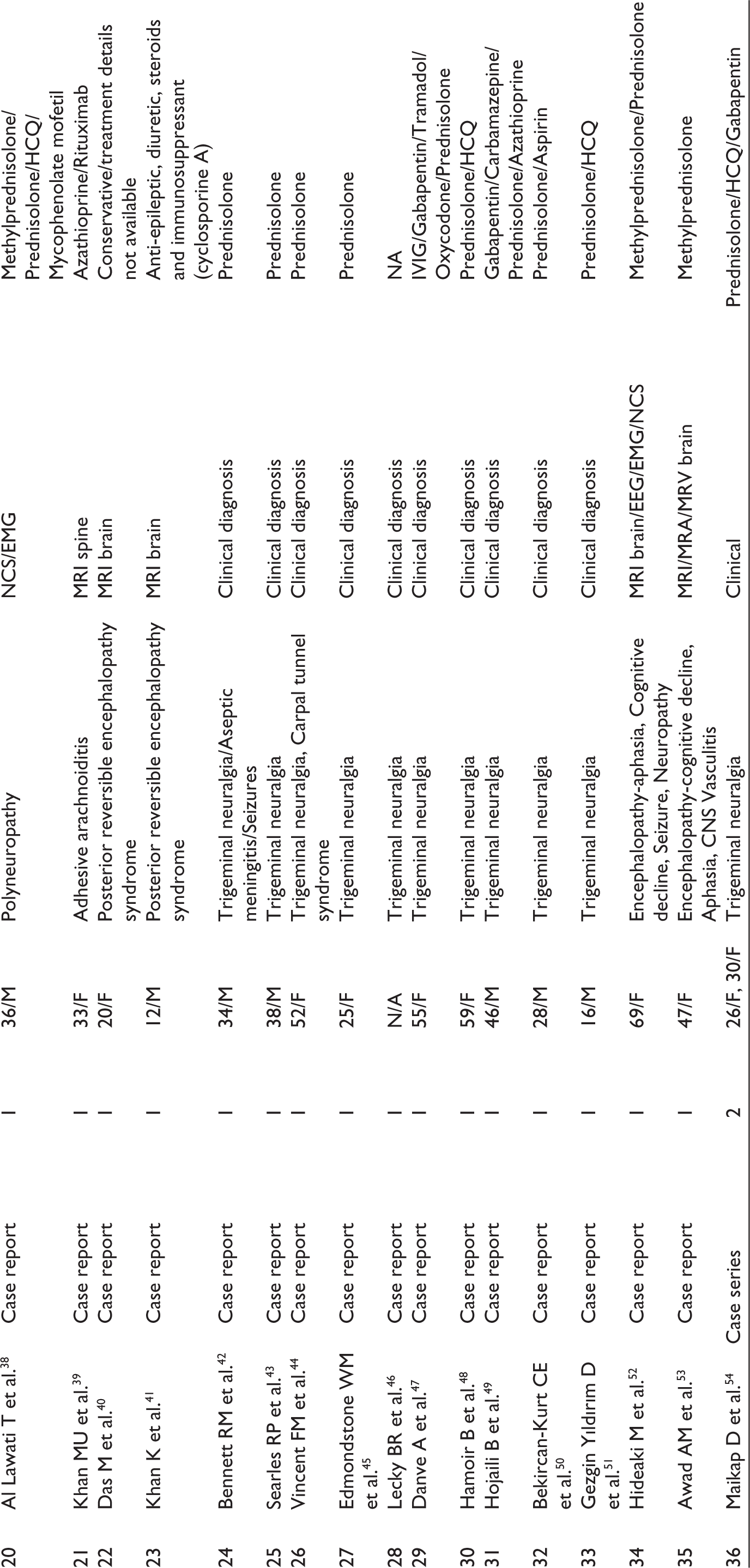
Characteristics of Included Studies.
Neurological Manifestations of MCTD.
Narrative Synthesis
Existing evidence on the prevalence of neurological manifestations of MCTD is given in the following studies. First, the study by Bennett RM et al. showed neuropsychiatric manifestations are seen in up to 25%. 9 Second, a study by Cappelli S et al. showed that neurological manifestations were seen in up to 11.2%. 60 Another study by Hajas et al. showed that the neurological manifestations are seen in up to 20%. 61
Peripheral Nervous System Manifestations
Trigeminal Neuropathy
Trigeminal neuropathy in MCTD is considered to be a common neurological manifestation, and in some cases, it is the first presentation, even before the onset of other features of MCTD, and in some other cases, it may develop during progression of the disease in follow-up. Trigeminal nerve dysfunction presents with numbness over the face and mucosa in the region of distribution of the trigeminal nerve, along with pain. 62
Trigeminal neuropathy is the presence of sensory and motor dysfunction, whereas trigeminal neuralgia is just pain over the distribution of the trigeminal nerve. Trigeminal neuropathy is mostly bilateral, and hence, presentation of bilateral trigeminal neuropathy needs further workup to rule out CTD, like MCTD.
The pathophysiology of this manifestation is postulated to be vasculitis leading to ischaemia in the nerve due to vasa nervorum interruption and compression of the nerve by fibrosis. 63 Based on cases reported so far, it was found that it may respond to steroids, and the addition of HCQ gives an added good response.33,42–51 Some cases required multiple agents like carbamazepine and gabapentin for control of pain, and one case even required IVIG to have a complete resolution.
Polyneuropathy
It is yet unknown what pathogenetic process causes polyneuropathy in MCTD. According to Adelaide et al., peripheral neuritis in MCTD patients was associated with regional vasculitis, as evidenced by myelinoclasis, axon breakdown and perivascular lymphocyte infiltration by nerve biopsy. One of the most prevalent neurological symptoms of MCTD is neuropathy. There are three forms of neuropathies associated with MCTD: treatment-related neuropathy, non-vasculitic neuropathy and vasculitic neuropathy. 64
Few cases are reported to have peripheral neuropathies as a neurological manifestation of MCTD Association of CIDP with MCTD is very rare, and only two cases are reported so far, as per the literature search.28,65 Corticosteroids and, alternatively, IVIG are preferred treatment. After being initially identified in systemic sclerosis, sensory ganglionopathy in CTD has now been connected to SLE in a few cases. Because fenestrated capillaries create a loose blood-nerve barrier that can cause ganglionitis, autoimmune attacks can impact the sensory ganglia.66,67
We found a single case of sensory ganglionopathy associated with MCTD, and the patient was started on MP pulse dose and maintenance steroids, along with steroid-sparing agents, which arrested the progression. 32
Sensorineural Hearing Loss (SNHL)
Bilateral SNHL was commonly seen in MCTD patients. The presence of Raynaud phenomenon and secondary APLA meant that patients are at high risk for developing SNHL, as these manifestations showed a positive predictive value for SNHL.
The reason for this involvement of the hearing by MCTD is not so clear, but factors like immune complex-mediated vasculitis in the inner ear are one important factor considered, and antibodies in MCTD have a role by directly damaging the inner ear structures. But considering this antibody-mediated damage, the target antigen has not yet been found. More studies are needed to find out the target and antigen and the exact mechanism for this SNHL. 55
The presence of coexisting anticardiolipin antibody in patients who are already positive for MCTD serology has the highest risk for developing immune-mediated SNHL. 68
Serum levels of antibodies like serum levels of anti-U1RNP and IgG type aCL antibodies, anti-endothelial cell antibodies, and cytokines like IFN-γ, TNF-α, and IL-10 were shown to have a significant difference with higher levels in MCTD patients than in the controls. While considering the patients with MCTD, those with SNHL had a more significant rise in IFN-γ, TNF-α, and IL-10 levels. While evaluating the percentage and the absolute number of CD4+CD25high Tregs, it was found that there is a decrease in these cells in MCTD patients with SNHL compared to patients without SNHL.
In a study by AGOTA HAJAS et al., 19 MCTD patients with SNHL were given methylprednisolone (CS) at a dose of 2 mg/kg bodyweight/day for two weeks. After a month, they were tapered to a daily dose of 10 mg. Intravenous cyclophosphamide was added to CS treatment in five patients who experienced acute hearing loss. 55
Anakinra, an anti-interleukin-1 (anti-IL-1) drug, was recently shown to ameliorate SNHL in patients with Muckle-Wells syndrome, a dominantly hereditary autoinflammatory disease. However, the role of this in MCTD is yet to be studied. 69
Dropped Head Syndrome
Dropped head syndrome is most commonly caused by isolated extensor muscle myopathy, as evidenced by one review showing 41 of 129 (31.8%) reported cases having the DHS due to it. However, the same review showed that DHS due to CTD was only 9 of 129, which accounts for 7%. 70 This autoimmune disease causing DHS will commonly be due to PM/DM, systemic sclerosis, and scleromyositis, and respond to immunosuppressive agents. 71 In MCTD cases, the commonly affected muscles are in the proximal muscles of the limbs, and involvement of cervical muscles is rare. 72 Two cases have been reported so far, having weakness of the extensor muscles of the neck, leading to a dropped neck.20,73
Central Nervous System Manifestations
Encephalopathy
One report by Matsui, Hideaki et al. showed a patient presenting with features of encephalopathy, like cognitive decline, aphasia, seizure, and gait disturbance, and was also having associated features of MCTD and was subsequently given a pulse dose of methylprednisolone followed by prednisolone maintenance dose and showed good improved of the cognition, aphasia and gait and did not have any new seizure. 52
Cognitive function decline is one of the less common manifestations of MCTD. One study by Nowicka-Sauer K et al. showed that the prevalence of MCTD was 20% and it was less severe compared to other CTDs like SLE. 57 The CTD-associated dementia is considered treatable. 74
We have evidence from Hideaki et al. that MCTD-associated dementia is also a treatable entity. Another case was reported by Amer M Awad et al., showing a 47-year-old female presenting with subacute encephalopathy with features of cognitive decline and aphasia, and the cause of this was found to be small to medium vessel vasculitis, and treatment with a pulse dose of methylprednisolone showed a modest improvement. 53
Devic’s Disease
Four cases have only been reported so far, having an association between MCTD and Neuromyelitis Optica.19,27,30 Vasculitis and thrombosis of small arachnoid arteries of the spinal cord are considered to be the pathology behind this manifestation of myelitis. 30 The association between RNP Abs and AQP4 is rare, as seen in a study by Chen C et al., who assessed the antibody profile in patients with AQP4 antibody. 75
A study by Fan R et al. showed that the presence of multiple serum antibodies, particularly antinuclear antibody positivity, is associated with earlier onset of disability. 76 The treatment is the same as other causes of Neuromyelitis Optica, starting with a pulse dose of methylprednisolone followed by immunoglobulin and plasmapheresis if refractory, and for maintenance therapy, the best drugs are azathioprine and rituximab.30,77
Posterior Reversible Encephalopathy Syndrome
PRES is commonly seen secondary to hypertension, and MCTD, causing PRES, is now reported. Five cases have been reported so far showing an association between MCTD and PRES based on a literature search.21,24,25,40,41 Out of the five cases reported, one case also had nephritic syndrome with elevated BP, so there was no clear association, and the remaining four cases did not have elevated BP or other known causes of PRES.
This association of MCTD with PRES might be due to autoantibodies causing damage to the endothelial cell, and other mechanisms considered are vasculopathy and autonomic system dysfunction. Autonomic dysfunction is commonly seen in MCTD patients, so this might also be contributing to the development of PRES. 78
Transverse Myelitis
This is one of the rare manifestations of MCTD, with only nine reported cases found in the literature search. 36 Transverse myelitis is one of the severe neurological manifestations of MCTD, and the most commonly affected area is the thoracic spine. 79
To study the pathophysiology of transverse myelitis in MCTD, Weiss et al. performed postmortem examination in cases of MCTD associated with transverse myelitis and found that there was atrophy in the level of the thoracic cord along with gliosis and necrosis involving focal areas in the spine tissue. On further examination of the cerebral tissue, it was found that there were multiple regions of necrosis along with demyelination of white matter and thickened vessels with infiltration of inflammatory cells, and based on these findings, it is considered that the mechanism of these will be vasculitis and arterial thrombosis. 80
Once the diagnosis of transverse myelitis is suspected clinically, the preferred imaging modality is MRI, which shows a hyperintense lesion on T2-weighted imaging with good enhancement, but the pitfall is that available evidence suggests that even MRI may be normal in 30% of patients with SLE and transverse myelitis, and this normal percentage of MRI in MCTD-associated transverse myelitis is yet to be studied. 81
So apart from MRI we need to look for a good clinical examination and ruling out other common causes and also look for CSF analysis which can classically show us granulocyte containing pleocytosis, increased protein and low glucose. since evidence regarding treatment of transverse myelitis is not extensive enough, in general practice the treatment which is adopted for transverse myelitis associated with SLE is followed here also and based these reported cases this treatment has shown a good response. The regimen followed is methylprednisolone pulse dose combined with cyclophosphamide, and in some other cases, azathioprine is also tried and has shown a good response. 22
CNS Vasculitis
Any small, medium, or large vessel may be impacted by secondary vasculitis, which typically indicates a dismal prognosis. Any organ system may be affected, and the presentation would change based on that. The kind and degree of presentation determine the course of treatment. 82
About 10% of people with CTD have vasculitis; the highest association rate is seen in patients with SLE. Although vasculitis is documented primarily in tiny vessels, vessels of any size may be affected. 83
Vasculitis is considered to be the mechanism for the CNS manifestations of MCTD, like encephalopathy, transverse myelitis, CVA, and neuropathy. In a literature search of CNS vasculitides in MCTD, we found a case presenting with encephalopathy and another case with haemorrhagic stroke, and management involved giving a pulse dose of steroid apart from the specific treatment for the particular manifestation.26,53
Stroke
A study by Sun L-L et al. showed that ischaemic stroke secondary to CTDs tended to involve multiple vascular territories, and the infarction volume was mostly small to medium. The areas commonly affected are cortical and subcortical areas. This rule applies to various mechanisms causing stroke in MCTD, except for one mechanism, which is CNS vasculitis, where there is involvement of a large vessel. 59
Autoimmune disease is emerging as an aetiology for stroke, particularly in young patients who do not have conventional risk factors like diabetes, hypertension, and others. Stroke due to MCTD is considered due to aetiology like hypercoagulability, cardiac embolism, and vasculitis
Involvement of multiple vascular territories is well known in stroke due to atrial fibrillation, haematological disorders, and cancer-related causes. 84 CTD as a cause for this pattern is only reported and is gaining evidence in recent days.
Meningitis
Meningitis in MCTD is aseptic, and along with pulmonary artery hypertension and trigeminal neuropathy, it is considered to be one of the characteristic organ involvements used for the diagnosis of MCTD. 15 Its exact prevalence cannot be described as evidence is lacking.
Meningitis in a patient with MCTD will be mainly due to two reasons: the first one being caused by drugs used in the treatment of the MCTD itself, like steroids and NSAIDs, and the second reason is due to the direct effect of the disease. we must carefully differentiate this, as for the first reason causing meningitis, we need to stop the drug, whereas for the second, we need to start on the steroids.
CSF interferon-gamma and interleukin-6 levels will be raised in the case of drugs causing meningitis, whereas anti-U1RNP antibodies will not be elevated in such cases. In cases of the second mechanism described above, which causes MCTD disease, causing meningitis, the levels of anti-U1RNP antibodies will be raised. In this way, we will be able to differentiate the cause of meningitis in MCTD and offer a correct treatment. 85
Cerebral Venous Sinus Thrombosis
The first case of MCTD causing cerebral venous sinus thrombosis was reported by Shah PM et al. 31 This patient was started on antioedema measures along with low molecular weight heparin, and then warfarin was started. After ruling out all the other possible causes, it was found that MCTD is the condition, and prednisolone was also started, and this patient showed good improvement in one month. Another case was reported to have an association of MCTD with sinus vein thrombosis, but that case also had serology positive for APLA syndrome. 86 This highlights the fact that headache in MCTD can be due to many factors, but we must always consider sinus vein thrombosis in the differential diagnosis.
Spinal Subarachnoid Haemorrhage (SSH)
Only one case was reported to have an association between MCTD and SSH by Andreoli S et al., it was a perioperative case, and it was postulated that perioperative increased intraluminal abdominal pressure, combined with the fact that spinal arachnoid matter fragility, led to vascular rupture and resulted in SSH. This patient was then managed conservatively as the neurological signs improved rapidly and symptoms disappeared within a few days. The learning point from this case is that caution is recommended while undergoing thoracic or abdominal surgery, as it may lead to this potential complication. 23
Normal Pressure Hydrocephalus (NPH)
The relationship between CTD and NPH needs more evidence. As per present evidence, there are a few reports showing a connection between SLE and NPH. Only one case was shown to have a possible relation between NPH and MCTD. 34 This possible association was postulated because there was the presence of perivascular lymphocytic infiltration similar to that seen in probable SLE-associated NPH in the brain biopsy. At present, the standard treatment for NPH is shunting. In the future, if we are to identify a strong association between MCTD and NPH, we will be able to treat the comorbid CTD first and avoid going for the invasive shunting procedure.
Discussion
From our systematic review, we found that trigeminal neuropathy may be the presenting feature in some cases. and in cases presenting with bilateral trigeminal neuropathy, it is apt to look out for other features of MCTD to make an early diagnosis. It responds to steroids and, in some cases, HCQ, carbamazepine, gabapentin and even IVIG might be needed.42–51 Peripheral neuropathy is reported only in very few cases and can present in various forms. CIDP, mononeuritis multiplex, and sensory ganglionopathy are reported forms. It is mostly responsive to steroids, and in some cases, steroid-sparing agents may be needed.28,32,64,65 Encephalopathy can present in various forms, like dementia manifesting as cognitive decline, aphasia, and even seizures. It is treatable and responds to steroids.52,58 Neuromyelitis optica may occur secondary to MCTD and is mostly responsive to standard therapy for NMO, which includes pulse dose of steroids, followed by immunoglobulins.19,27,30
SNHL is reported in MCTD, and treatment involves steroids, and if unresponsive, cyclophosphamide may also be tried. 55 Transverse myelitis, commonly involving the thoracic spine, is also a rare manifestation of MCTD, and at present, the standard therapy, as utilised for other causes of transverse myelitis, like pulse dose of steroid in combination with cyclophosphamide, is followed. 36 PRES can present in MCTD and mistaken to be due for other causes. We suggest looking for features of MCTD if BP is not significantly elevated and there is a search for the cause. 21
Aseptic meningitis can occur in MCTD due to either the effect of the drug used for treating itself, where we need to taper the drug, or it may be due to the direct effect of the disease, which is responsive to steroids. The differentiation between these causes is established by checking CSF anti-U1RNP antibodies. 15 Cerebrovascular accidents involving both types, like ischaemic and haemorrhagic, can present in the MCTD, and treatment involves the standard therapy for stroke, along with the addition of steroids. 59
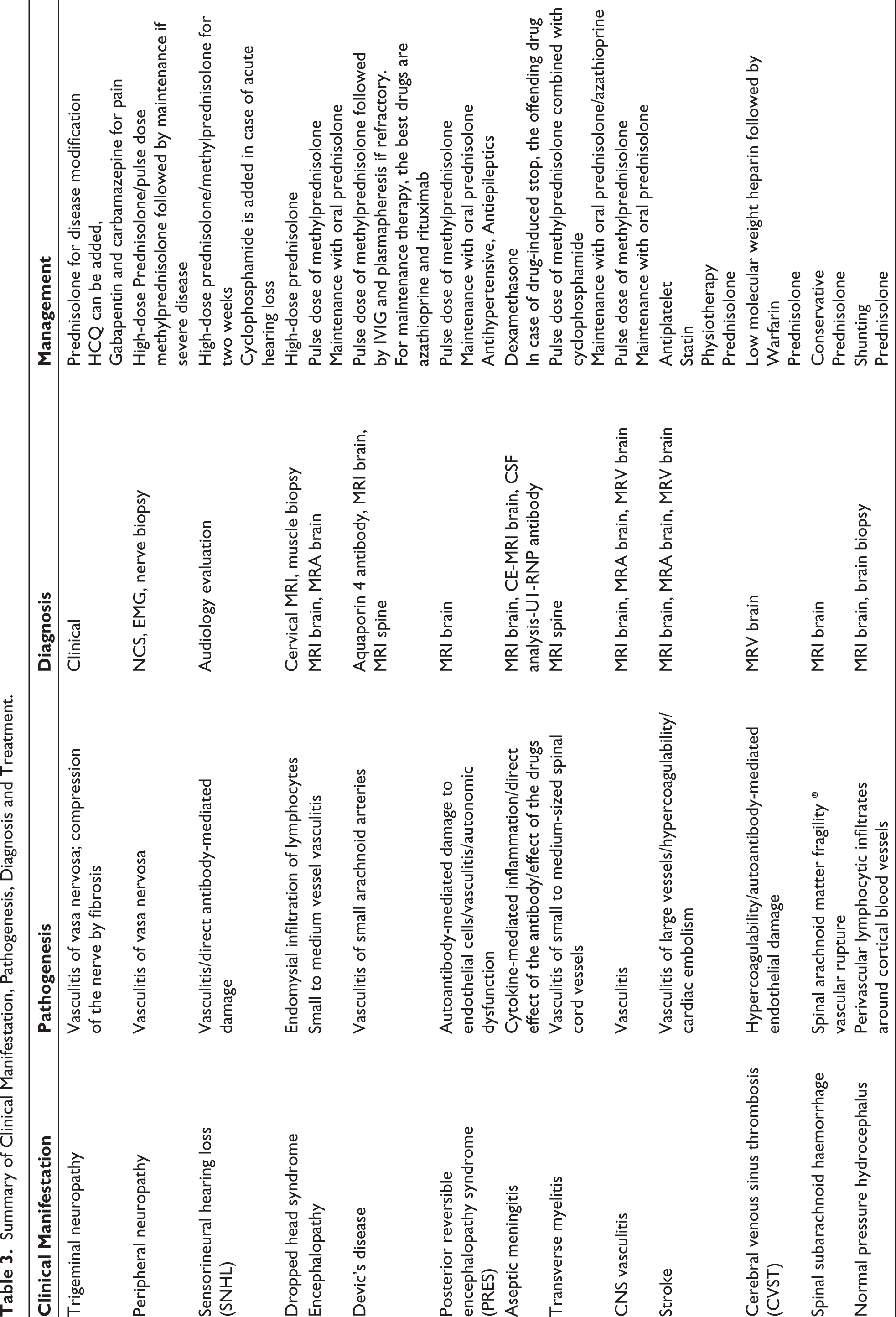
Apart from these, only one case of the following, like cerebral venous sinus thrombosis, dropped head syndrome, SSH, and NPH, is reported, and more evidence will be required to study their exact pathogenesis and link.23,31,34 The findings of our systematic review are summarised in Table 3.
The findings should be interpreted with caution, as they are largely derived from case reports and small series, subject to publication bias, and hampered by heterogeneity due to the absence of standardised diagnostic criteria, highlighting the need for larger, prospective studies with uniform protocols to better define the neurological spectrum.
Summary of Clinical Manifestation, Pathogenesis, Diagnosis and Treatment.
Conclusion
Neurological involvement in MCTD remains a clinically significant but underrecognised aspect of this rare connective tissue disorder. Evidence from case reports, case series and a small number of observational studies highlights a wide spectrum of central and peripheral nervous system manifestations, including trigeminal neuralgia, posterior reversible encephalopathy syndrome, Neuromyelitis Optica, neuropsychiatric manifestations, transverse myelitis, encephalopathy, various forms of neuropathy, dropped head syndrome, sub arachnoid haemorrhage, haemorrhagic stroke, sagittal sinus thrombosis, NPH, arachnoiditis, aseptic meningitis and psychosis. The overall quality of evidence is limited, with most data derived from single cases from case reports and series.
Although early detection of neurological symptoms in MCTD is difficult, it is essential for prompt management due to the variety of presentations and the absence of established diagnostic techniques. Future studies, in the form of multi-centre prospective cohort studies using uniform, standardised neurological assessment tools in MCTD, should involve the exploration of biomarkers such as anti-U1RNP titres and cytokines in CSF for predicting neurological involvement. Additionally, longitudinal follow-up to assess treatment response and outcomes should be carried out.
In order to enhance patient outcomes, clinicians must continue to be on the lookout for a variety of neuropsychiatric and neuromuscular symptoms in MCTD.
Supplemental Materia
Supplemental material for this article is available online.
Footnotes
Acknowledgements
I would like to thank the Department of General Medicine and the Department of Community Medicine for their constant support for this systematic review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval is not needed as it is a systematic review.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent statements are not needed, as it is a systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.