
Abstract

Dear Editor,
Diagnosis of rheumatological diseases is made by typical pattern recognition with judicious interpretation of autoantibodies. Autoantibodies are a double-edged sword. On the one hand, it helps in suspecting or confirming a diagnosis of rheumatological ailments. On the other hand, there are certain conditions, the so-called rheumatological mimics, where these autoantibodies can falsely be positive. To further complicate the scenario, the clinical presentation of many of these mimics closely resembles the presentation of rheumatological diseases. Hereby, we present one such case.
A 38-year-old lady presented with tingling dysesthesias and loss of temperature sensation over both hands and feet in a glove and stocking distribution, small joint inflammatory polyarthritis for two months and difficulty in walking for the last month. There was a history of slippage of her footwear while walking, but no history of any difficulty in getting up from a sitting position, making handgrip or doing overhead activities. She also gave the history of a reddish rash over both her cheeks. However, she denied any history of associated photosensitivity, oral ulcer or hair loss. There was no history of any fever, weight loss or systemic symptoms. General examination revealed an erythematous rash over the malar area, forehead, chin and palms, trophic ulcers over both feet, healed burn marks over hands and gross wasting of the small muscles of hands and feet (Figure 1A-C). The skin lesions had normal sensation. There was tenderness noted over the bilateral wrist and metacarpophalangeal joints without any joint swelling. Neurological examination revealed a distal predominant weakness affecting both upper and lower limbs, absent supinator and ankle reflexes with other deep tendon reflexes being diminished, loss of all sensory modalities distally below the elbows and knees and bilateral thickened ulnar nerves. The rest of the systemic examination findings were normal.
(A) Erythematous Rash Over the Forehead, Malar Area and Chin. (B) Erythematous Rash Over Palms with Wasting of Small Muscles of the Hand and Healed Burn Mark Over the Right Palm. (C) Trophic Ulcer Over the Heel and Ball of the Great Toe. (D) Slit-skin Smear (Z.N. Stained) Showing Acid-fast Bacilli.
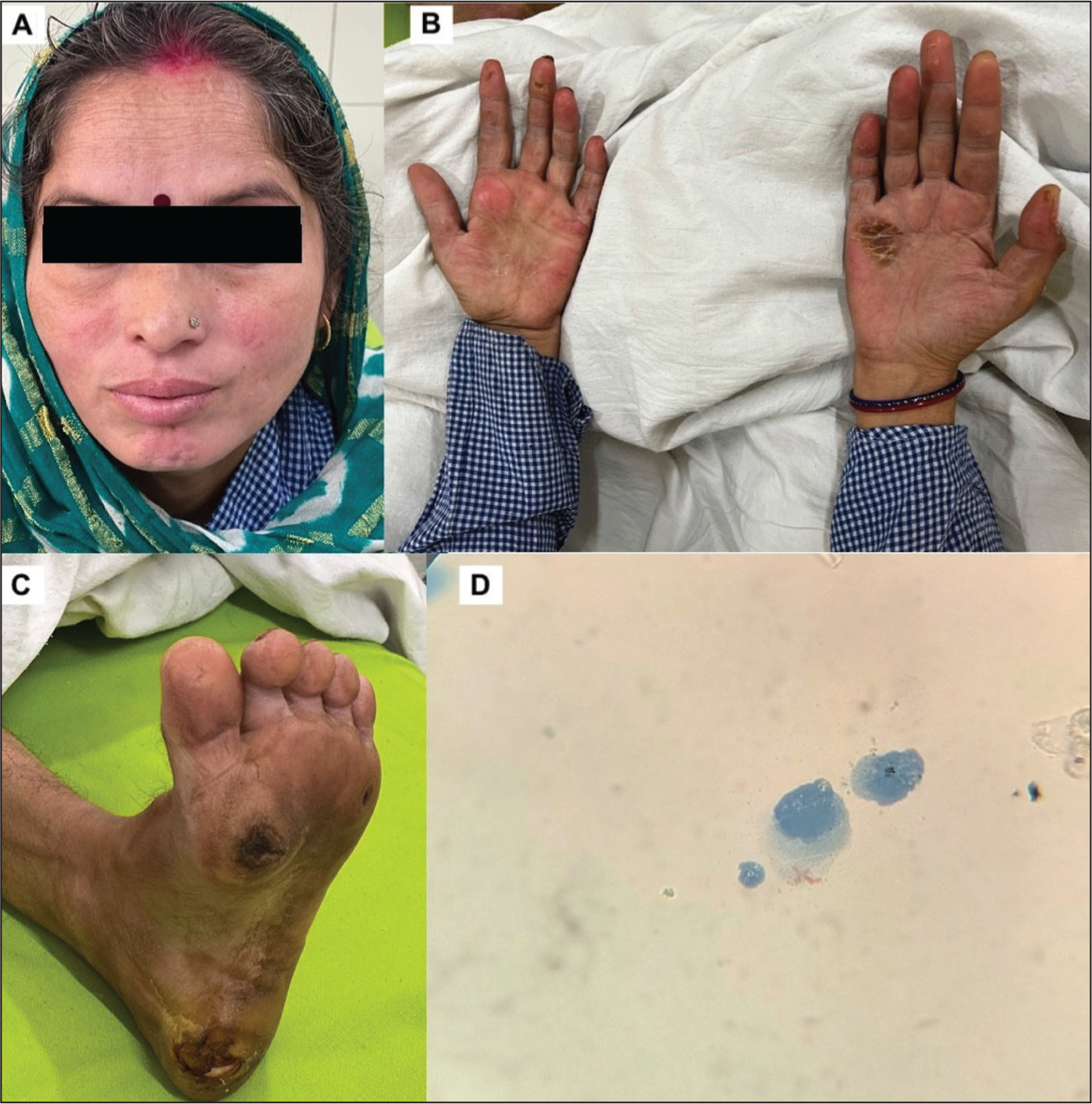
With a history of skin rash and arthritis, the possibility of a connective tissue disease (CTD) such as systemic lupus erythematosus (SLE) was primarily considered. The neurological findings indicating neuropathy were considered due to suspected CTD. Also, with a background of thermoanesthesia and thickened ulnar nerves, leprosy was kept as another possibility. Investigations revealed high ESR (42 mm/1st hour) with normal CRP and other haematological and biochemical parameters. All immunological investigations (ANA, ANCA, RF and anti-CCP) turned out to be normal. A nerve conduction study revealed a sensory-motor axonal polyneuropathy of bilateral upper and lower limb nerves. Given the negative immunological work-up, a slit-skin smear was done from the right ear lobule, which showed the presence of acid-fast bacilli with a bacteriological index of 2+ (Figure 1D), thus confirming a diagnosis of multibacillary leprosy. Although there were erythematous skin lesions, none of those were classical hypoaesthetic or anaesthetic. However, considering the presence of thickened nerve and BI of 2+, lepromatous leprosy was the most likely probability as per the Ridley-Jopling classification. She was started on multibacillary multidrug therapy. Prednisolone 40 mg once daily was also started for neuritis with a plan for gradual tapering over the next 12 months. Protective footwear and lifestyle modifications were also advised to prevent further damage accrual secondary to neuropathy.
Leprosy can be a great mimic for various rheumatological diseases. The most common rheumatological manifestation of leprosy is polyarthritis, with almost 1%–5% of patients having a presentation mimicking rheumatoid arthritis. 1 Other well-known musculoskeletal manifestations include tenosynovitis, enthesitis or Charcot arthropathy in varying frequency. 2 Cutaneous manifestations include cutaneous ulcers, erythematous macules or plaques, Raynaud’s phenomenon and hypo or hyperpigmented patches mimicking a range of rheumatic diseases such as scleroderma, vasculitis, sarcoidosis or SLE. 1 Positivity for various immunological markers such as ANA, RF, antiphospholipid antibodies and HLA-B27 has also been reported, thus making the diagnosis more challenging in such cases.3,4 Amongst various autoantibodies, ANA positivity has been reported in 3%-34% of cases, usually in a low titer and the commonest pattern observed was speckled and homogenous. 5 Multibacillary leprosy, a previous history of multiple lepra reactions, older age and longer duration of illness are some of the factors associated with a greater chance of positive ANA. Thus, an erythematous cutaneous rash in a background of neuropathy and positive ANA may lead to an erroneous diagnosis of SLE. Rather than too much reliance on a single clinical finding, careful consideration of all the clinical and laboratory findings can help in such diagnostic dilemmas.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the patient.