
Abstract
Background
Chronic joint pain with movement restriction in a child often has a multitude of aetiologies. The most frequent cause is Juvenile Idiopathic arthritis. Post Viral arthralgia, Complex regional pain syndrome, Fibromyalgia, reactive arthritis, vasculitis, and autoimmune disorders are amongst other causes. 1 In a child, due to varying clinical presentation of joint deformity and pain, a thorough clinical evaluation and work-up is required to arrive at a diagnosis amongst the possible vast differential diagnoses. 2
In this article, we present a case of a child with a 2-month history of bilateral knee pain and contracture. The unique clinical profile of the child led to a diagnostic enigma. The requirement of a multidisciplinary approach in recognising the importance of each symptom and its correlation with the available list of diagnoses is highlighted.
Case Presentation
The case presentation is chronologically described to understand the step-wise approach and the way in which the diagnostic difficulties were addressed.
History
At first presentation to our Orthopaedic clinic—An early adolescent girl (age 14 years) with a two-month history of bilateral progressive knee deformity with gradually increasing knee and thigh pain (Visual Analogue Scale 9). Pain was referred to both hips. There was an associated limp. Over the course of two months, she started walking with support.
History of on and off abdominal pain and loss of appetite for 7 days prior to hospital visit, with evening temperatures, history of left forearm injury 4 months back (No documentation).
History was negative for multiple joint involvement, morning stiffness, trauma/Injury, fever/rashes, back pain/weakness, paraesthesia/stiffness of joints and similar complaints in the past. There was no significant family history.
Clinical Examination
The child was conscious and alert. She was moderately nourished. General Physical examination was unremarkable.
Local examination
B/L Upper limbs were normal. Gait: Supported crouching gait. Exaggerated lumbar lordosis and Thomas’ test confirmed fixed flexion deformity (FFD) of 15° in both hips. There was bilateral knee contracture of 30° with further flexion range up to 100°. Bony and joint tenderness of both hips, knee and distal thigh. Wasting of the bilateral quadriceps and calf was noted. Diffuse lumbar spine tenderness was present. Both knees were tender on palpation. There was no effusion. Allodynia was present. There was no local temperature rise/any scars/sinuses/signs of previous injury/surgery/rashes. Extremities were normal in texture and temperature. Neurological examination was normal except around the hip and knee, which the child was unable to do due to pain. Ankle and foot were normal.
Systemic examination
Chest was clear. Diffuse lower abdominal tenderness was noted.
Clinical diagnosis: Probable Inflammatory Arthritis causing bilateral knee pain and flexion attitude. The term inflammatory arthritis was used based on the clinical signs pending laboratory evaluation for an organic aetiology.
Differential Diagnosis
The symptoms and clinical findings were highly discordant. The following possibilities in the order of suspicion were considered.
Juvenile Idiopathic Arthritis/associated connective tissue disease—possibly oligoarticular variant. It was ruled out due to the absence of small joint involvement, morning stiffness, negative screening of Rheumatoid factor and Anti-CCP, HLA B27, ANA and absence of arthritis on ultrasonography and MRI.
Complex Regional Pain Syndrome: The clinical presentation of CRPS varies in every individual. CRPS involves the distal extremities and is more often seen in the upper limb, and hence, the index of suspicion was low. 3
Fibromyalgia: Usually presents with diffuse pain all over the body. However, localised pain can be seen. The index of suspicion was low due to non-specific complaints and not fulfilling the guidelines outlined in the Royal College of Physicians document for diagnosis of Fibromyalgia. 4
Pain amplification syndrome: Episodes of emotional stress and physical pain were correlated late in this case when the child was found to be less interactive. The index of suspicion was high.
Bilateral Psoas abscess (Tubercular): Presence of abdominal pain, psoas tenderness and bilateral hip and knee deformity pointed to a possible psoas abscess, which is common in the Indian subcontinent. It was ruled out by a negative ultrasonography and MRI spine.
Muscular dystrophy: Proximal muscle involvement of the bilateral lower limb in this case prompted the workup. It was ruled out by a normal nerve conduction study, and deformities were corrected with traction.
Investigations
Work-up
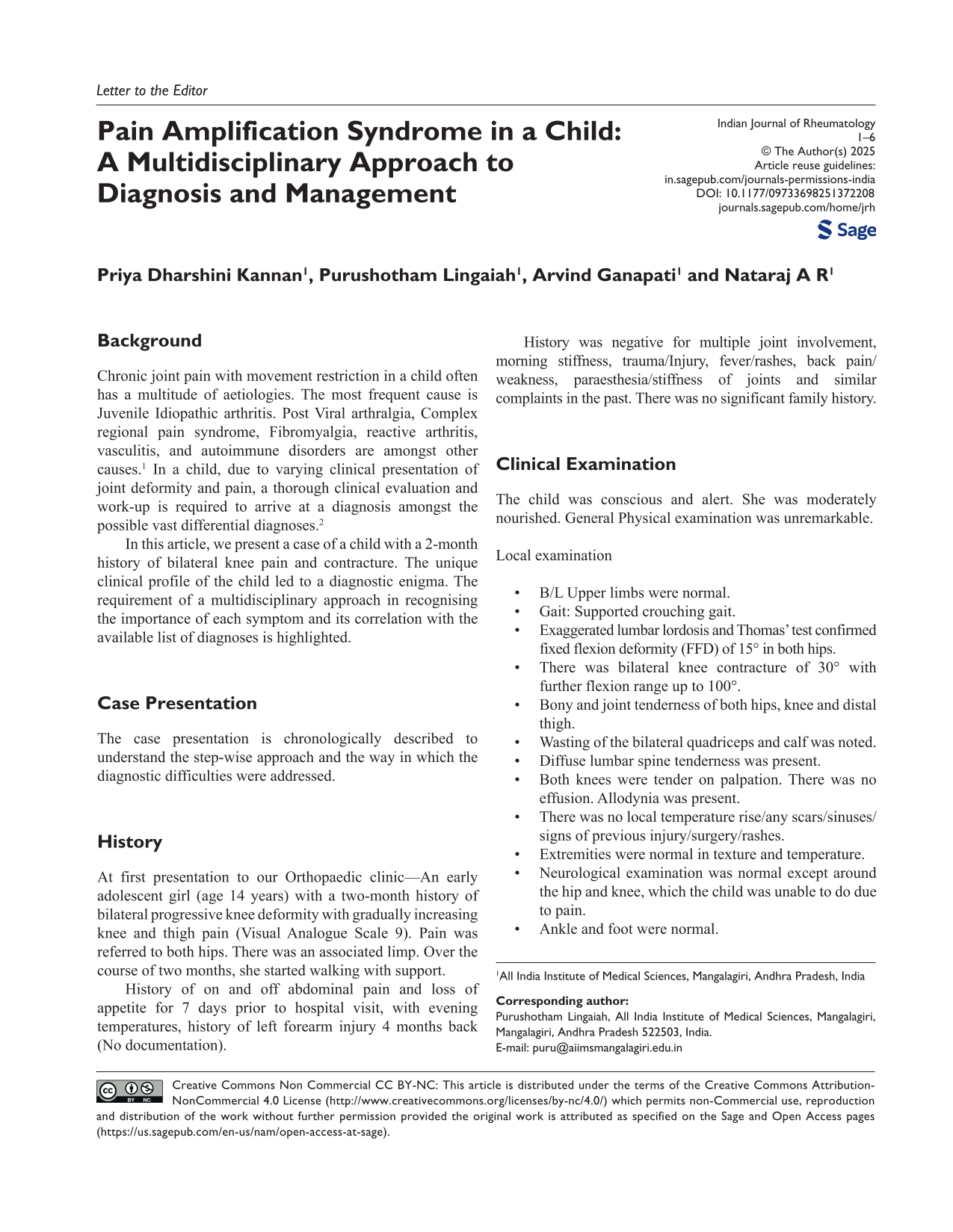
Based on the differential diagnosis, we proceeded with a multidisciplinary approach. The reason for interdepartmental referral, their opinion, work-up and review have been tabulated (Table 1).
Interdepartmental Referral and Work-Up.
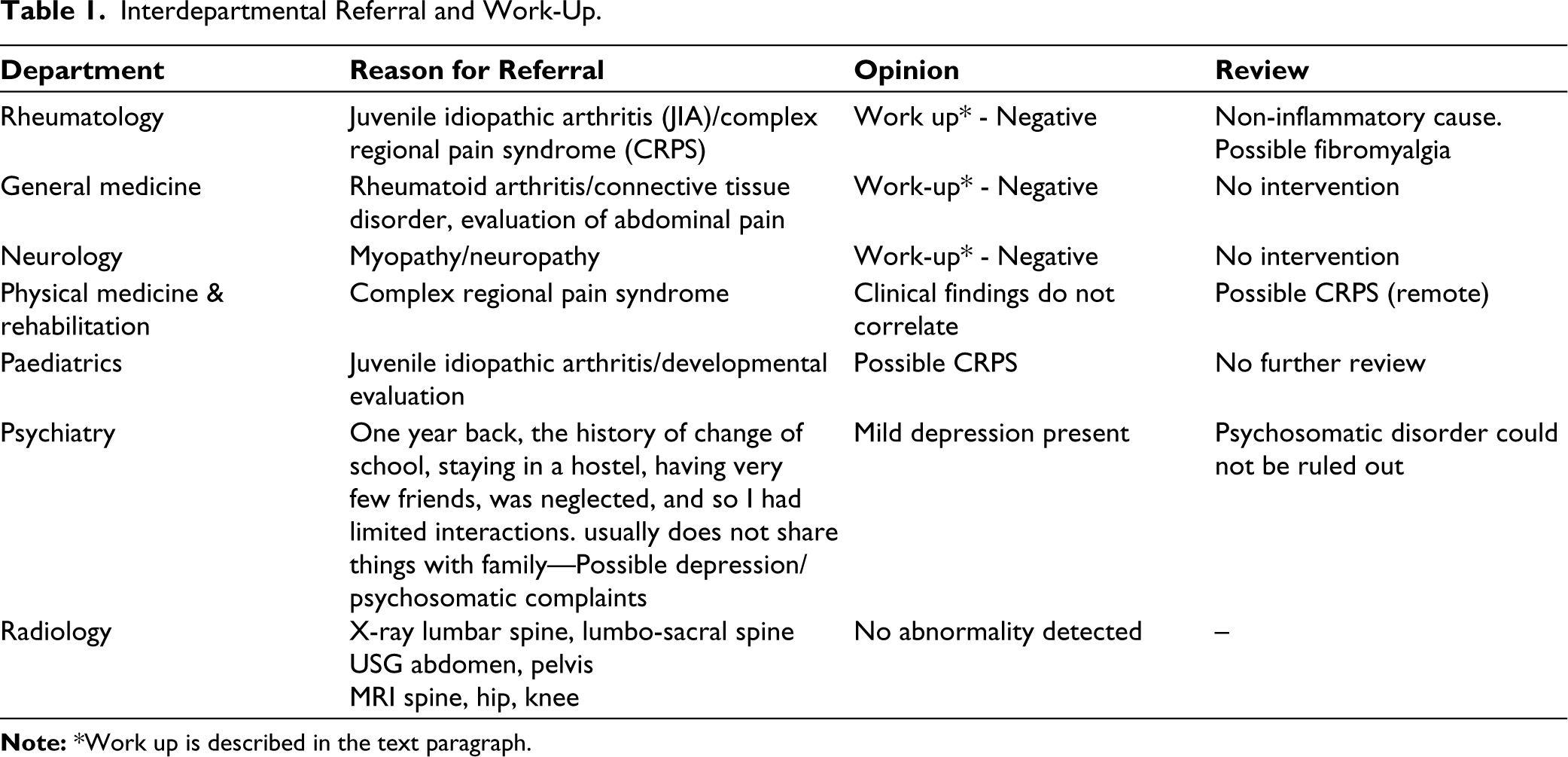
Laboratory and radiological investigations were raised as per the work-up advice of various medical disciplines and reviewed. Complete blood picture, Erythrocyte sedimentation rate, c-reactive protein, Liver and renal function tests, complete urine examination, Viral antibody markers, Rheumatoid factor, Anti cyclic citrullinated peptide, HLA-B27, Metabolic tests, Thyroid profile, Anti-nuclear antibody profile, Creatine phosphokinase, Anti double strand DNA, serum amylase, lipase levels, radiographs of hip, knee and spine, Ultrasonography of abdomen, Computed tomography of chest, Magnetic resonance imaging (MRI) of spine and hip, Electromyography of Lower limb muscles and Nerve conduction studies. None of the tests revealed any significant findings (Table 2). The clinical presentation in the absence of any supportive Neurological, Rheumatological and Orthopaedic aetiology makes functional cause very probable.
Laboratory Results.
Final Diagnosis
Initial suspicion of inflammatory arthritis was revised due to the absence of supportive laboratory and imaging findings. A thorough multidisciplinary approach to diagnosis and treatment led to the possibility of underlying stress causing somatic symptoms. The Working diagnosis of Pain amplification syndrome was arrived at after a positive response to physical therapy and rehabilitation, traction and cast application, pharmacological therapy and psychological counselling.
Treatment
Course in the Hospital
During her stay in the hospital, a lack of interaction and response to communication was observed. The child was then evaluated by a psychiatrist when the diagnosis of mild depression was made. Counselling sessions were started for the same.
Bilateral below-knee skin traction was applied for the correction of knee and hip deformity.
After the review from multiple medical specialities, the treatment protocol supported by literature was followed. Non-steroidal anti-inflammatory drugs and a trial of glucocorticoids were given in the initial phase of hospitalisation. No response to these drugs helped in ruling out an inflammatory aetiology.
Vitamin D3 and Vitamin B12 were nutrient supplements.
Anti-convulsant (Pregabalin) trial was given to look for a response in terms of CRPS. Although the initial phase response was low, the addition of psychological counselling drastically improved the health condition. This was continued even after the diagnosis of Pain amplification syndrome was made.
A tricyclic antidepressant was started late in the course of evaluation for Pain amplification syndrome and stress-induced symptoms.
Physical therapy and rehabilitation played a vital role in shaping the overall comprehensive treatment. The contractures eventually were corrected.
Outcome and Follow-up
The child showed dramatic improvement over the course of 1 month of treatment. The deformities were corrected with occasional pain (Visual analogue scale 2) in the distal thigh. She was able to walk unassisted with a normal gait. At 6 months follow-up, there was no recurrence of symptoms. The child had returned to school and developed fair social interaction. The quality of life had significantly improved.
Discussion
The presence of physical and psychological symptoms in a child poses a challenge for diagnosis and treatment. The non-specific symptoms with non-correlating clinical signs, laboratory results and radiological findings add to this menace. The spectrum of diseases considered as possible diagnoses in our case included JIA, Pain amplification syndromes such as CRPS, Fibromyalgia or Amplified musculoskeletal pain syndrome (AMPS), Muscular dystrophy and proximal myopathy. Although there are distinctive features in each of these conditions with a well-established diagnostic criterion, the diagnosis remained obscured in our case due to mixed presentations without supportive work-up findings. One common entity is the presence of mental stress, which either is a cause or a result of these clinical conditions. 5 The presence of mental stress and social fear detected in our case played a vital role in management and improving the quality of life of the child.
The understanding of the basis of pain in these subgroups of patients requires a holistic approach, and the biopsychosocial model of pain explains the interplay of various components involved in the pain process. It proposes that pain is not solely a biological experience, but rather a complex interplay of biological, psychological, and social factors. This model emphasises that these factors interact dynamically and influence an individual’s pain experience. 6 The biological factors include the physical aspects of pain, such as tissue damage, nerve function, and the body’s response to injury. The psychological factors encompass thoughts, feelings, and behaviours related to pain. The social factors relate to the social and cultural context in which pain is experienced. A Holistic approach encourages a comprehensive view of pain, considering all contributing factors. Recognising the unique interaction of these factors in each individual allows for tailored treatment plans. Psychological and social interventions highlight the importance of addressing psychological distress and social factors in pain management. The biopsychosocial model is widely adopted in pain research and treatment, shifting the focus from purely biomechanical explanations of pain to a more holistic and integrated approach.
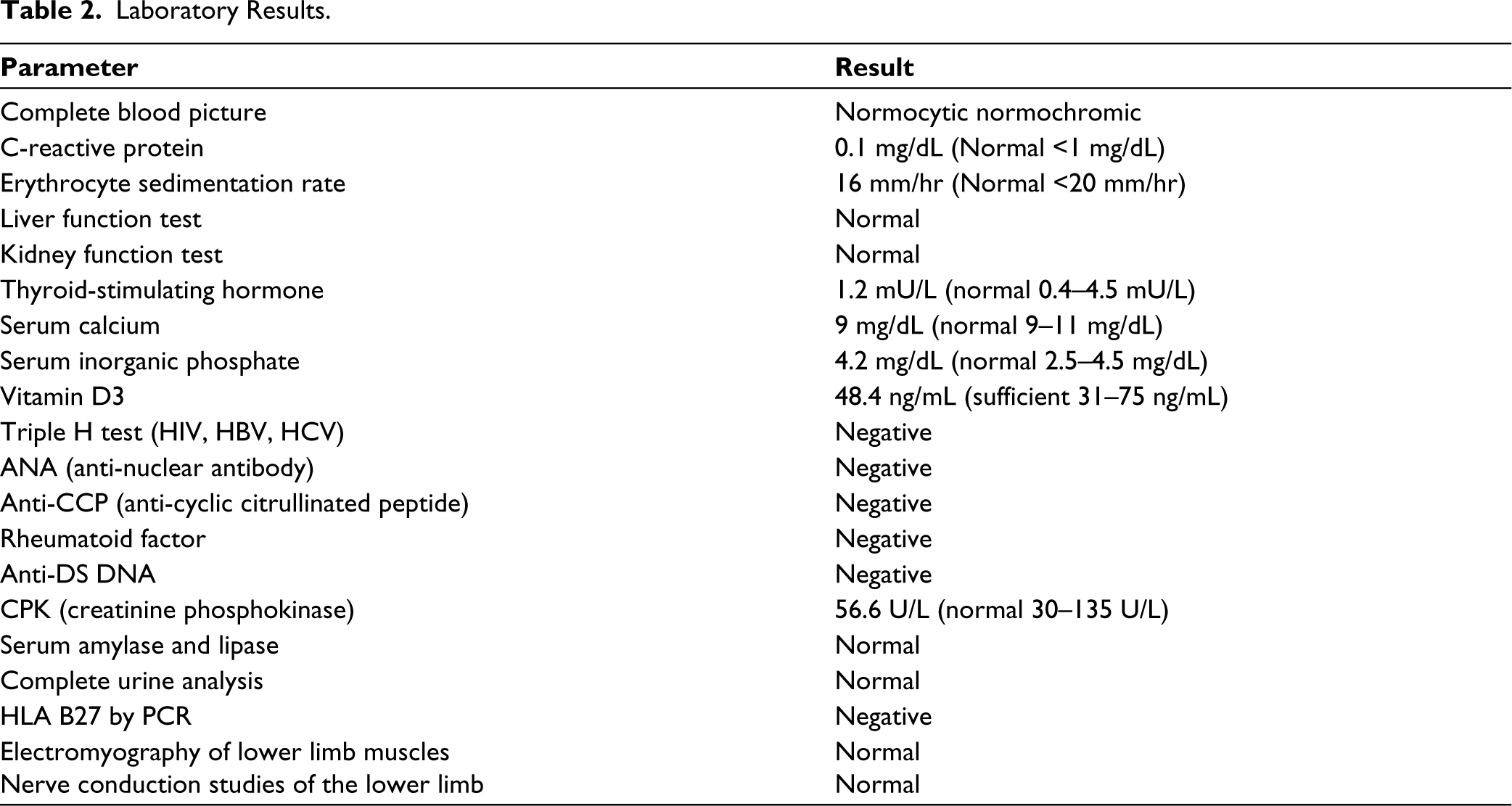
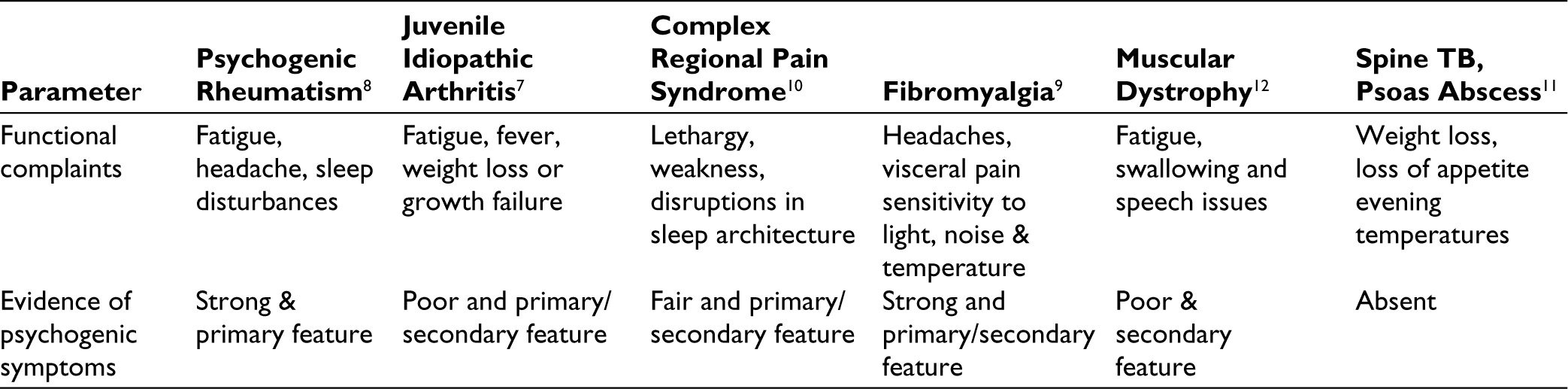
Considerable overlap in the presentation of these disease conditions makes the diagnosis difficult. Various International associations and bodies have formulated diagnostic criteria which may guide the identification of symptoms attributable to a particular disease. The differentiating features presented in the table are just an overview and not absolute features.6–12 Varying presentations may be encountered in patients. However, a thorough knowledge will guide the physicians for early detection of symptom complex and pursue a multidisciplinary approach for treatment (Table 3). The clinical presentation in our case pointed towards the diagnosis of Pain amplification syndrome spectrum, supported by diagnostic criteria more in favour of CRPS, followed by AMPS.
Differentiating Features of Diagnoses.
Learning points/take-home messages: Three to five bullet points
The diagnosis of Pain amplification syndrome requires a team approach. The term Pain amplification syndrome should be borne in mind when the non-specific physical ailments are accompanied by inherent mental stress and social suffering. A multidisciplinary treatment should be initiated at the earliest to reduce the symptoms and improve the quality of life in these cases. Physical, psychosocial and pharmacological treatment works in tandem to provide a positive response.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Written informed consent was obtained from the parent of the child. Ethical approval was obtained from the Institutional Review Board.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent has been taken from the patient to use clinical photographs, data for the purpose of research and publication.