
Abstract
Background:
Comorbidities in rheumatoid arthritis (RA) patients vary significantly, with prevalence ranging from 3% to 60%. However, limited data exist from India. This study aims to evaluate the prevalence of comorbidities in RA patients in Indian clinical settings.
Methods:
The multicentre, observational study was conducted across eight centres in India using data from the Indian Rheumatology Association database. Comorbidities were classified using the International Classification of Diseases, Tenth revision (ICD-10) Charlson Comorbidity Index. Data were categorised by comorbidity, age and region and analysed using descriptive statistics, Fisher’s exact test, chi-squared test, t-test, analysis of variance (ANOVA) and logistic regression.
Results:
The study included 4,655 RA patients who met the European League Against Rheumatism (EULAR) classification criteria, with a mean age of 52.42 ± 12.18 years. Comorbidities were present in 41.72% of the patients. Those with comorbidities were older (56.16 vs. 49.74 years) and had a longer duration of RA (122.34 vs. 107.67 months). Out of 1,942 patients with comorbidities, 90% were female and 72% were from Southern India. The major comorbidities included hypertension (21.87%), thyroid disorders (14.5%) and diabetes (11.99%). Patients over 50 years had higher prevalence of diabetes, hypertension and cardiac diseases, while younger patients had more migraines and thyroid disorders.
Conclusion:
RA patients in India have a significantly higher burden of comorbidities, with hypertension, thyroid disorders and diabetes being the most common. Older age and a greater proportion of patients residing in Southern India were associated with increased comorbidities, suggesting potential regional differences in risk factors, healthcare access or lifestyle. These findings highlight the need for region- and age-specific management strategies.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disorder that primarily affects the joints, leading to disability and reduced life expectancy. Globally, it impacts an estimated 17.6 million individuals, with a prevalence of about 0.75% in India.1,2 The prevalence of comorbidities in RA patients varies significantly, with reports suggesting a range from 3% to 60%, and some studies estimating that up to 80% of RA patients may experience additional health conditions.3,4
Comorbidities in RA are closely linked to factors such as chronic inflammation, medication use and other disease-related risks all of which contribute to increased mortality.5,6 In a cross-sectional study by Singh et al., 60 comorbidities were identified in RA patients, with anaemia being the most prevalent, followed by infections, thyroid disease, renal disease, osteoporosis, cardiovascular disease, lung disease and vasculitis. 7 Identification of comorbidities plays a crucial role in guiding personalised treatment for RA, as they can influence the choice of therapies and affect treatment response. Understanding their prevalence and patterns is vital for optimising management, predicting outcomes and improving patient care. Comorbid conditions not only impact disease activity and treatment effectiveness but also contribute to functional impairment and reduced quality of life. A comprehensive approach addressing both RA and its associated comorbidities is essential for better long-term outcomes. 8
In India, research on comorbidities in RA is limited, with most studies focusing on specific regions. This study aims to explore comorbidity patterns across the country using data from the Indian Rheumatology Association (IRA) database, capturing both clinical and demographic features. By examining the relationships between comorbidities and disease characteristics, this study aims to provide valuable insights to help clinicians with risk stratification, comprehensive care and informed decisions on treatment and patient monitoring in RA management.
Materials and Methods
Registry/Database Design and Study Population
The independent, cross-sectional, multicentre observational study was conducted across eight centres in India, selected based on their geographic location. The IRA database, established in April 2020, was designed to collect data on patients with six autoimmune rheumatic diseases (AIRDs): RA, spondyloarthropathy (SpA), psoriatic arthritis (PsA), systemic lupus erythematosus (SLE), scleroderma and primary Sjögren’s syndrome (pSS). The primary focus of this study was to gather data on comorbidities in both newly diagnosed and follow-up patients over 18 years old who met the 2010 American College of Rheumatology/European League Against Rheumatism (EULAR) classification criteria for RA. 9 The last patient of the dataset recruited was in June 2022. Data collection was conducted using two structured forms: one for general patient information and another for disease-specific details, both validated by experts. Clinical research associates (CRAs) completed the forms based on patient interview and their medical charts. To ensure consistency, both the principal investigators (PIs) and CRAs from all centres participated in online training sessions. The PI at the central centre addressed any queries related to data collection. All participating centres obtained approval from their institutional ethics committees and written informed consent was secured from all patients (other ethics committee details are provided in the supplementary file).
Sample Size Calculation for Registry
For the entire registry, the minimum number of subjects with AIRDs needed for comparison was calculated, with the primary objective of evaluating the clinical and laboratory profiles of the six AIRDs under consideration. The estimated number of patients to be recruited for the analysis of AIRDS was 6,500. 10 The sample size for each disease was estimated based on the prevalence of each autoimmune disease, with a proportionate sample considered for each disease. For RA, which has an estimated prevalence of 0.6% to 1.2%, approximately 2,000 patients were considered the minimum target.
Data Collection and Definition
The data on comorbidities were collected as per the definitions in the new International Classification of Diseases (ICD)-10 version of the Charlson Comorbidity Index. 11 Information was collected from patients interviews and medical charts. The comorbidities assessed included cardiovascular conditions such as myocardial infarction, congestive heart failure, congenital heart disease (CHD), rheumatic heart disease and peripheral vascular disease. Neurological conditions included migraine, cerebrovascular events (including stroke and transient ischaemic attack), hemiplegia, dementia, Parkinson’s disease or other degenerative neurological disorders. Respiratory conditions comprised chronic pulmonary disease, bronchial asthma and allergic diathesis (including asthma). Rheumatologic and musculoskeletal conditions included rheumatologic diseases, psoriasis, osteoporosis, fibromyalgia and osteoarthritis. Gastrointestinal conditions encompassed peptic ulcer disease, recurrent diarrhoea of unknown cause, inflammatory bowel disease (IBD), mild liver disease and moderate or severe liver disease. Metabolic and endocrine conditions included hyperlipidaemia, diabetes (with and without chronic complications) and thyroid disorders (hypothyroidism or hyperthyroidism). Renal conditions included moderate-to-severe renal disease. Oncological conditions comprised cancer without metastases, leukaemia, lymphoma and metastatic solid tumours. Infectious conditions included tuberculosis, hepatitis B and C and acquired immunodeficiency syndrome (AIDS) or human immunodeficiency virus (HIV) infection. Psychiatric conditions included neurosis and depression. Other conditions identified by the PI were also considered. Comorbidities were defined according to ICD codes, and trained experts at each site proactively assessed their presence. Anaemia due to chronic disease (AOCD) or iron deficiency was not classified as a comorbidity in this study. Confirmation of comorbid conditions was based on prior evaluations from the patients’ previous visits or from their treating physicians. 12
Statistical Analysis
For the analysis, patients were categorised into two groups: those with comorbidities and those without. To calculate age-wise incidence, patients were further divided into two age categories: >50 and ≤50 years. Descriptive statistics, with categorical variables represented as counts and percentages, and continuous variables as mean ± standard deviation (SD), Fisher’s exact test and chi-squared test were used for categorical comparisons, while the two-tailed t-test and analysis of variance (ANOVA) were employed for continuous variables.
Logistic regression analysis was performed for common and significant comorbidities. It was conducted with cardiac diseases, migraine, neurological diseases, rheumatological diseases, hyperlipidaemia, diabetes, infection hypertension and hypothyroidism as the dependent variables, based on their higher prevalence (>1%). Age, gender and duration of illness were included as covariates, considering their potential influence on the development of comorbidities.
The regression output included coefficient estimates (B), Wald statistics and P values to assess the statistical significance of each predictor. Odds ratios (OR, Exp[B]) with 95% confidence intervals (CIs) were calculated to quantify the effect of each predictor on the likelihood of comorbidities. A P value <.05 was considered statistically significant.
Multicollinearity was assessed prior to logistic regression analysis to ensure that independent variables were not highly correlated. Tolerance and variance inflation factor (VIF) values were examined, with variables having VIF values >10 or tolerance values <0.1 excluded from the final model.
The analysis also included classification plots, Hosmer–Lemeshow goodness-of-fit tests, case-wise residuals, correlation of estimates, iteration history and 95% CIs for Exp(B). Outliers beyond 2 SDs were identified in the residuals. The model incorporated a constant, with stepwise entry and removal probabilities set at 0.05 and 0.10, respectively, a classification cutoff of 0.5 and a maximum of 20 iterations.
Results
The study included 4,655 patients who met the EULAR classification criteria for RA. The mean age was 52.42 ± 12.18 years (range: 16–97), with 87.5% being females. The average duration of RA was 113.8 ± 83.52 months (range: 1–600).
Overall, 41.72% of patients had one or more comorbidities. Patients with comorbidities were significantly older, with a mean age of 56.16 ± 11.04 years (range: 18–97), compared to 49.74 ± 12.26 years (range: 16–96) in those without comorbidities (P < .001). The duration of RA was also longer in the comorbidity group, at 122.34 ± 87.01 months (range: 1–600), versus 107.67 ± 80.38 months (range: 1–588) in those without comorbidities (P < .001). Females had more comorbidities than males (89.8% vs. 10.2%, P < .001). Geographically, the Southern region of India had the highest proportion of patients with comorbidities (71.99%) compared to other regions (P < .001) (Supplementary Table 1).
Distribution of Comorbidities Among the RA Patients.

The most prevalent comorbidities were hypertension (21.87%), thyroid disorders (14.5%) and diabetes (11.99%), followed by cardiac diseases (0.71%). Among cardiac diseases, CHD and prior myocardial infarction were the most common, each affecting 0.17% of the cohort. Hyperlipidaemia was noted in 1.27%, and overlap rheumatologic diseases in 1.93%, with osteoarthritis being the most frequently observed (Table 1). Dementia was reported in 0.54% of patients. Less common conditions, such as anaemia, thrombosis (unknown antiphospholipid syndrome status), congenital insensitivity to pain with anhidrosis, chronic obstructive pulmonary disease (COPD) and various skin conditions, were observed in 0.02% or fewer patients. Of the total, 1,377 patients (29.6%) had one comorbidity, 469 (10.1%) had two, 89 (1.9%) had three and 7 (0.2%) had four comorbidities.
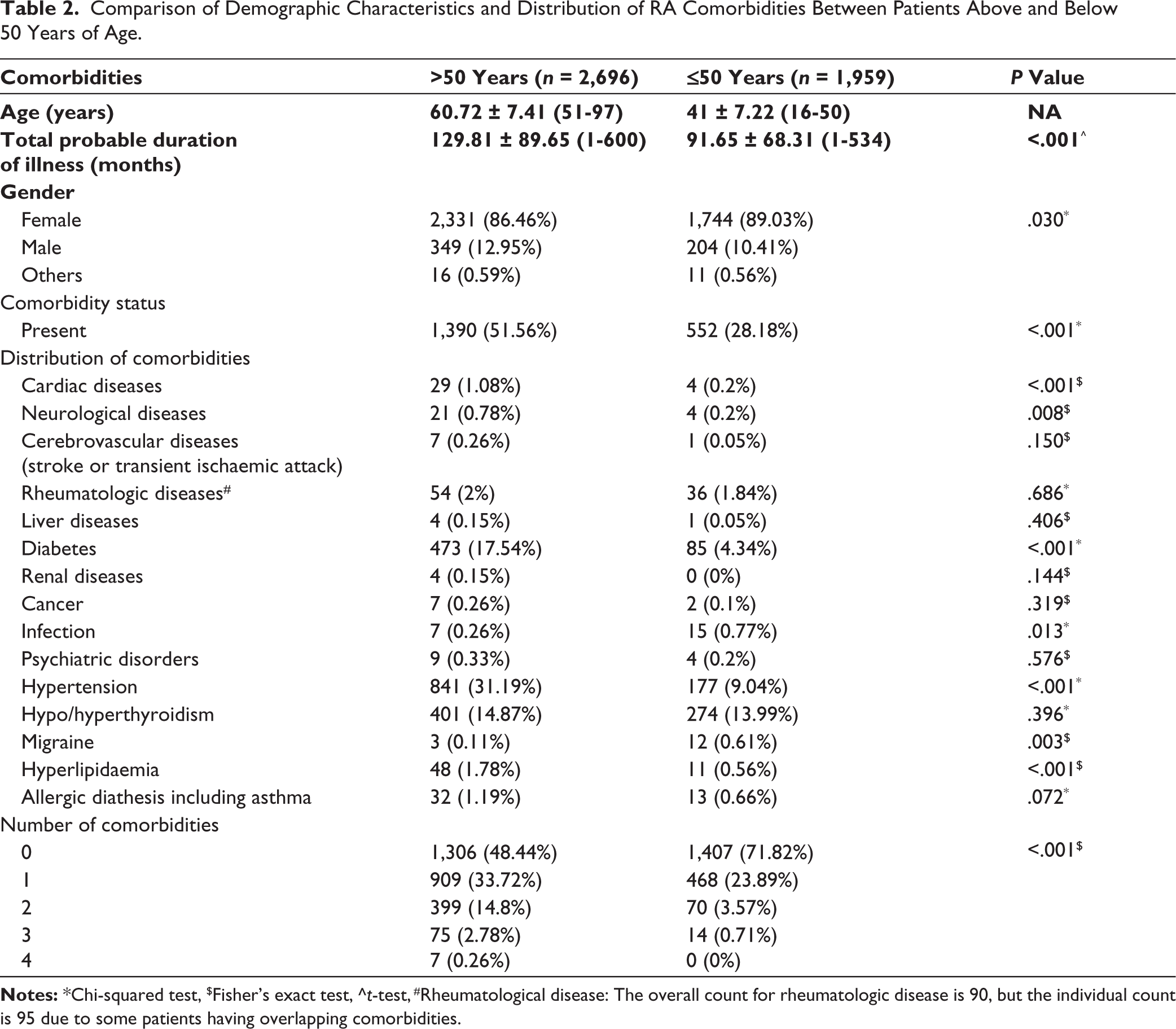
Comparison of Comorbidities Between RA Patients Above and Below 50 Years of Age
The older group (>50 years) had significantly longer duration of RA (129.81 ± 89.65 months) compared to the younger group (P < .001). Females predominated in both age groups, with a slightly higher percentage in the younger group (89.03% vs. 86.46%, P = .030).
Comorbidities were more prevalent in group >50 years with 52% having with one comorbidity, compared to younger (P < .001). Cardiac disease (1.08%) and neurological diseases were more common in >50 years group (0.78%, P = .008), whereas migraines in the ≤50 group (0.61%, P = .003). Dementia was more in older patients (0.74% vs. 0.2%, P = .012), and stroke or transient ischaemic attacks in the >50 age group (0.22%, P = .043) (Supplementary Table 2). Diabetes was more prevalent in the older group (17.54%) compared to the younger group (P < .001), as were hyperlipidaemia (1.78% vs. 0.56%, P < .001) and hypertension (31.19% vs. 9.04%, P < .001). Older patients (>50 years) were more likely to have multiple comorbidities. The prevalence of having three or more comorbidities was significantly higher in older patients (P < .001, Table 2). The details of comorbidities that are not significant have been provided in Supplementary Table 2.
Comparison of Demographic Characteristics and Distribution of RA Comorbidities Between Patients Above and Below 50 Years of Age.
Region-wise Comparison of RA Patients with Comorbidities
The mean age of the population was lower in the northern and eastern regions of India compared to the southern and western regions (P < .001). The mean age of patients from the southern region was 53.97 ± 11.92 years (range: 18–97 years), and the duration of RA was 116.13 ± 83.34 months (range: 1–600 months). These values were comparable to those from the western region, where the mean age was 51.24 ± 12.27 years (range: 18–87 years) and the duration of RA was 115.33 ± 87.15 months (range: 2–588 months). Conversely, the eastern region had the shortest RA duration (77.50 months, P < .001) and a younger age profile. The female-to-male ratio was consistent across regions, except in the eastern region (female-to-male ratio 18.5:1).
Comorbidities were highest in the eastern region (46.41%), despite its younger population, and lowest in the western region (35.78%, P < .001). Neurological diseases were more prevalent in the south (0.74%, P = .041), while rheumatologic diseases were more common in the north (6.13%, P < .001). Diabetes prevalence was highest in the south (14.1%) and east (10.53%, P < .001), with the east experiencing more chronic complications (5.74%, P = .026).
Infections were most prevalent in the east (3.83%), whereas cancer was more common in the west (0.57%), including cancer without metastases (0.57%, P = .009). Depression was more frequent in the west (0.86%, P = .010). The prevalence of hypertension was highest in the west (23.13%) and south (23.08%, P < .001). The east had the highest prevalence of hyperlipidaemia (1.58%) and thyroid disorders (23.92%, P < .001, Table 3).
Descriptive Analysis of Comorbidities by Geographic Region.


Findings of Logistic Regression Analysis
Logistic regression analysis revealed that comorbidities such as cardiac diseases (P < .001), neurological diseases (P = .001), hyperlipidaemia (P < .001), diabetes (P < .001) and hypertension (P < .001) significantly increased with age, whereas migraines were more common among younger patients (P = .005). Gender significantly influenced the likelihood of developing hyperlipidaemia (P = .043), thyroid disorders (P < .001) and hypertension (P = .003). The duration of RA illness was significantly associated with hyperlipidaemia (P = .014) and hypertension (P = .004), but did not affect other comorbid conditions (Table 4). Detailed results are provided in Supplementary Table 3.
Results of Logistic Regression Analysis of Comorbidities.

Discussion
This study found that 42% of RA patients had at least one comorbid condition, with comorbidities being more prevalent in those over 50 years of age and showing a significant female predominance. Common comorbidities included hypertension, thyroid disorders, diabetes, hyperlipidaemia, cardiac diseases, rheumatoid diseases and neurological disorders. This aligns with a pilot study from northeast India, which also reported a higher frequency of comorbidities in female RA patients. 7 A study from western India similarly found comorbidities in about 34% of RA patients, with a greater prevalence in females (65.53% vs. 34.47%). 13 These findings are consistent with global studies, which indicate that 40% to 67% of RA patients experience comorbid conditions, often presenting with one or more comorbidities at RA onset.14–16
Comorbidities were notably more common in patients aged 40 to <60 years. 17 In this study, higher prevalence of comorbidities was found in those over 50 years of age, with regression analysis confirming that the likelihood of comorbidities increases with age. This observation aligns with findings from the Karnataka Rheumatoid Arthritis Comorbidity (KRAC) study, which examined comorbidities in the South Indian population. 18 A study by Renu and Suchita also reported similar findings, with hypertension (22%) and diabetes (10%) being more common in individuals over 50 years of age. 19 Diabetes and hypertension are widely prevalent among the middle-aged and elderly general population across all regions and socioeconomic groups in India. 20 In a comparative study conducted in New York, Fuller et al. reported that the prevalence of comorbidities in RA patients such as COPD and hypertension increases with age, peaking above 50 years. 21 Similarly, a Saudi Arabian retrospective study found that each additional year of age was associated with 8.6% higher odds of comorbidities in RA patients (OR: 1.086, P = .025), highlighting a significant link between age and comorbidities. 8
The KRAC study identified thyroid dysfunction (17.41%) as the most prevalent comorbidity in RA patients, followed by hypertension (14.93%) and diabetes (3.98%). 18 Similarly, Vaghela et al. reported that about 40% of RA patients in Western India had comorbid conditions such as hypertension, diabetes, thyroid dysfunction, hyperlipidaemia and respiratory problems, compared to 11% in the control group. 14 Singh et al. also found hypertension (19.61%) to be the most common comorbidity, followed by diabetes (9.80%) and dyslipidaemia (7.84%). 7 However, this study found the prevalence of hypertension to be 21.87%, diabetes 11.99% and thyroid disorders 14.5%.
Previous studies have shown a 14% prevalence of thyroid disorders in RA patients, which aligns with this study findings of 14.87% in patients over 50 years of age.22,23 Another study reported a higher prevalence of thyroid disorders, around 18%, in RA patients above 50 years. 19 A Saudi Arabia-based study also reported a high prevalence of thyroid disorders among RA patients (26.3%). 24 Additionally, the prevalence observed in this study is slightly higher than the overall thyroid disorder prevalence in the general Indian population, estimated at 12.89%. 25
In the South Indian tribal population, the prevalence of diabetes was 7.4%, and hypertension was 36.5%. Hypertension was associated with older age, female gender, generalised and abdominal obesity and diabetes, with abdominal obesity and hypertension identified as risk factors for diabetes. 26 In the Indian Council of Medical Research–India Diabetes (ICMR-INDIAB) national cross-sectional study of the general population, Anjana et al. reported an overall diabetes prevalence of 11.4%, with the highest proportion in the southern and northern regions of India. 27 According to the International Diabetes Federation, the prevalence of diabetes in the adult general population in India is estimated to be 8.3%, with a higher prevalence of 25.2% in the 45–59 years age group. 28 However, this study reported a diabetes prevalence of 12% in overall RA patients.
This study observed a higher prevalence of hypertension in overall RA patients at 21.87%, which is comparable to the age-standardised prevalence of hypertension in the general population of India (24.2%), with prevalence increasing with age. In the general population, region-wise, prevalence was highest in the South (39%), followed by the North (24%). 29 Regionally, in the general population, the prevalence was highest in the South (39%), followed by the North (24%). However, in this study, the prevalence of hypertension in the South and West regions was similar (23.08% and 23.13%, respectively). Hypertension was prevalent at 35.5% throughout the country, except in the central region. 27
The ICMR-INDIAB nationwide cross-sectional epidemiological study reported an overall prevalence of dyslipidaemia in the general population at 81.2%, which is significantly higher than the 1.27% observed in this study. 30 The discrepancy may be attributed to the fact that the study did not actively screen for dyslipidaemia but only recorded cases among those who were screened. Additionally, the use of hydroxychloroquine might have contributed to the lower prevalence observed. However, hyperlipidaemia was found to increase with the duration of illness.
The Korea National Health and Nutrition Examination Survey (KNHANES) identified hypertension (30.3%), dyslipidaemia (14.1%), diabetes (12.9%), pulmonary tuberculosis (8.6%), thyroid disease (8.0%) and cardiac diseases (5.7%) as the most common comorbidities among RA patients. 31 In contrast, the prevalence of cardiac disease and hyperlipidaemia was much lower in this study (0.71% and 1.27%, respectively). This difference may be attributed to regional variations, lifestyle factors, age of the patient population and genetic predispositions. In this study, a total of 30 patients had cardiac diseases, including 8 with CHD and 14 with ischaemic heart disease (IHD) of which 7 had myocardial infarction. These findings are consistent with the KRAC study conducted in Karnataka, India, which also reported a low prevalence of cardiovascular diseases (6 patients). 18 Dougados et al. found that hypertension (28%) and diabetes (11%) were the most common comorbidities in RA patients, whereas the prevalence of cardiovascular diseases was lower. These findings suggest that cardiovascular diseases may manifest later in RA or may be underdiagnosed in certain populations due to varying clinical approaches. 3 Hypertension (40%), dyslipidaemia (32%) and diabetes (14%) had the highest prevalence among RA patients in their study. Additionally, they found that a longer duration of RA was linked to a higher likelihood of developing multiple comorbidities. 32 This supports the observation that patients with comorbidities in this study had a longer average illness duration of RA. In this study, both hypertension and dyslipidaemia increased with duration of disease. The higher prevalence of multimorbidity noted in females is consistent with studies conducted in Germany and the United States.33,34
In this study, the younger group exhibited a higher prevalence of migraines. One potential explanation is that the link between RA and migraines may involve an underlying autoimmune mechanism. A systematic review and meta-analysis have indicated that migraines frequently coexist with various chronic inflammatory conditions, including RA. 35 In a cross-sectional study, the prevalence of migraines among RA patients was reported to be 28.2%, with a higher occurrence in younger patients. 36
The study involved eight centres across India, ensuring a diverse sample that enhances the generalisability of findings. Data collection followed a standardised proforma to maintain consistency, with trained CRAs and PIs ensuring accuracy. The large sample size strengthened the statistical analysis of comorbidities and their prevalence, despite comorbidity being a secondary objective. The use of the ICD-10 version of the Charlson Comorbidity Index provided a standardised framework for defining and categorising comorbidities.
However, comorbidity data were derived from patient reports and medical charts, posing a potential risk of underreporting or misreporting. Treatment compliance was not assessed, and while cross-sectional disease activity data were collected, the absence of long-term disease activity scores limited conclusions on its impact on comorbidities. However, disease duration was considered in the analysis of comorbidity risk factors.
Although the study population included participants from across India, a larger proportion were from South India. Despite this regional skew, the absence of geographical recruitment restrictions ensured representation from various parts of the country, supporting broader generalisability. The large sample size and multicentre design further reinforce the study’s relevance to the Indian population. Additionally, the lower prevalence of IHD noted in the study could be attributed to the younger mean age of the population (52.42 ± 12.18 years) and the absence of proactive screening for IHD as per the study protocol. This may have led to an underestimation of its true prevalence in the cohort.

Conclusion
The study highlights a significant comorbidity burden in RA patients, with hypertension, thyroid disorders and diabetes being most common. Older age, increasing duration of illness and the Southern region were associated with a higher prevalence of comorbidities. These findings underscore the need for tailored treatment and management strategies to improve outcomes for older RA patients experiencing more chronic conditions.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
Authors are thankful to Debashish Dhanda and Aman Sharma for their participation in an administrative role in the IRA database. The authors acknowledge the help of Research Assist (
Authors’ Contributions
All the authors have contributed equally to the conceptualisation, data capturing and developing of the content.
Rudra Prosad Goswami served as co-investigator and Debashish Danda served as overall in charge of the IRA database. All other authors served as principal investigators from respective centres.
Data Availability
Data will be provided on request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
All participating centres received approval from their respective institutional ethics committees (listed in the appendix). Since this is an observational study, no direct human intervention was involved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors received educational and research grants from Novartis India for developing a database for the Indian Rheumatology Association.
Informed Consent
Written informed consent was obtained from all selected patients following institutional guidelines.
Patient Consent
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.