
Abstract
Dear Editor,
Drug-induced interstitial lung disease (DI-ILD) is a recognised subtype of diffuse parenchymal lung disease (DPLD), accounting for almost 3%-5% of the prevalent ILD cases. 1 The current incidence of DI-ILD, reportedly estimated at 4.1–12.4 per million per year, 2 could be an underestimate considering the significant expansion of newer chemotherapeutic and biological therapies with a higher potential for lung toxicities.1,3 In addition, the increasing awareness and improved diagnostic modalities for ILD have been associated with the increasing overall prevalence of ILD in the last few decades. 4 While more than 400 drugs have been associated with the development of DI-ILD, the most commonly implicated drugs for DI-ILD include disease-modifying antirheumatic drugs (DMARDs), antiarrhythmic medications, as well as antimicrobial, antineoplastic drugs, and immune checkpoint inhibitors (ICIs).1–3 In contrast, rituximab has infrequently been reported as a cause of DI-ILD. A recent study investigating 42 categories of drugs for DI-ILD suggested that epidermal growth factor receptor (EGFR) inhibitors (odds ratio (OR): 16.84) and class III antiarrhythmic drugs (OR: 7.01) were those associated with the highest disease risk. 5 Although maintaining a high level of clinical suspicion is crucial, determining causality for DI-ILD following exposure to a potentially pneumotoxic drug and excluding other causes of ILD can be concerning.
A 59-year-old male, never-smoker, was under treatment for follicular-B-cell type non-Hodgkin’s lymphoma (NHL). He received six cycles of rituximab and bendamustine, followed by seven cycles of rituximab every three months. Before treatment initiation, the thoracic high-resolution computed tomography (HRCT) showed no evidence of lung abnormality. He had a dry cough and gradually increasing shortness of breath during physical activity over four months. His symptoms began nearly two years after he received the first dose of rituximab, with the latest dose administered two months before the onset of symptoms. He reported the absence of any constitutional symptoms, clinical features suggestive of connective tissue diseases and exposure to organic or inorganic dust. Medical history was nonyielding for any other drug exposure except rituximab. The physical examination was notable for exertional desaturation on pulse oximetry and fine end-inspiratory basal crepitations in bilateral chest auscultation.
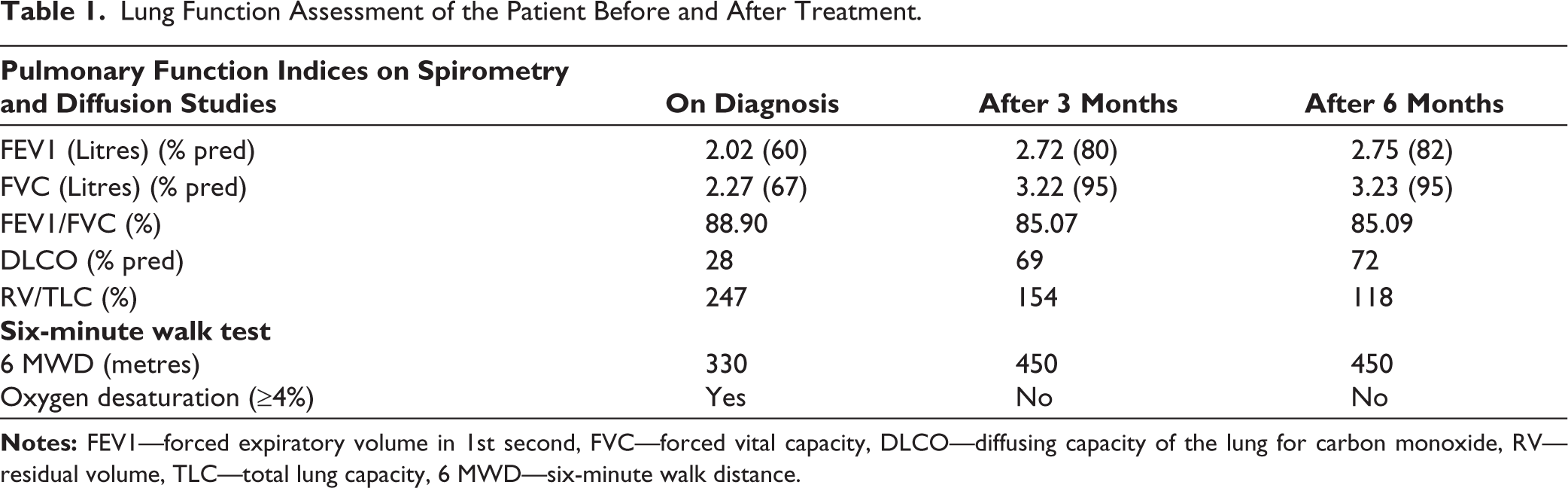
The HRCT chest revealed bilateral diffuse asymmetrical reticular opacities with ground glass attenuation and mild tractional bronchiectasis with no apicobasal gradient, and peripheral subpleural areas of patchy consolidations with peribronchial thickening, suggestive of a nonspecific interstitial pneumonitis (NSIP) pattern with organising pneumonia (OP) (Figure 1A, B). On lung function testing (Table 1), the spirometry showed a restrictive pattern, with severe limitation of the diffusion capacity (DLCO). A broad spectrum of differential diagnoses comes under the DPLD umbrella; therefore, the patient was evaluated step-wise. Infections were ruled out based on microbiological bronchoscopic bronchoalveolar lavage (BAL) analysis. Blood counts, procalcitonin, galactomannan in blood and BAL were within normal ranges. The detailed serological workup of autoimmune markers for connective tissue diseases, including antinuclear antigen (ANA), extractable nuclear antigen (ENA) profile, rheumatoid factor (RF), anticyclic citrullinated peptide (anti-CCP), myositis-specific autoantibodies (MSA) and antineutrophilic cytoplasmic antibodies (ANCA), was negative. BAL cytology showed no evidence of granulomas or malignant cells. Echocardiography showed no cardiac abnormality. Transbronchial lung cryo-biopsy (TBLC) was performed, and the histopathological evaluation confirmed the diagnosis of NSIP (Figure 1C, D). After a multidisciplinary discussion (MDD) among the experts in radiology, pulmonology, immunology and pathology, the patient was diagnosed with rituximab-induced interstitial lung disease (RI-ILD). Treatment with oral corticosteroids was initiated, and rituximab was discontinued. The steroids were tapered gradually and stopped. After six months of oral corticosteroid treatment, the patient showed clinical improvement. Functional assessment showed significant improvement in lung function indices, as shown in Table 1, and radiological improvement in CT chest after six months (Figure 1E, F).
(a and b) High-resolution Computed Tomography (HRCT) of the Chest at the Time of Clinical Presentation, Revealing Bilateral Diffuse Asymmetrical Reticular Opacities (White Arrow) with Ground Glass Attenuation and Mild Tractional Bronchiectasis with No Apicobasal Gradient and Peripheral Subpleural Areas of Patchy Consolidations with Peribronchial Thickening (Black Arrow), Suggestive of a Nonspecific Interstitial Pneumonitis (NSIP) Pattern with Organising Pneumonia (OP); (c and d) The Histopathological Findings on Transbronchial Cryo-biopsy of Lung (TBLC), with Diffuse Infiltration of Alveolar Septae by Moderate Mononuclear Inflammatory Infiltrate and Septal Fibrosis with Pneumocyte Hyperplasia and Alveolar Macrophages in the Alveolar Space Suggestive of NSIP Pattern. Features of OP Are Also Seen in a Few Alveolar Sacs and Bronchioles (Black Arrowhead); (e and f) The Follow-up Imaging with HRCT of the Chest at Six Months After Treatment, Revealing Marked Radiological Resolution.

Rituximab is a chimeric humanised immunoglobulin G1 (IgG1) monoclonal antibody targeting CD-20 expressed over B and pre-B-cells. It destroys B lymphocytes by one of the three potential mechanisms: antibody-dependent cell-mediated cytotoxicity, apoptosis and complement-mediated pathway. 6 Among the rituximab-induced pulmonary adverse effects, though rare, early onset acute and subacute acute respiratory syndrome (ARDS) which occurred following the first cycle and within the second to fourth cycles of rituximab respectively hypersensitivity pneumonitis, diffuse alveolar haemorrhage and late-onset interstitial lung disease, were reported in the literature. In a previous review of RI-ILD, 121 cases were identified with the onset of the disease up to the twelfth cycle of rituximab.7,8 Based on the results retrieved by a literature search, 10 RI-ILD cases have been reported in India, as listed in Table 2.9–13 In this case, the onset of symptoms was after 13 cycles of rituximab, which was quite outlandish compared to cases reported in the literature. As per the modified criteria to diagnose DI-ILD, including the onset of symptoms, temporal association with exposure, exclusion of other causes of the interstitial pneumonitis, resolution on withdrawal of the drug and positive rechallenge testing, our case met all the criteria except the rechallenge testing. 7
Lung Function Assessment of the Patient Before and After Treatment.
Clinical Details of Rituximab-induced Interstitial Lung Disease Cases from India.
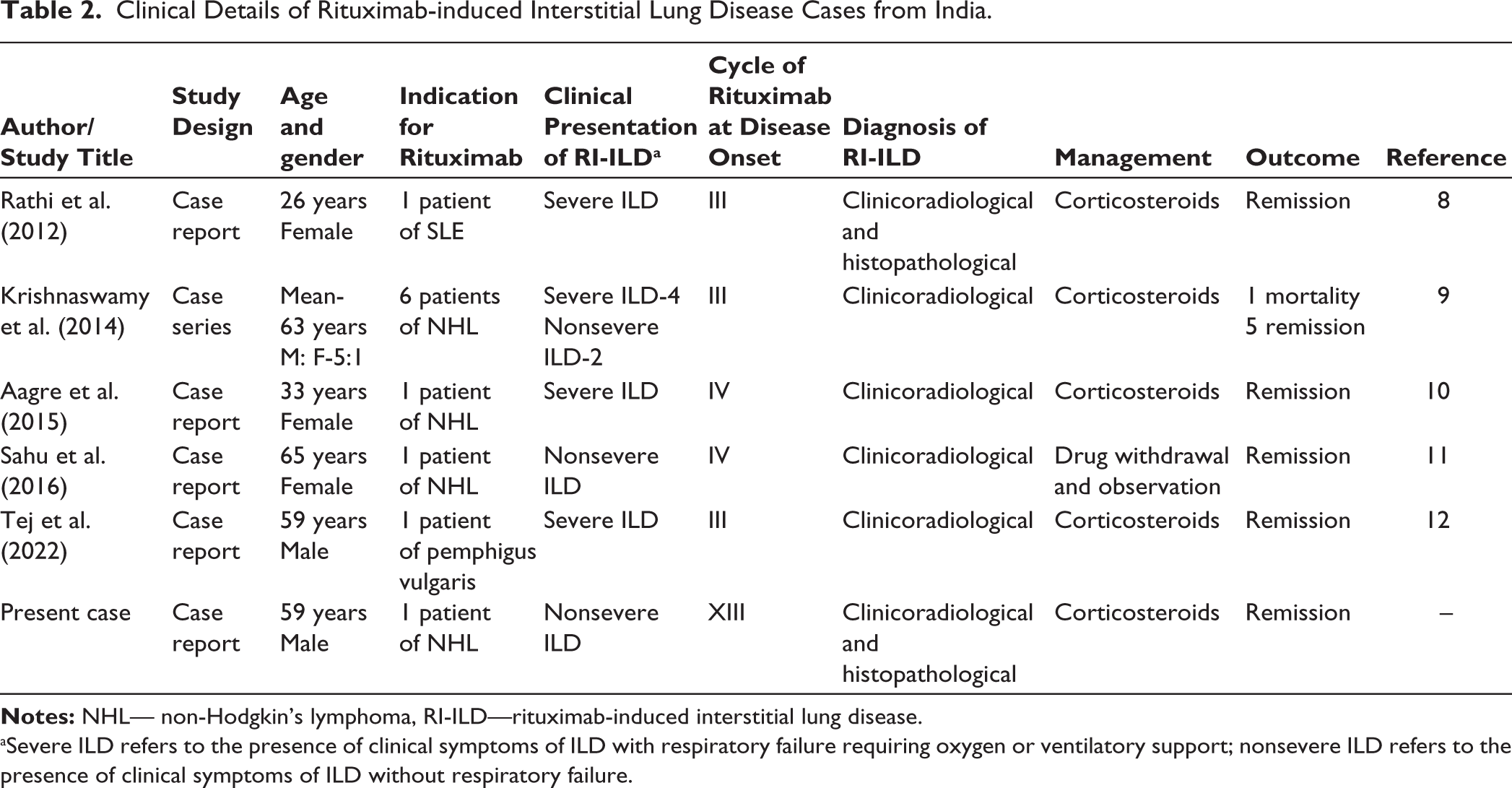
aSevere ILD refers to the presence of clinical symptoms of ILD with respiratory failure requiring oxygen or ventilatory support; nonsevere ILD refers to the presence of clinical symptoms of ILD without respiratory failure.
There is no specific radiological pattern for DI-ILD. However, among the reported cases, common findings include bilateral diffuse infiltrates, ground-glass opacities, with or without focal or diffuse consolidation and reticular abnormalities. 9 Though not typical, likely OP and NSIP patterns are most commonly evident in DI-ILD, as seen in our case.7–10,14 The common histological patterns are OP, isolated or associated nonspecific interstitial pneumonia and usual interstitial pneumonitis. 2 The exact pathogenesis for the causation of diffuse parenchymal lung disease by rituximab was uncertain. Early-onset ARDS or acute ILD may be due to the hypersensitivity reaction and inflammatory cytokine activation, while chronic late-onset ILD has varied pathogenesis. Rituximab binds with CD20+ B-cells which triggers the trail of events including B-cell signalling and apoptosis of lymphocytes, complement cascade activation and cytokine release, which is responsible for the infusion reactions, antibody-mediated cell damage and lymphocytic crosstalk following B-cell destruction, causing cytotoxic T-cell dysregulation leading to lung injury. Cross-reactivity between lung and tumour antigens could also be a plausible explanation for generating self-reactive clones precipitating lung damage. Rituximab infusion can incite a significant increase in complement activation products, including C3b/c and C4b/c, along with cytokines interleukin-6 (IL-6), IL-8 and tumour necrosis factor-α (TNF-α), among which TNF-α is proposed to be a major cytokine with proinflammatory properties in the pathogenesis of ILD, inducing chemokines, angiogenic factors and other inflammatory cytokines.7–18
The primary objective of this case report is to enlighten physicians about important considerations when treating patients with rituximab. First, the clinician should be aware of the potential pulmonary side effects of the medication and should rule out any pre-existing pulmonary abnormalities before starting treatment. Second, to prevent acute ILD or hypersensitivity reactions during administration, it is suggested that an increased dose of glucocorticoids be administered beforehand. 19 Third, it is crucial to monitor for any respiratory symptoms during and after rituximab therapy and to appraise appropriately with chest imaging. While the onset of symptoms was commonly seen around the fourth cycle, there are instances where RI-ILD can develop later, 8 as seen in this case, where symptoms appeared after the thirteenth cycle of administration, which spotlighted the necessity of maintaining vigilance over time. Fourth, early glucocorticoid intervention promotes rapid recovery and is recommended to prevent permanent lung damage and halt the disease progression.7,20 Lastly, rechallenge with rituximab in patients with drug-induced pulmonary manifestations is usually not recommended but may be considered with a high dosage of glucocorticoids in inevitable circumstances.7,10
In conclusion, this case highlights the potential for rituximab to cause DI-ILD, even after extended use (13 cycles in this instance). Even with the same drug, diagnosing DI-ILD is challenging due to the nonspecific and variable clinical, laboratory, radiological and histological features, mandating a MDD among pulmonologists, radiologists, rheumatologists and pathologists to establish the diagnosis. Early recognition, clinical suspicion and prompt corticosteroid treatment are critical for managing DI-ILD and improving outcomes. Monitoring respiratory symptoms and chest imaging during and after rituximab treatment is essential, as delayed onset can occur. Clinicians should be aware of the pulmonary side effects of rituximab and take preventive measures when administering the drug.
Footnotes
Authors’ Contribution
Priyadarshini S and Mansi Gupta helped with data collection, data organisation and writing of the original draft preparation, review and editing. All authors have contributed to reviewing and editing the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship and/or publication of this article.
Ethical Approval
Since this is a case-based review, approval was not mandatory per the institutional review board (IRB).
Funding
The authors received no financial support for the research, authorship and/ or publication of this article.
Patient Consent
Informed consent was obtained from the patient for publication.