
Abstract
Introduction:
Assessment of disease activity in patients with rheumatoid arthritis (RA) is usually performed using disease activity indices such as the Disease Activity Score 28 (DAS28) and the Clinical Disease Activity Index (CDAI), both of which require formal joint assessment and are therefore time consuming. The Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5) is a relatively newer, patient-based RA disease activity index that does not require formal joint assessment and is thus more suitable for use in a clinic. We translated RADAI-5 into Punjabi language for use in the Indian Punjabi population and evaluated its correlation with DAS28 and CDAI.
Materials and Methods:
During the first 2 months of the study, the RADAI-5 was translated into Punjabi language and validated amongst 45 RA patients. Then, 200 patients were enrolled, and their disease activity was assessed using the Punjabi RADAI-5, CDAI and DAS28. The correlation and level of agreement between the disease activity indices were analysed using the Spearman correlation coefficient and Cohen’s kappa coefficient.
Results:
The newly synthesised Punjabi version of RADAI-5 was found to have psychometric properties of feasibility, internal consistency and validity. Furthermore, the Punjabi version of RADAI-5 showed a strong correlation with DAS28 and CDAI (r = 0.868 and 0.869, both at P < .0001) and a fair level of agreement with both DAS28 (k = 0.391, P = .0001) and CDAI (k = 0.391, P = .006).
Conclusion:
The Punjabi version of RADAI-5 is a valid instrument. It has a strong positive correlation and a fair level of agreement with both DAS28 and CDAI, thus yielding similar information on disease activity as DAS28 and CDAI.
Keywords
Main Points
We translated Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5) into Punjabi language and validated the Punjabi language version (‘Punjabi’ is the native language of Punjab, India)
The newly synthesised Punjabi version of RADAI-5 was found to have psychometric properties of feasibility, internal consistency and validity.
The Punjabi version of RADAI-5 showed a strong correlation with Disease Activity Score 28 (DAS28) (r = 0.868, P < .0001) and Clinical Disease Activity Index (CDAI) (r = 0.869, P < .0001).
Punjabi RADAI-5 demonstrated a fair level of agreement with DAS28 (k = 0.391, P = .0001) and CDAI (k = 0.391, P = .006).
Introduction
Rheumatoid arthritis is a chronic autoimmune inflammatory disease with articular and extra-articular involvement. The natural course of rheumatoid arthritis (RA) includes exacerbations and remissions, which are important to identify early to escalate or de-escalate the treatment and thus help prevent permanent joint deformity and toxicity from disease-modifying antirheumatic drugs (DMARDs) used in the treatment of rheumatoid arthritis. Regular and timely assessment of disease activity thus forms a cornerstone of an appropriate treatment strategy for rheumatoid arthritis.
The conventional scoring systems used to assess disease activity in rheumatoid arthritis, such as Disease Activity Score 28 (DAS28) and Clinical Disease Activity Index (CDAI), are based on formal joint examination done by the physician, which is time-consuming and not practical in a busy outpatient department (OPD), particularly in a country like India where the disease burden is high. 1 Active disease in RA causes joint tenderness, stiffness, limitation of movement and impairment in overall quality of life. Since these are subjective phenomena, patients themselves can grade them on a Likert scale, which can lead to an adequate assessment of disease activity. Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5) is a relatively newer and less studied index that is based on this concept. RADAI-5 includes only patient-reported outcome measures and may be more practical in a resource-limited setting, as it does not involve a formal joint count. It can classify disease activity as near-remission, low disease activity, moderate disease activity and high disease activity, just as the conventional indices.
The RADAI-5 scoring system has not yet been studied in the Indian Punjabi population. We aimed to translate RADAI-5 into a Punjabi version with the intent to cater to most of the Indian Punjabi population visiting the study hospital, as Punjabi is the native language in this part of India and easily understood even by the uneducated strata of the society.
However, it is important to know if this cross-culturally adapted index yields similar information as provided by formal joint count-based indices like DAS28 and CDAI. Hence, we aimed to study the correlation and agreement of the Punjabi version of the RADAI-5 index with the joint count-based indices DAS28 and CDAI. If the correlation is good, RADAI-5 can be used for patient care in clinical practice to make treatment decisions, as it is quick to administer, requires no investigations and no examination by the physician. It is a patient-based score, so it can be self-administered from time to time and, hence, help the patient recognise any flare at home itself and seek physician’s advice early.
Methods
Ethical clearance for this study was obtained from the Institutional Ethics Committee.
Study Design
Adult patients with RA (those who met the 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for RA) visiting the Medicine and Rheumatology OPD at a tertiary care hospital and medical college in Punjab, India, and consenting to participate in the study were enrolled in this prospective study over a period of 2 years. Written informed consent was obtained from the patients in English, Punjabi or Hindi language (whichever they best understood) in the presence of a witness (staff or patient’s family member). A total of 245 patients (45 patients for assessing the validity of the newly synthesised Punjabi version of RADAI-5, and 200 patients to study the correlation and agreement of RADAI-5 with other disease activity indices) were enrolled. Patients who were severely anaemic (haemoglobin <7 g/dL) or had pre-existing renal, cardiac, liver or pulmonary disease were excluded from the study. These exclusion criteria were chosen to minimise the confounding factors that could alter a patient’s answers to various questions of RADAI-5. For the translation and validation of RADAI-5 in the Punjabi language, the initial 2 months of the study were contemplated, and 45 patients were enrolled for this part of study.
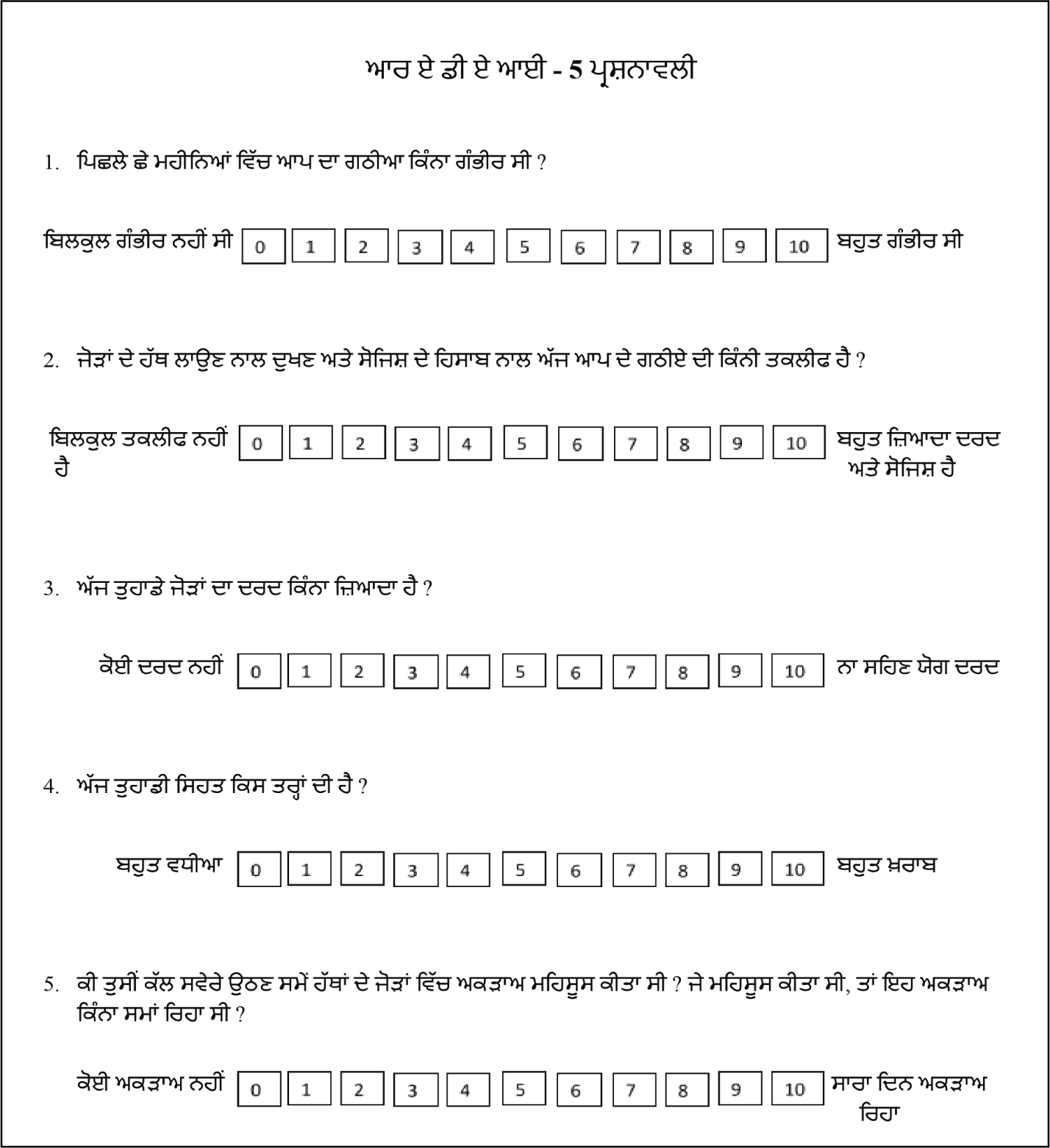
For analysing the correlation of the Punjabi version of RADAI-5 (Figure 5) with DAS28 and CDAI, a further 200 patients were enrolled. This sample size was deemed appropriate as per the standard formula for sample size in correlation studies. 2 The sample size required to conclude results with >80% power of study and a correlation coefficient of 0.21 (the minimum possible r value for correlation to exist) was 176, and this study included 200 patients to increase the power. 3
RADAI-5 was translated into Punjabi after seeking permission from the developer, Dr Burkhard Leeb.
Step 1: Translation of RADAI-5 into Punjabi Language
The English version of RADAI-5 was translated into Punjabi version using the standard guidelines of the American Association of Orthopaedic Surgeons (AAOS).4,5 The AAOS guidelines have been previously used for the translation of RA disease activity measuring indices into other languages, including translation of RADAI into Thai language 6 and RADAI-5 into Turkish language. 7
Steps of Translation Process
Forward Translation
Two translators (whose mother tongue was Punjabi) independently translated the original RADAI-5 into the Punjabi version. One translation was done by a resident doctor (person 1) and the other by a translator (person 2).
Selection and Synthesis of the Most Appropriate Punjabi Translated Version
A team of two members, both doctors and hospital faculty members (persons 3 and 4), then reviewed the two translations and selected the more appropriate one. Further changes were made by the team to make the chosen Punjabi version of RADAI-5 conceptually equivalent to the original RADAI-5, yet simple enough to be understood even by the uneducated section of the population.
Backward Translation
This Punjabi version of RADAI-5 was then translated back into English by a doctor and faculty member (person 5) and an English teacher (person 6). Both were unfamiliar with the original English version of RADAI-5. The back-translated versions were compared to the original RADAI-5 by the doctor and the English teacher (persons 5 and 6). It was then concluded that the back-translated forms almost matched the original RADAI-5.
Review of Forward and Backward Translation and Choosing a Final Version
The forward translation of RADAI-5 into Punjabi and the backward translation of the Punjabi version of RADAI-5 into English were then extensively compared with the original version of RADAI-5 by a team consisting of person 3, person 4, a forward translator (person 1) and a backward translator (person 5). They were compared and assessed on a question-to-question basis, and the existence of their conceptual equivalence was established. Any discrepancies were resolved, and grammar was reviewed. The simplicity of words in the question was reviewed, and the clarity of question was also assessed. Then, a final version of the Punjabi RADAI-5 was selected. This was pretested on the RA patients visiting the OPD for 3 days by the above-mentioned team and was found to be easily comprehended by patients, easy to understand and was able to convey to patients the purpose of each question, with every question being different without repetition.
Step 2: To Assess Psychometric Properties (Reliability, Feasibility and Validity) of the Punjabi Version of RADAI-5
To be able to use the translated Punjabi version of RADAI-5, its psychometric properties (reliability, feasibility and validity) were tested during the first 2 months of the study. In this 2-month period, 45 patients were enrolled, and their Punjabi version of RADAI-5 scores were obtained along with DAS28 and CDAI. Statistical analyses were then applied to assess the Punjabi version of RADAI-5. Reliability was assessed by measuring internal consistency using Cronbach’s alpha, and item analysis was carried out using item-total correlation scores. Feasibility was assessed by evaluating floor and ceiling effects in the Punjabi RADAI-5. To establish validity, the convergent validity method was used, and correlations between the Punjabi version of RADAI-5 and DAS-28, CDAI, erythrocyte sedimentation rate (ESR), swollen joint count (SJC), tender joint count (TJC), patient global evaluation (PGE) and evaluators global assessment (EGA) were assessed. Once the newly synthesised Punjabi version of RADAI-5 was found to be valid statistically, it was then used for further study.
Step 3: Comparison of Punjabi Version of RADAI-5 with DAS28 and CDAI
A total of 200 patients were recruited to study the correlation of the Punjabi version of RADAI-5 with DAS28 and CDAI. A proforma including demographic profile of the patient, vitals, latest value of ESR (by Westergren method), lab results, presence or absence of deformities, patient global assessment (PGA) score, EGA score, general health (GH) score and parameters of DAS28, CDAI and RADAI-5 was completed for each study patient. Formal joint examination was done for 28 joints to record SJC and TJC. For computation of the score of the Punjabi version of RADAI-5, a questionnaire (for self-filling or narrated in Punjabi to the patient by the interviewer, with answers recorded for scoring) containing five self-explanatory questions in Punjabi was administered, and the patients had to score those items on a 0–10 ordered category scale. The RADAI-5 score obtained by adding the scores of these five questions. DAS28 (ESR) and CDAI were computed using the formula:
DAS28 = 0.56 √TJC + 0.28 √SJC + 0.70(log ESR) + 0.014(GH) CDAI = TJC + SJC + PGA + EGA
Statistical Analysis
After statistically validating the Punjabi version of RADAI-5, 200 OPD RA patients were enrolled, and the data generated was simplified and arranged in Excel sheets. Scores for DAS28, CDAI and the Punjabi version of RADAI-5 were obtained. The Spearman correlation coefficient was used to study the correlation between RADAI-5 and DAS28, and between RADAI-5 and CDAI. Kappa agreement statistics was used to study the level of agreement between the disease activity indices.
The statistical analysis was done using SPSS software (Statistical Package for the Social Science) SPSS version 21 statistical program for Microsoft Windows. A probability value (P value) less than .05 was considered statistically significant.
Outcome Assessment
The Punjabi version of RADAI-5 was studied and validated using statistical analyses including Cronbach’s alpha, Spearman’s correlation coefficient and floor/ceiling effect to establish internal consistency, feasibility, criterion validity and construct validity. A Cronbach’s alpha value of >0.7 was considered indicative of a good level of internal consistency. 8 Spearman’s coefficient value of >0.6 was suggestive of a strong correlation. 3 Kappa agreement statistics value of >0.21 was interpreted as a fair level of agreement. 9
Results
Validation of RADAI-5 in Punjabi language
After translating the RADAI-5 into Punjabi version, 45 patients with RA visiting the OPD were recruited during the first 2 months of the study period to validate the new Punjabi version of RADAI-5.The mean age of these patients was 46.93 ± 13.43 years. The mean (± SD) scores for question 1 (Q1), question 2 (Q2), question 3 (Q3), question 4 (Q4) and question 5 (Q5) of the Punjabi version of RADAI-5 were 6.11 ± 2.66, 5.53 ± 2.94, 3.76 ± 2.99, 3.51 ± 2.51 and 0.93 ± 1.34, respectively.
Item analysis showed the item-total correlation coefficients for questions 1–5 of 0.411, 0.596, 0.702, 0.521 and 0.368, respectively (each >0.3, thus signifying good discriminatory power for each question). The Cronbach’s alpha value for this 5-item questionnaire of the Punjabi version of RADAI-5 was 0.745, indicating a good level of internal consistency.
The mean RADAI-5 score was 3.97 ± 1.80, with the lowest RADAI-5 score of 0.40 and the highest RADAI-5 score of 6.80. Only one patient had the lowest RADAI-5 score of 0.4, and only one patient had the highest RADAI-5 score of 6.8. No patient scored 0 or 10; thus, there was no floor or ceiling effects. This aids in the feasibility check of the RADAI-5 in the Punjabi language.
The Spearman correlation coefficient of the Punjabi translated RADAI-5 with DAS28 and CDAI was 0.835 (P < .0001) and 0.797 (P < .0001), respectively. These correlations were calculated to assess the criterion validity of the Punjabi version of RADAI-5. Both values are statistically significant, thus fulfilling the criterion validity.
For evaluating the construct validity of the Punjabi version of RADAI-5, the correlation between the scores of the Punjabi version of RADAI-5 and ESR, SJC, TJC, PGA and EGA was assessed using Spearman’s correlation coefficient. The coefficients were 0.650, 0.567, 0.764, 0.758 and 0.779, respectively, all with P < .0001. These results established the construct validity of the Punjabi version of RADAI-5.
Establishment of Correlation and Agreement Level of Punjabi RADAI-5 with DAS28 and CDAI
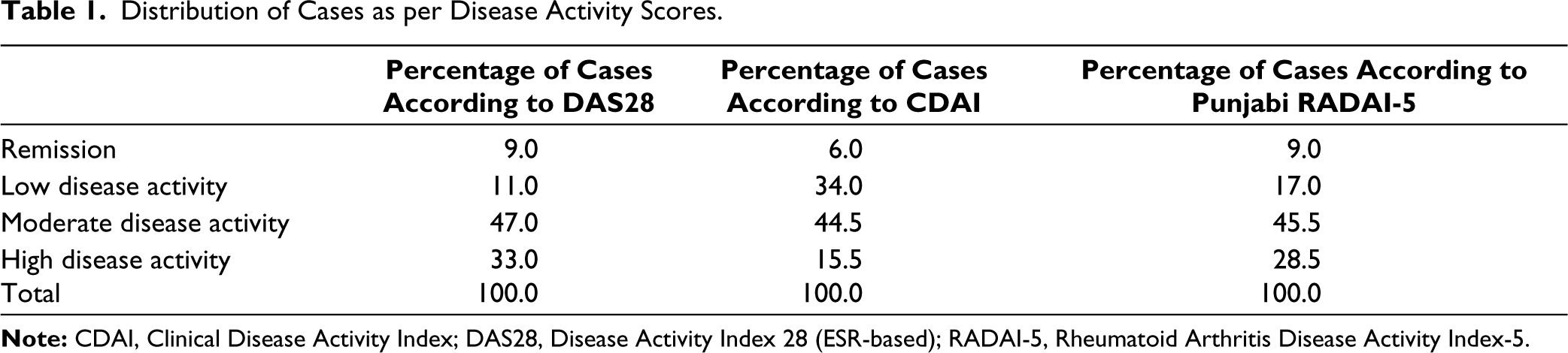
DAS28 ESR-based scores, CDAI and Punjabi RADAI-5 scores were calculated for all 200 patients, with mean values (±SD) of 4.38 ± 1.23, 13.79 ± 7.81 and 4.3 ± 1.74, respectively. Based on these scores, the patients were classified into disease activity categories of remission, low disease activity, moderate disease activity and high disease activity (see Table 1).
Distribution of Cases as per Disease Activity Scores.
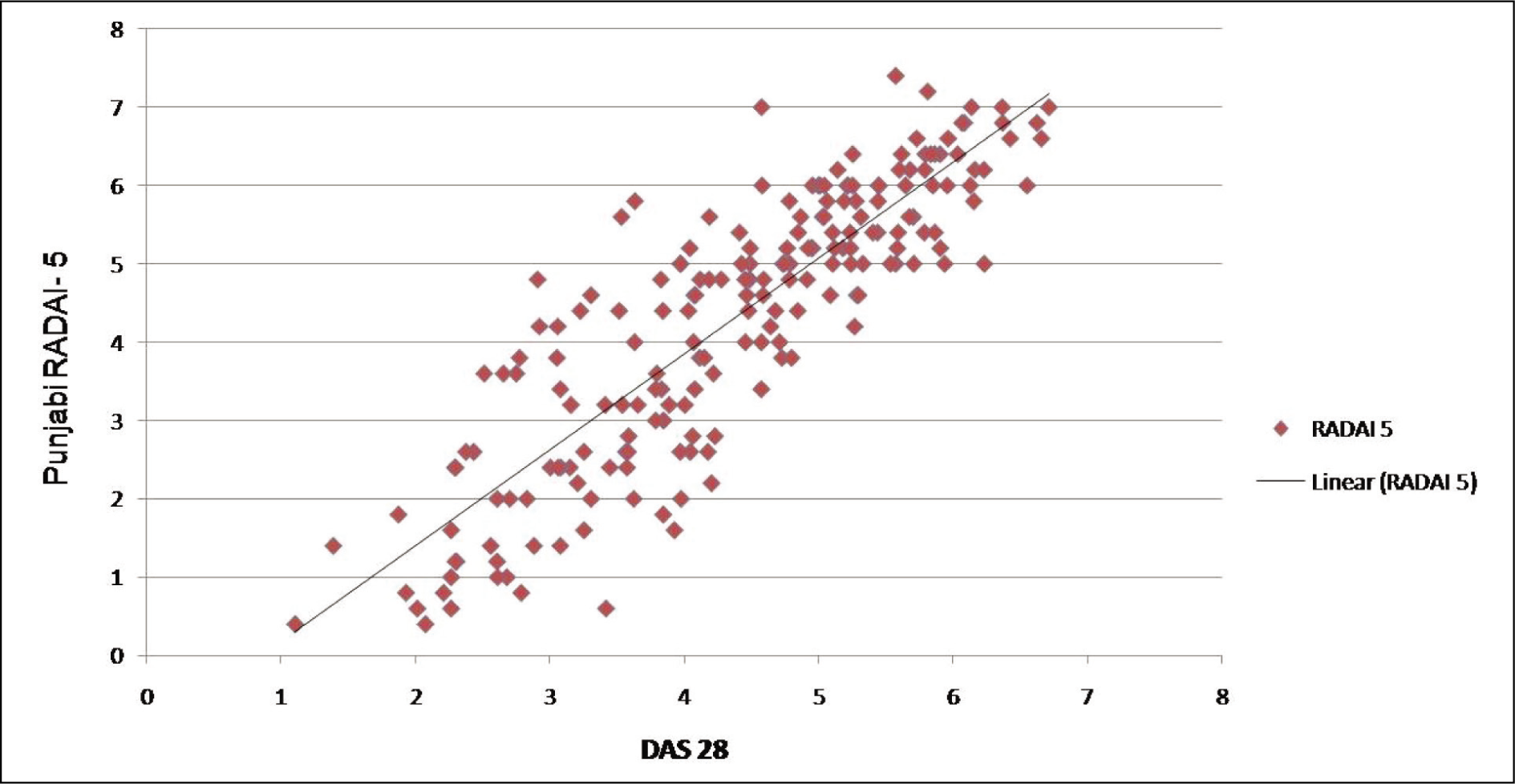
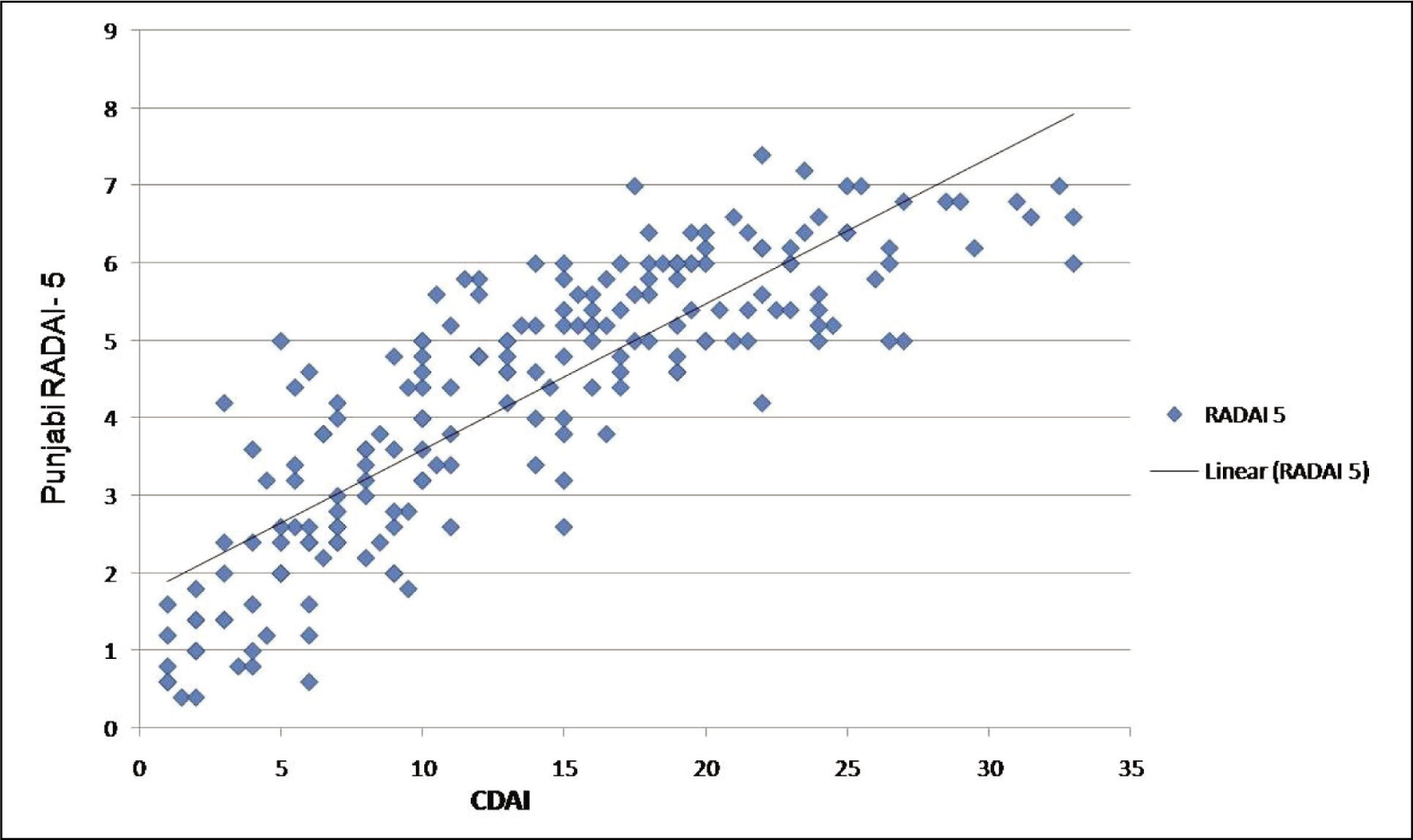
Spearman’s correlation coefficient of the Punjabi version of RADAI-5 with DAS28 was 0.868 (P < .0001) and with CDAI was 0.869 (P < .0001), indicating a strong positive correlation of the Punjabi version of RADAI-5 with both DAS28 and CDAI (see Figures 1 and 2).
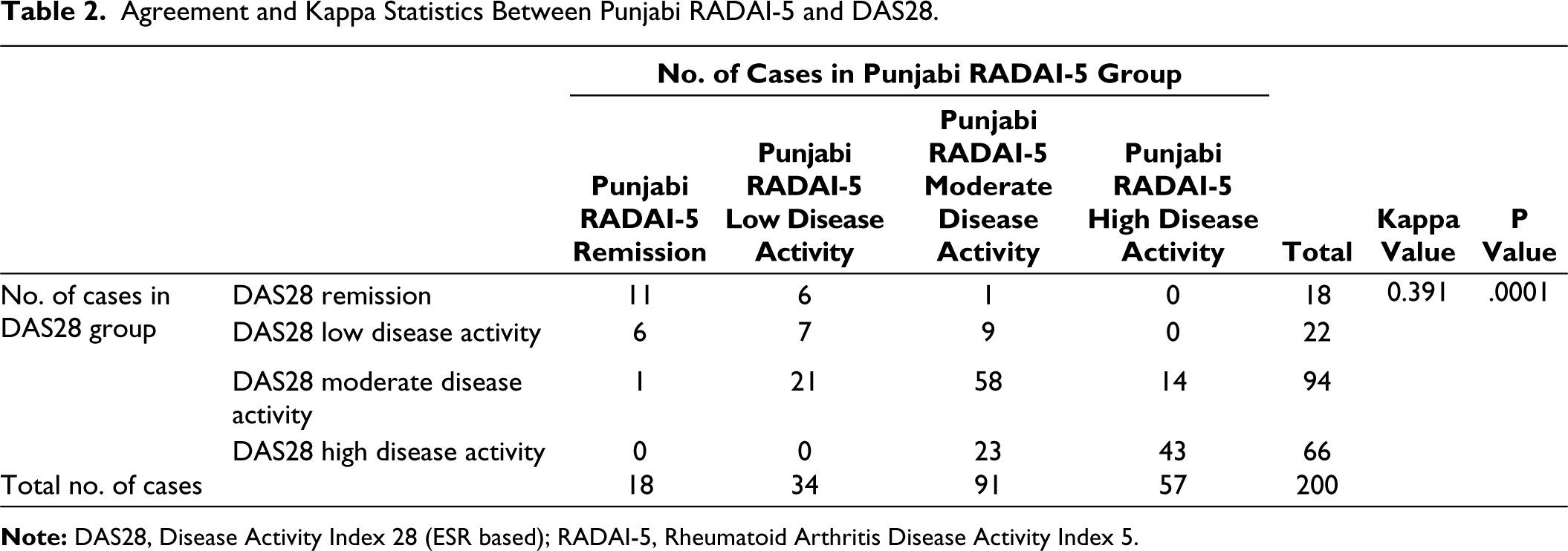
The level of agreement between the indices was assessed using Cohen’s kappa statistics (κ).
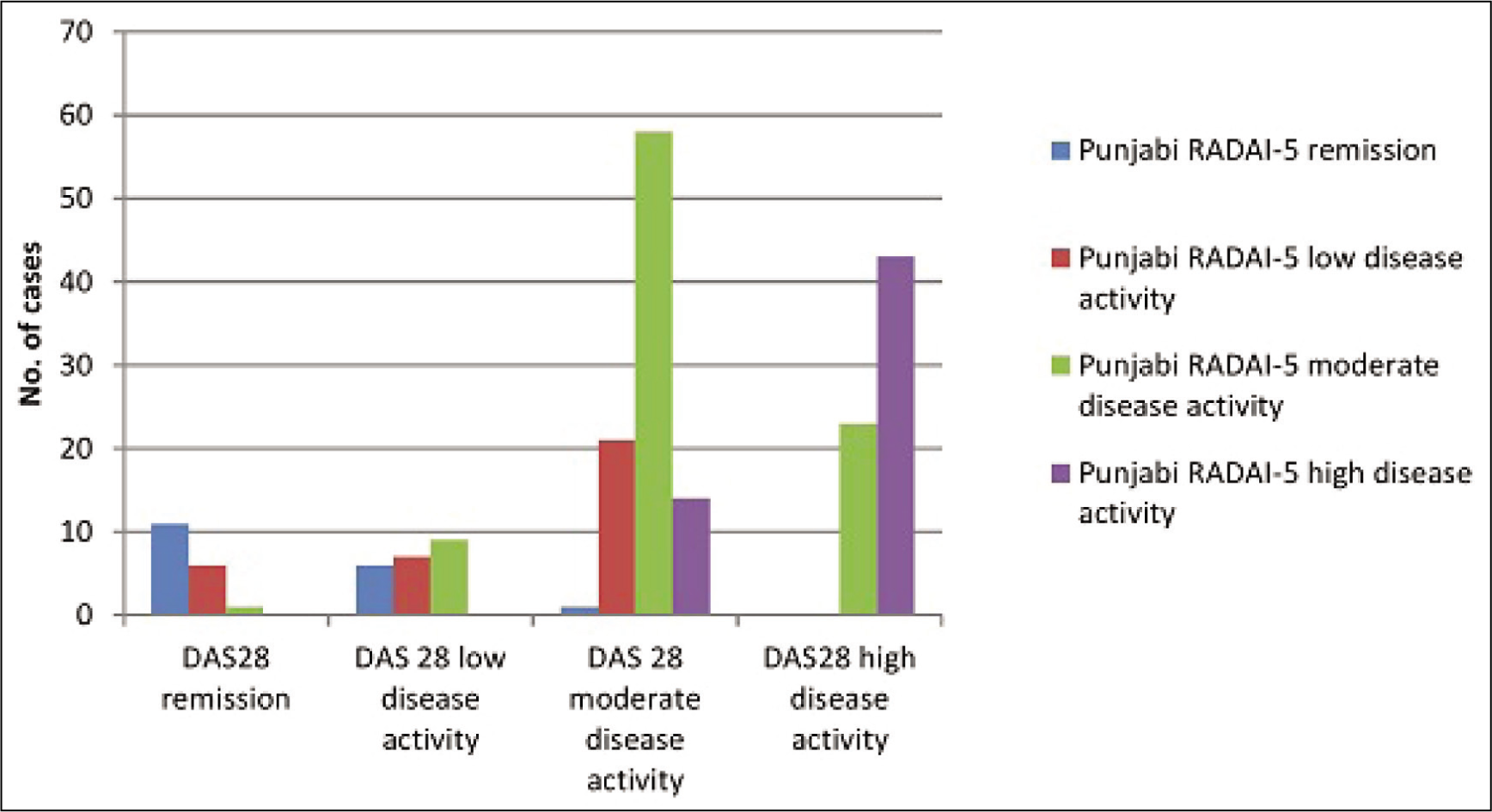
There was a fair level of agreement between the Punjabi version of RADAI-5 and DAS28, with κ = 0.391 (P = .0001), as shown in Table 2 and Figure 3.
Agreement and Kappa Statistics Between Punjabi RADAI-5 and DAS28.
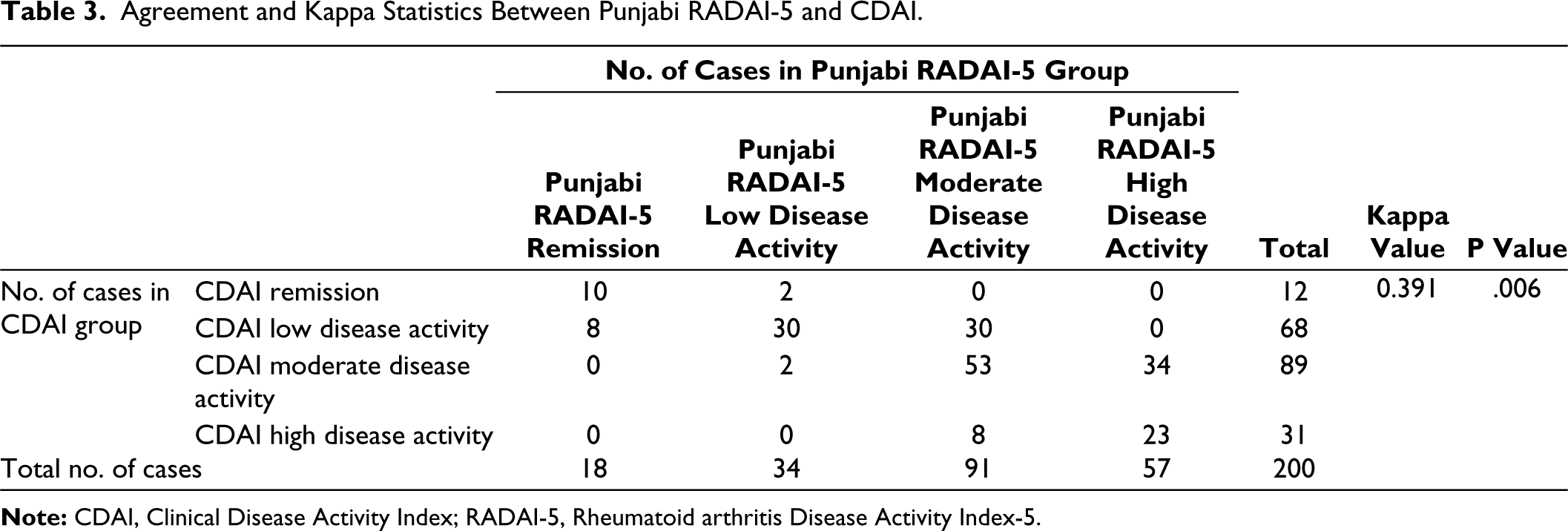
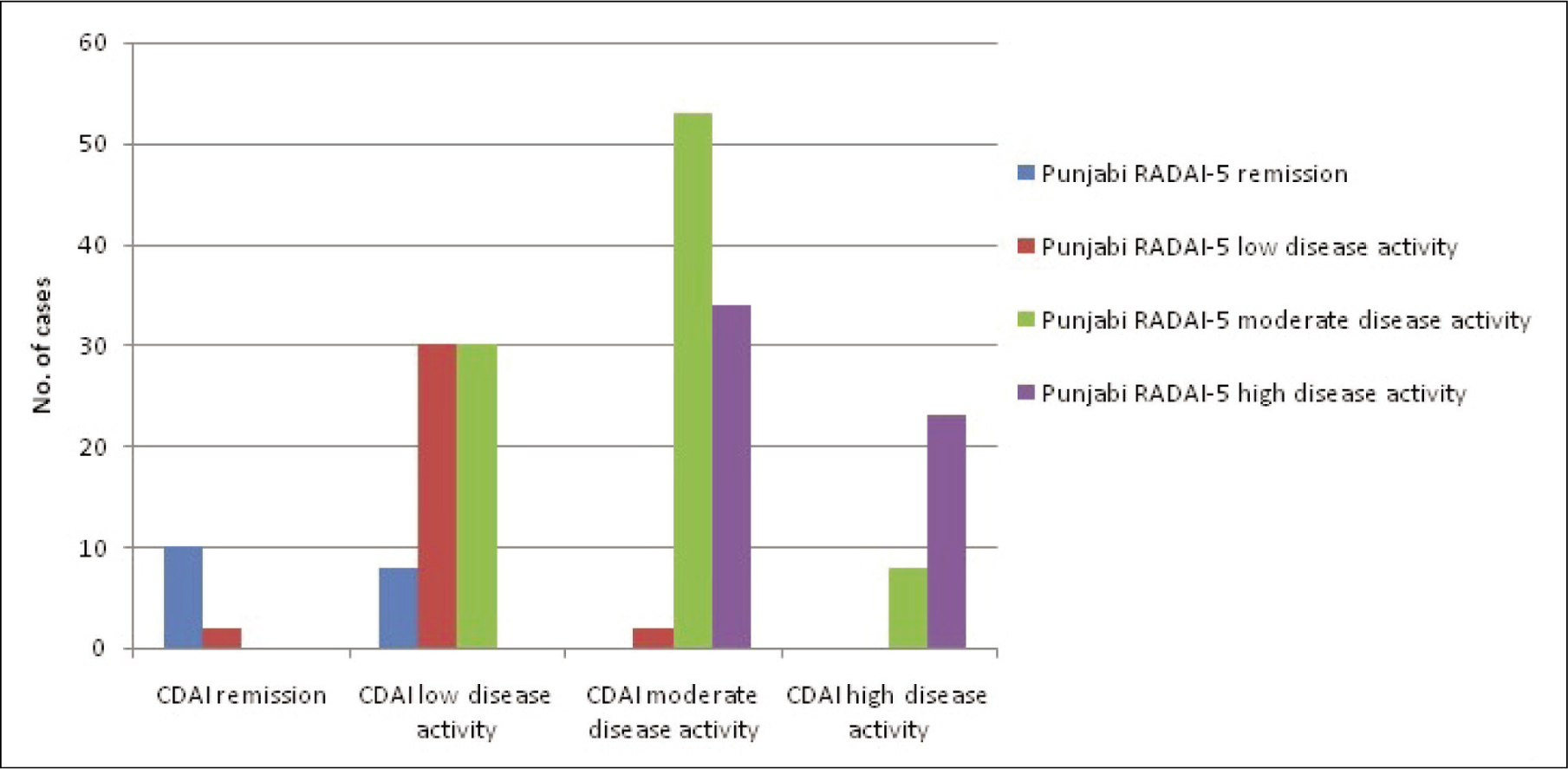
Kappa statistics when applied between RADAI-5 and CDAI resulted in a similar fair level of agreement with κ = 0.391 (P = .006), as shown in Table 3 and Figure 4.
Agreement and Kappa Statistics Between Punjabi RADAI-5 and CDAI.
Discussion
We found the newly synthesised Punjabi version of RADAI-5 to have psychometric properties of feasibility, internal consistency and construct validity. Feasibility was established as the percentage of patients with the lowest and highest possible RADAI-5 scores was <15%, indicating no floor or ceiling effects. 10 Reliability of the Punjabi version of RADAI-5 was evaluated based on internal consistency, calculated using Cronbach’s alpha, which was 0.745, indicating a good level of internal consistency. 8 Further, this also signifies that the questions in the Punjabi version of RADAI-5 demonstrate interrelatedness amongst themselves, have a homogeneous construct and are not redundant. The psychometric property of validity of the Punjabi version of RADAI-5 was evaluated in terms of criterion and construct validity. 11 Criterion validity was established by the strong correlation of the Punjabi version of RADAI-5 with DAS28 and CDAI. 3 Construct validity was assessed using convergent validity and was confirmed by the positive correlations between the scores of the Punjabi version of RADAI-5 and ESR, SJC, TJC, PGA and EGA.
Hence, it was concluded that the Punjabi version of RADAI-5 is a feasible, reliable and valid questionnaire that is easy to administer and can be used in RA patients to assess disease activity. Furthermore, we found the Punjabi version of RADAI-5 to have a strong correlation with DAS28 and CDAI. A fair level of agreement was seen between the Punjabi version of RADAI-5 and both DAS28 and CDAI for disease activity category classification.
RADAI-5 has been previously translated and validated for use in the Turkish language by Sunar et al. 7 and RADAI has been translated and validated for use in the Thai language by Katchamart et al. 6 Both studies found the translated versions of RADAI-5 or RADAI to be feasible, valid and reliable, with significant correlations to disease activity measures (the Turkish version of RADAI-5 with DAS28 and the Thai version of RADAI with both DAS28 and CDAI).6,7 Similar to these findings, we also found the Punjabi version of RADAI-5 to be feasible, valid and reliable, and strongly correlated with DAS28 and CDAI.
Tanwar et al. 12 in a 3-month follow-up study amongst 100 RA patients reported a significant correlation of RADAI-5 with DAS28 and CDAI, with an average agreement between DAS28 and CDAI. In a study of 169 RA patients by Leeb et al. 13 the correlation of RADAI-5 with both DAS28 and CDAI was statistically significant, with a fair level of agreement with both indices. Bossert et al. 14 also reached a similar conclusion from their cross-sectional study on 200 patients. Similarly, Singh et al. 15 found RADAI-5 to be statistically correlated with DAS28 and CDAI.
Conclusion
The Punjabi version of RADAI-5 is a valid, reliable and feasible instrument. It demonstrated a strong correlation with both DAS28 and CDAI. Also, the different disease activity categories as per Punjabi RADAI-5 were in agreement with those by DAS28 and CDAI. Hence, the Punjabi version of RADAI-5 yields similar information on disease activity as that provided by DAS28 and CDAI, and therefore can be used to assess disease activity without the need for ESR or CRP values or formal joint counts by the physician. Thus, it seems to be an appropriate alternative to assess disease activity when compared to conventional indices DAS28 and CDAI. Hence, the Punjabi version of RADAI-5 is an appropriate disease activity index for use in the Indian Punjabi population in a busy OPD.
Footnotes
Declaration of Conflicting Interests
The manuscript is the original work of the authors carried out at Dayanand Medical College & Hospital, Ludhiana, Punjab, India, a tertiary care hospital. The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The data are available with the corresponding author and can be reproduced if required.
Ethical Approval
The ethical approval was obtained from the institution’s ethics committee (No. BFUHS/2k21p-TH/5021).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from all the patients.