
Abstract

Introduction
Chronic nonbacterial osteomyelitis (CNO) and juvenile spondyloarthritis (SpA; enthesitis-related arthritis, ERA) are two paediatric inflammatory diseases that share clinical similarities, leading to significant overlap due to their respective extra-bony and extra-articular manifestations. The clinical features of both diseases may overlap, making it difficult to differentiate between the two entities.
Case Report
A 19-year-old male presented with a history of episodic bilateral thigh pain since the age of 10 years (2015). Each episode lasted approximately two weeks and was episodic rather than nocturnal, with transient relief from nonsteroidal anti-inflammatory drugs (NSAIDs). He denied any history of inflammatory low back pain, arthritis, extra-articular symptoms, rash, fever or constitutional symptoms. A family history revealed SpA in his mother and grandmother, both managed with NSAIDs on an as-needed basis; however, their HLA-B27 status was unavailable.
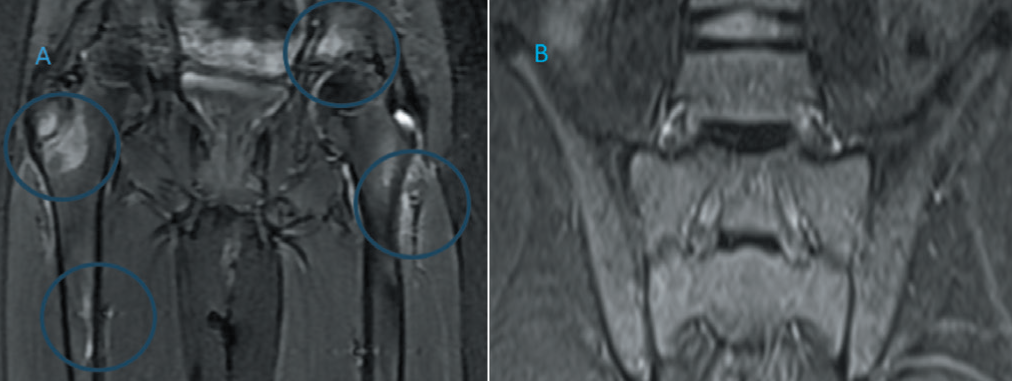
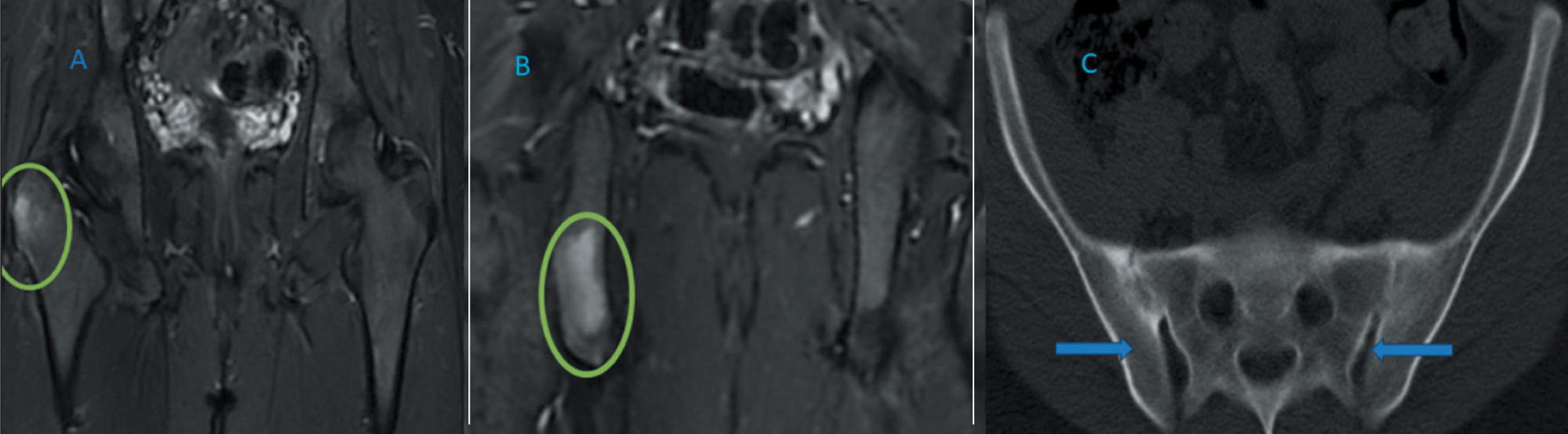
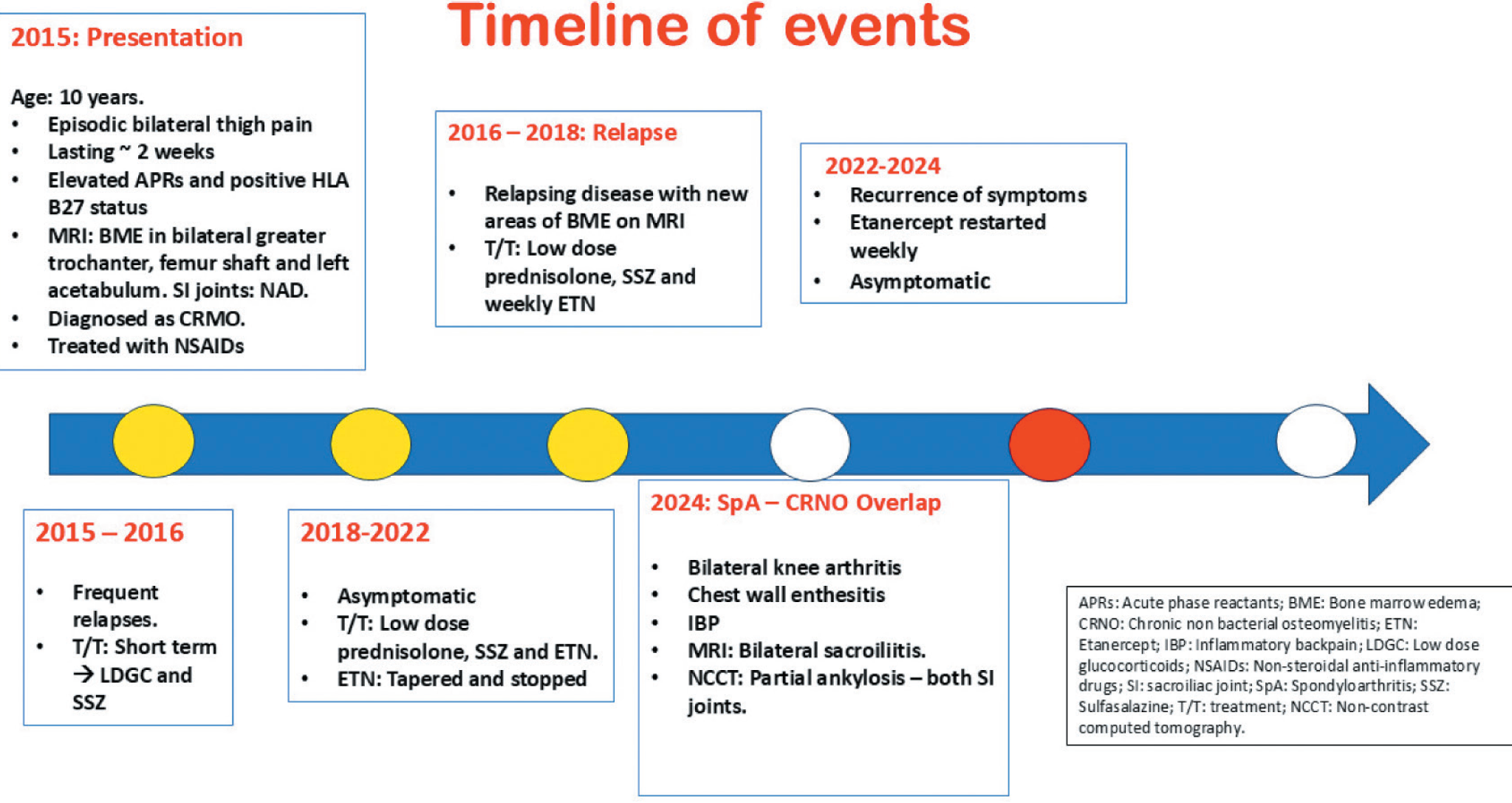
On examination, he had localised tenderness in the right mid-thigh. The rest of the systemic examination was unremarkable. Investigations revealed elevated acute phase reactants (ESR: 67 mm/hr, CRP: 87 mg/dL), and his HLA-B27 by polymerase chain reaction (PCR) was positive. The remaining haematological and biochemical parameters were normal. Whole-body magnetic resonance imaging (MRI) revealed bone marrow oedema (BME) in the bilateral greater trochanters, the proximal shaft of the femur and the roof of the acetabulum on the left side, with normal sacroiliac joints (Figure 1, panels A and B). After ruling out infectious and malignant aetiologies, he was diagnosed with CNO and started on naproxen 250 mg twice a day (2015). Initially, he responded to treatment, but he experienced recurrence of symptoms and was subsequently started on low-dose steroids and sulfasalazine (2015–2016). He remained asymptomatic for six months but later experienced a recurrence of symptoms with worsening left thigh pain and new sites of BME noted on MRI. Treatment included sulfasalazine, corticosteroids and weekly injections of etanercept (2016-2018). He remained asymptomatic, but symptoms recurred when etanercept was discontinued in 2022. Weekly injections of etanercept were restarted, and he remained asymptomatic until June 2024. This time, he presented with inflammatory low back pain, peripheral arthritis involving bilateral knees and chest wall enthesitis. Repeat MRI revealed worsening BME and bilateral sacroiliitis (Figure 2, panels A, B and C). A low-dose noncontrast computed tomography (NCCT) of the sacroiliac joints showed partial ankylosis bilaterally. Timeline of course of events is summarised in Figure 3.
MRI Images at the Onset of Disease (2015). Panel A: MRI STIR Images Showing BME at Multiple Sites. Panel B: Normal Sacroiliac Joint.
MRI and CT Images After 10 Years (2024): Panels A and B: BME at Multiple Sites. Panel C: Low-Dose NCCTSI Joint Showing Partial Ankylosis of Bilateral Sacroiliac Joint.
Course of the Disease Over 10 Years.
This case presents a diagnostic dilemma: Are we dealing with CNO, juvenile spondyloarthritis (ERA) or CNO progressing to SpA over a period of 10 years? Alternatively, could this be an association between the two entities? To find answers, we conducted a literature review.
Discussion
CNO is an autoinflammatory bone disorder. Familial autoinflammatory forms of CNO and their associated mutations are linked to interleukin-1β (IL-1β) dysregulation, while nonfamilial or sporadic forms are attributed to variable defects in the TLR4/MAPK/inflammasome signalling cascade, resulting in an imbalance between pro- and anti-inflammatory cytokine expression in monocytes.1,2
A large case series revealed that CNO can present with heterogeneous clinical manifestations, including mucocutaneous and musculoskeletal symptoms, a family history of autoimmune disease and HLA-B27 positivity in 8%-15% of cases. 3 ERA, a subtype of juvenile idiopathic arthritis (JIA), refers to a group of human leukocyte antigen (HLA)-B27-associated inflammatory disorders that primarily affect male patients over the age of six years. 4 Peripheral arthritis, predominantly involving the lower limbs and sacroiliitis are the major clinical manifestations.
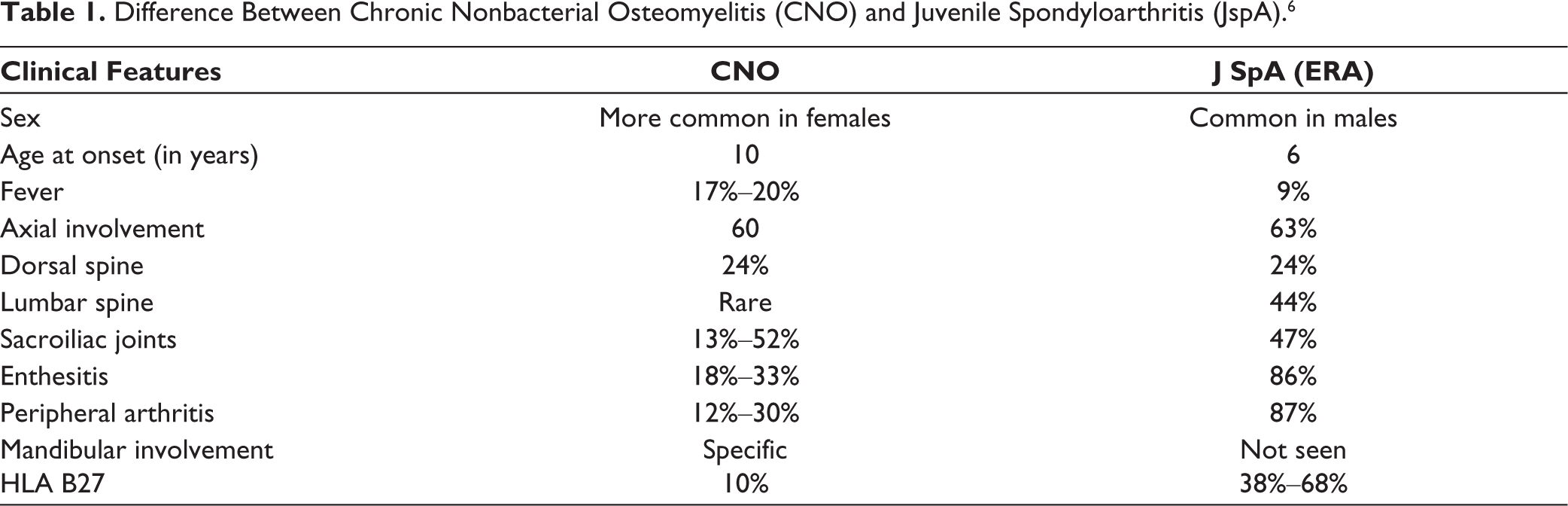
In a long-term retrospective study on the outcomes of CNO by Vittecoq et al., it was noted that 12 patients evolved into SpA over a period of 10 years. Interestingly, these patients differed from classical SpA, exhibiting unilateral sacroiliitis, no familial forms and no association with HLA-B27. 5 Notably, our patient developed bilateral sacroiliitis during the course of the illness. Many times, these two entities are difficult to differentiate. 4 The salient differences are mentioned in Table 1.
Difference Between Chronic Nonbacterial Osteomyelitis (CNO) and Juvenile Spondyloarthritis (JspA). 6
Our patient initially presented with typical features of CNO but gradually developed predominant features of SpA, including inflammatory low back pain, peripheral arthritis, enthesitis and sacroiliac joint ankylosis on imaging, over a period of 10 years. Unlike previous studies reporting CNO progression to SpA, our patient was HLA-B27 positive, had a family history of SpA and exhibited bilateral sacroiliitis on imaging. Studies suggest that intestinal dysbiosis may serve as a common potential trigger for these two diseases. 6
Conclusion
The overlapping clinical and radiological features of CNO and SpA posed a significant diagnostic challenge in our case. This case highlights the potential spectrum of CNO-SpA and the shared efficacy of anti-tumour necrosis factor-alpha (anti-TNF-α) agents and NSAIDs in their management. However, it is notable that IL-1 inhibitors, commonly used for treating CNO, are not effective in managing SpA. Further research is needed to better delineate the pathophysiological and therapeutic overlap between these two entities.
Footnotes
Data Availability Statement
All data relevant to the study are included in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written consent has been obtained from the patient for publication.