
Abstract

Introduction
Spondyloarthritis (SpA) can present with various extra-articular manifestations, involving eyes, bowel, heart, lungs, kidneys, skin and bones. Although renal involvement in SpA is uncommon, it can manifest as secondary renal amyloidosis (AA type), non-steroidal anti-inflammatory drug (NSAID) nephropathy, glomerulonephritis or IgA nephropathy.
Secondary amyloidosis is characterised by the extracellular deposition of amyloid A fibrils in various tissues and organs, caused by protein misfolding. This condition is a well-known complication associated with several chronic inflammatory diseases, such as rheumatoid arthritis (RA), SpA spectrum disorder like ankylosing spondylitis (AS), arthritis related to inflammatory bowel disease (IBD), reactive arthritis (ReA), psoriatic arthritis (PsA), enthesitis related arthritis (JIA ERA) and other autoinflammatory disorders. 1 The most common organ affected in secondary amyloidosis is the kidney, 2 although other organs may also be involved. The typical presentation of amyloidosis is nephrotic range proteinuria.
According to a longitudinal population-based cohort study by Kridin M et al., the incidence rate of amyloidosis in SpA is 2.15%, with 6.6-fold higher risk than the general population with a hazard ratio of 6.16. 3 Risk factors for developing secondary amyloidosis include older age, male sex, prolonged duration of the disease, uncontrolled disease activity, high inflammatory markers, delayed diagnosis and delayed initiation of therapy. Among the spectrum of SpA, amyloidosis is more frequently associated with arthritis related to IBD, followed by reactive arthritis, SpA and psoriatic arthritis. 4
The time between the diagnosis of SpA and the onset of amyloidosis can vary widely. However, studies suggest that long periods of uncontrolled disease can lead to AA amyloidosis, with one study indicating that as little as four years of disease duration may develop amyloidosis as a complication of SpA. 4
In this case series, we present four patients with SpA who were followed at a tertiary care centre and later developed renal amyloidosis. Written consent was obtained from all patients.
Key Message: Despite advancements in therapy, amyloidosis should be suspected in patients with SpA who present with proteinuria and oedema
Case 1
A 25-year-old male presented with a four-year history of pain over the left knee, bilateral ankles and buttocks. He had inflammatory back pain with early morning stiffness lasting about one hour and frequent nocturnal awakenings. He had no symptoms suggestive of IBD, psoriasis or uveitis, and his family history was not significant. For the past three months, he had experienced facial swelling accompanied by periorbital puffiness and bilateral lower limb swelling up to mid-calf. He denied having symptoms such as breathlessness, paroxysmal nocturnal dyspnoea, orthopnea, chest pain or oliguria. On examination, he had pallor, anasarca, periorbital puffiness, macroglossia (Figure 1A), nail dystrophy (Figure 1B) with thin and brittle nails. Laboratory investigations showed urea 46 mg/dL, creatinine 4.8 mg/dL and potassium 3.36 mg/dL. Urine analysis showed 800 mg of protein with no active urinary sediments, and a 24-hour urine collection for protein showed 12 g/day. Due to a rapid and persistent rise in creatinine levels and progressive anasarca, he was started on haemodialysis. Ultrasonography of the abdomen suggested mild hepatomegaly, normal kidney size, and attenuated corticomedullary differentiation. Renal biopsy showed weakly periodic acid-Schiff (PAS) positive mesangial deposits, no vessel proliferation, tubular atrophy and interstitial fibrosis (Figure 2A). Congo red staining demonstrated apple green birefringence under polarised light microscopy, and no deposits were found on immunofluorescence. Immunohistochemistry revealed positivity for amyloid AA (Figure 2B) and amyloid P, indicating secondary amyloidosis, with a primary diagnosis of AS. He was treated with infliximab (5 mg/kg) 8 weekly, with angiotensin-converting enzyme inhibitors (ACEI) and a high-protein diet. He was followed up every three months and significant proteinuria reduction to 5 g was achieved after 12 months.
(A) Macroglossia in a 25-Year-Old Patient With Spondyloarthritis With Systemic AA Amyloidosis. (B) Nail Dystrophy, Thin and Brittle Nails With Yellowish Discolouration in the Same Patient.

(A) Section From Renal Biopsy Shows Weakly PAS-Positive Deposits in Glomeruli (Asterisk) and Blood Vessels (Arrow) (Periodic Acid-Schiff, ×50). (B) Renal Biopsy With Apple Green Birefringence in Glomeruli (Asterisk) (Congo Red Stain With Polarisation, ×200). Upper and Lower Right Images Show Amyloid P and Amyloid AA Positivity, Respectively, in Glomeruli on Immunohistochemistry (Arrows) (Diaminobenzidine, ×200).

Case 2
Our second case is a 52-year-old male, who had a history of symmetrical small and large joint inflammatory polyarthritis of both upper and lower limbs and inflammatory back pain with early morning stiffness lasting for approximately two hours for the last 10 years. He had psoriatic skin lesions. His symptoms were partially controlled with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs). After four years, he noticed blood in his stool and significant weight loss. On colonoscopy, he had findings suggestive of IBD and on histopathology, ulcerative colitis was diagnosed. He was then started on adalimumab (anti-TNF). With this treatment, his arthritis and psoriasis went into remission. In July 2022, he suffered from a right intertrochanteric fracture which was fixed with surgical intervention. After surgery, he developed repeated infections at the implant site, and adalimumab was restarted after the resolution of the infection. After two months, he presented with pain in his right knee and right wrist, along with bilateral lower limb oedema. He was worked up for lower limb oedema and his 24-hour urine protein level was 7.9 grams per day. Serum protein electrophoresis showed hypoalbuminemia and hypogammaglobulinemia with an elevation in the alpha-2 region, while the kappa-lambda ratio was normal in the serum light chain assay. An abdominal fat pad biopsy was performed which turned out negative for amyloid. Subsequently, his renal biopsy was done, which revealed Congo red-positive acellular deposits with apple green birefringence around arterioles and capillaries, as well as in the walls of arterioles under polarised light microscopy. This finding was consistent with vascular renal amyloidosis (Figure 3), secondary to the primary diagnosis of psoriatic arthritis and IBD. He was then started on an angiotensin receptor blocker (ARB) and infliximab at a dosage of 5 mg/kg at weeks 0, 2 and 6, followed by every two months, along with supportive measures. There was a significant improvement in proteinuria to 2.7 g after 12 months of follow-up.
(A) Section From Renal Biopsy Shows Weakly PAS-Positive Deposits in Glomeruli and Blood Vessels (Periodic Acid-Schiff, ×40). (B) Congo Red-Positive Acellular Deposits With Apple Green Birefringence Around Arteriole and Capillaries and in the Wall of Arterioles on Polarised Light, Suggestive of Vascular Renal Amyloidosis.

Case 3
A 34-year-old male presented with a 13-year history of inflammatory back pain, neck pain and polyarthritis affecting both small and large joints with early morning stiffness lasting for one hour. Four months ago, he developed swelling over both lower limbs and face, which progressed to anasarca. He also gave a history of polyuria and frothy urine. For the past three months, he had erythematous, itchy, desquamative plaque-like lesions on the lower one-third of both legs, thighs, lower back and abdomen, as well as hyperpigmentation and yellowish discolouration of the nails. There is no history of uveitis, IBD or dactylitis, and no family history of any autoimmune diseases. He was diagnosed with psoriatic arthritis, with a Psoriasis Area and Severity Index (PASI) score of 4.6. Enthesitis was present at multiple thoracic spinous processes. MRI of the sacroiliac joint showed bilateral acute on chronic sacroiliitis and Anderson lesions at the L2, L3 and L4 vertebrae. A 24-hour urine protein test showed 8.2 g of protein, and urinalysis showed 3+ proteinuria, without active sediments. Due to the nephrotic range proteinuria, a renal biopsy was performed, which revealed amorphous eosinophilic, weakly PAS-positive material in the mesangium and capillary walls, accompanied by a Congo red-positive interstitial mononuclear inflammatory infiltrate, indicating secondary amyloidosis. Initially, he was managed with infliximab but changed to adalimumab after an inadequate response. Proteinuria was improved to 2.3 g after 12 months of follow-up.
Case 4
A 24-year-old male presented with a 14-year history of inflammatory back pain, and alternating buttock pain along with bilateral shoulder, elbow and knee pain. He had early morning stiffness lasting for two hours. He underwent right total hip replacement after 11 years of disease onset. There was no history of psoriasis, uveitis, dactylitis or IBD. Since November 2023, he experienced swelling over both lower limbs and face, which gradually worsened and eventually led to anasarca. He did not complain of decreased urine output, frothy urine or dyspnoea. His lab investigation showed a haemoglobin of 8.64 g/dl, creatinine 1.8 mg/dl, Serum protein and albumin levels were 5.7 g/dl and 2.6 g/dl, respectively. Urine examination showed 3+ albuminuria, with 24-hour urine protein excretion of 16 grams. Renal biopsy was done which revealed weakly PAS-positive material in the mesangium, mild tubular atrophy with acute interstitial nephritis, hypertensive changes and both amyloid P and amyloid AA positivity on immunohistochemistry, indicating secondary amyloidosis with a primary diagnosis of SpA. He was treated with adalimumab at a dose of 40 mg subcutaneously every two weeks, significantly reducing proteinuria to 7.6 g after 12 months of follow-up.
Discussion and Review
The incidence of renal involvement in SpA varies from 5.2% to 21%. 5 The most common histological finding is AA amyloidosis followed by CIN, IgA nephropathy, focal segmental glomerulosclerosis, membranous nephropathy and immune complex-mediated membranoproliferative glomerulonephritis (IC-MPGN). 6 Amyloidosis can be present in 6.1% of the SpA patients with a mean time of 14.4 ± 10 years from the diagnosis. 6 IBD is strongly associated with amyloidosis, followed by AS, PsA and ReA. 7 Risk factors for the development of amyloidosis are male gender, older age, high inflammatory marker, longer disease duration and uncontrolled disease activity. Pathogenesis involves a two-hit hypothesis. The first hit is amyloid nidus formation from a granulomatous inflammatory condition, and the second hit is serum amyloid A production from another inflammatory process. 7 Amyloidosis complicates the underlying condition. Five-year survival rates among untreated and treated patients are 27% and 93%. 8 Treatment of AA amyloidosis involves treating the underlying condition. The most common treatments nowadays are biological therapy (anti-TNF, anti-IL-1 and anti-IL-6R) depending on the primary disease.9-12 Because of the rarity of AA amyloidosis, there are no reliable data regarding the effectiveness of these treatments. 13 TNF inhibitors are the first-line therapy in SpA with AA amyloidosis but can increase the rate of infection. Baseline proteinuria, serum creatinine and disease duration are the important predictors of the treatment response. 14
No trial has proven the medium- and long-term efficacy of ACEI and ARB in AA amyloidosis. As amyloidosis patients are prone to hypotension, these drugs need to be used very carefully.15,16 Protein restriction, which is typically suggested for cases of chronic renal insufficiency, is not always applicable to renal amyloidosis. More than 1.2 g/d proteinuria can be maintained. Sodium should be restricted, and fluid restriction should be done only if hyponatraemia is present. Dialysis-dependent individuals with AA amyloidosis have a poor prognosis with average survival from 20 to 50 months. 14 Renal transplantation increases overall patient prognosis and survival; however, it remains lower than transplants for end-stage chronic renal failure caused by different aetiology. 14
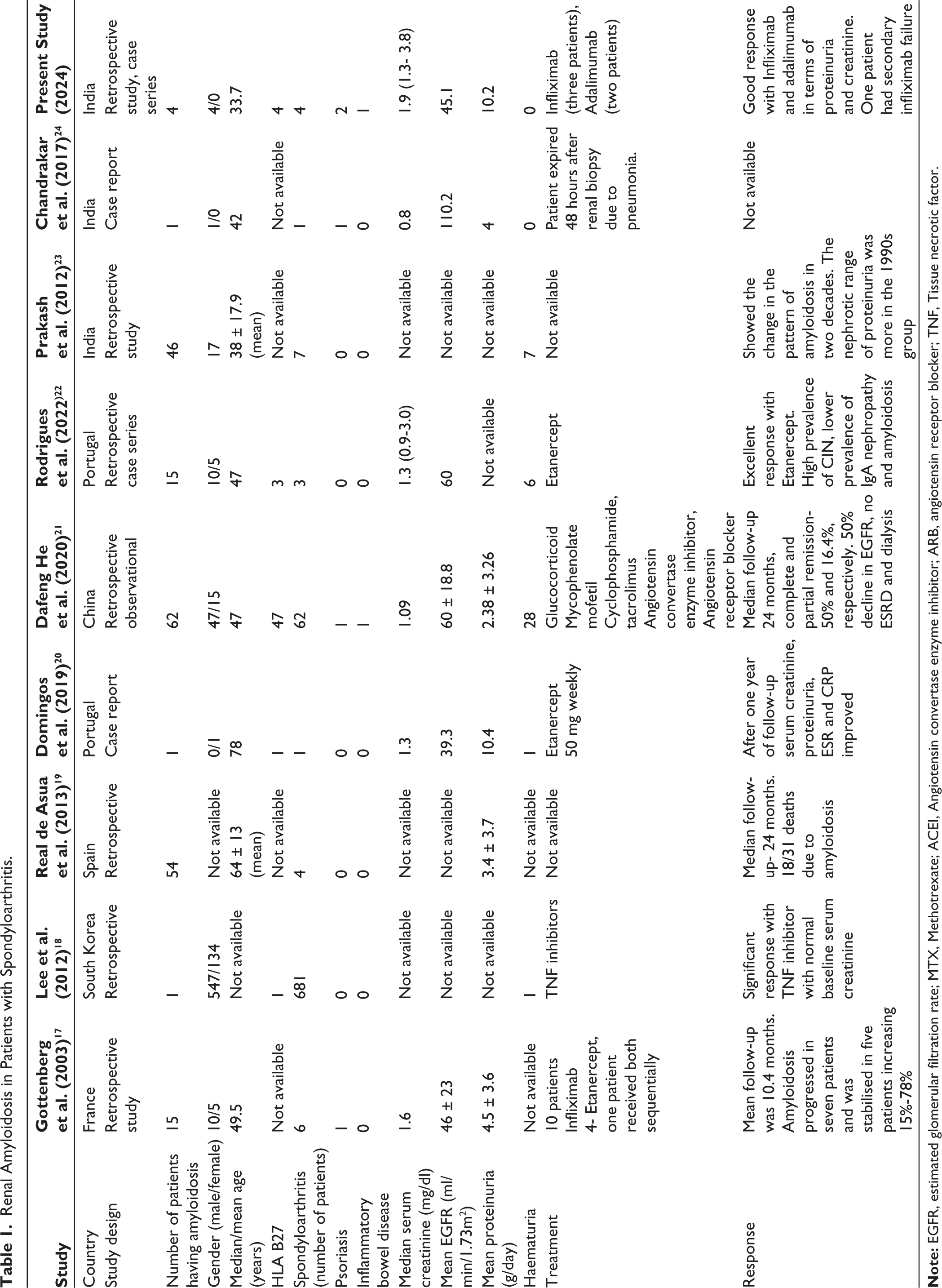
Gottenberg et al. studied retrospectively 15 patients with amyloidosis secondary to RA, AS, PsA and juvenile idiopathic arthritis. 17 Lee et al. found six patients with abnormal urine analysis, among whom only one case was diagnosed with renal amyloidosis among 681 patients with SpA. Both studies found that TNF inhibitors work better with baseline normal creatinine than abnormal creatinine.17,18 Real de Asua et al. from Spain, found 54 patients of AA amyloidosis in the SpA spectrum disorder with an average proteinuria of 3.4 g/day. 19 Domingos et al. from Portugal reported successful treatment with etanercept 50 mg weekly with a significant reduction in proteinuria and inflammatory markers in a 78-year-old female patient of SpA. 20 Dafeng He et al. did a retrospective observational study in 62 SpA patients with AA amyloidosis. They reported complete remission in 50% and partial remission in 16% of the patients with various immunosuppressive therapies like glucocorticoid, mycophenolate mofetil, cyclophosphamide and tacrolimus. 21 In a retrospective study, Rodrigues et al. found that 86% of SpA with AA amyloidosis patients had proteinuria and an excellent response with etanercept. 22
Urine analysis and 24-hour protein evaluation are the basic investigations to screen for amyloidosis. However, a definitive diagnosis of renal amyloidosis needs a biopsy with Congo red-positive amyloid fibrils with apple green birefringence in polarised light. Renal biopsies should only be performed if no other less invasive biopsy can detect amyloid deposits, such as accessory salivary gland biopsy or peri-umbilical fat pad biopsy. 9 Serum amyloid A protein can be detected by immunohistochemistry or serum samples.
In our case series of four patients, two patients had PsA out of which one had both PsA and IBD, and the rest two had AS. All of them were diagnosed to have secondary amyloidosis, and one of them had concurrent chronic interstitial nephritis (CIN). All were male and had high ESR as found in multiple studies shown in Table 1. All of the patients had high disease activity. 7 In this case series, the minimum disease duration of diagnosis of AA amyloidosis from the onset of primary disease was four years, although it is rare; the same finding was shown by Rodrigues AC et al. 22 and Prakash et al. 23 The younger age of onset in our study may be due to the underlying uncontrolled disease and the delayed initiation of the biological therapy because of the financial constraint. A similar finding was also seen in a study done by Chandrakar S from India. 24 All four patients had a nephrotic range of proteinuria, and one of them had deranged creatinine and is on maintenance haemodialysis. Most of the studies in Table 1 show mean proteinuria of ≥3 g/d. An Indian 2-decade case series from a single centre found a significant increase in the sub-nephrotic range of proteinuria and involvement of female patients from the 1990s to 2000s. All patients in our case series were on TNF inhibitors. The mean duration of follow-up on TNF inhibitors was around 12 months. All the patients had good responses in terms of proteinuria and creatinine after six months and 12 months of TNF inhibitors (Table 2). Previous studies have also shown better responses to TNF inhibitor therapy.17,18,20,22 The most common infections are respiratory and urinary tract infections. Due to neutropenia, they have a high risk of candidiasis. 25 In our study, the fourth patient had recurrent urinary tract infections following infliximab. Amyloidosis itself increases the risk of infection apart from other factors like poor hygiene and inadequate vaccinations. CIN as a renal manifestation of SpA can also be a possibility irrespective of medications used. 6
Renal Amyloidosis in Patients with Spondyloarthritis.
Investigations of the Present Case Series.

Our case series highlights that renal manifestations may occur before or concurrently with arthritis onset, emphasising the role of urine analysis in diagnosing amyloidosis in patients with SpA. However, the study has some limitations. First, a small sample size. Second, a causal association between chronic inflammatory nephritis (CIN) and SpA could not be found due to various drugs, genetic and environmental factors. Further prospective studies are needed to clarify the prevalence and associations of rare renal manifestations in SpA.
Footnotes
Abbreviations
AA, Amyloid A; FSGS, Focal segmental glomerulosclerosis; RA, Rheumatoid arthritis; SpA, Spondyloarthritis; AS, Ankylosing spondylitis; ReA, Reactive arthritis; PsA, Psoriatic arthritis; IBD, Inflammatory bowel disease; JIA, Juvenile idiopathic arthritis; PND, Paroxysmal nocturnal dyspnoea; CIN, Chronic interstitial nephropathy; CMD, Corticomedullary differentiation; NSAID, Non-steroidal anti-inflammatory drug; PAS, Periodic acid-Schiff; csDMARDs, Conventional synthetic disease-modifying antirheumatic drugs; TNFi, Tissue necrotic factor inhibitors.
Author Contributions
The conception and design of the study: RKS, DE, PP, PD, KK, UD, PK; acquisition of data, analysis and interpretation of data: RKS, DE, PD, KK, UD, PK. Drafting the article: RKS, DE, PD, KK, UD, PK; Revising it critically for important intellectual content: RKS, DE, PD, UD. Final approval of the version to be submitted: All authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: All authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Disclaimer
No part of this manuscript is copied or published elsewhere. No part of this study has been presented at any national or international conferences.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
An informed consent was obtained from the parent prior to the publication of any personal health information, ensuring adherence to ethical standards and patient confidentiality.