
Abstract

Dear Editor,
The temporomandibular joint (TMJ) is a synovial joint with a complex anatomy (Figure 1A) and unique joint biomechanics. 1 The complex biomechanics of the TMJ are maintained by articulating surfaces of the mandibular condylar with the temporal bone, intervening mobile articular discs and synovial lining along with surrounding ligaments and muscles. TMJ involvement is well-recognised in patients with rheumatoid arthritis (RA); however, managing chronic TMJ issues often requires cross-specialty collaboration with maxillofacial or dental surgeons. Consequently, rheumatologists often face gaps in their understanding of the natural history, imaging findings and optimal treatment strategies for TMJ issues in RA patients. Through the exploration of three cases, we aimed to highlight important aspects of TMJ management to enhance the care of patients with RA dealing with TMJ pathology (Table 1).
(A) Normal Temporomandibular Joint Anatomy (TMJ). (From Liebgott B: The Anatomical Basis of Dentistry, ed 3, Chapter 7, St. Louis, 2011, Mosby.) (B) MRI Showing Condylar Changes and Articular Disc Thinning Due to Synovitis. (C) Dynamic MRI of the Right TMJ Showing Medial Displacement of the Disc in the Closed-mouth Position. (D) Anterior Disc Displacement Observed in Closed-mouth Position. (E) Complete Reduction in Disc Displacement in the Open-mouth Position.

Clinical Characteristics and Imaging Findings of Three Patients with Rheumatoid Arthritis with Temporomandibular Pathology.
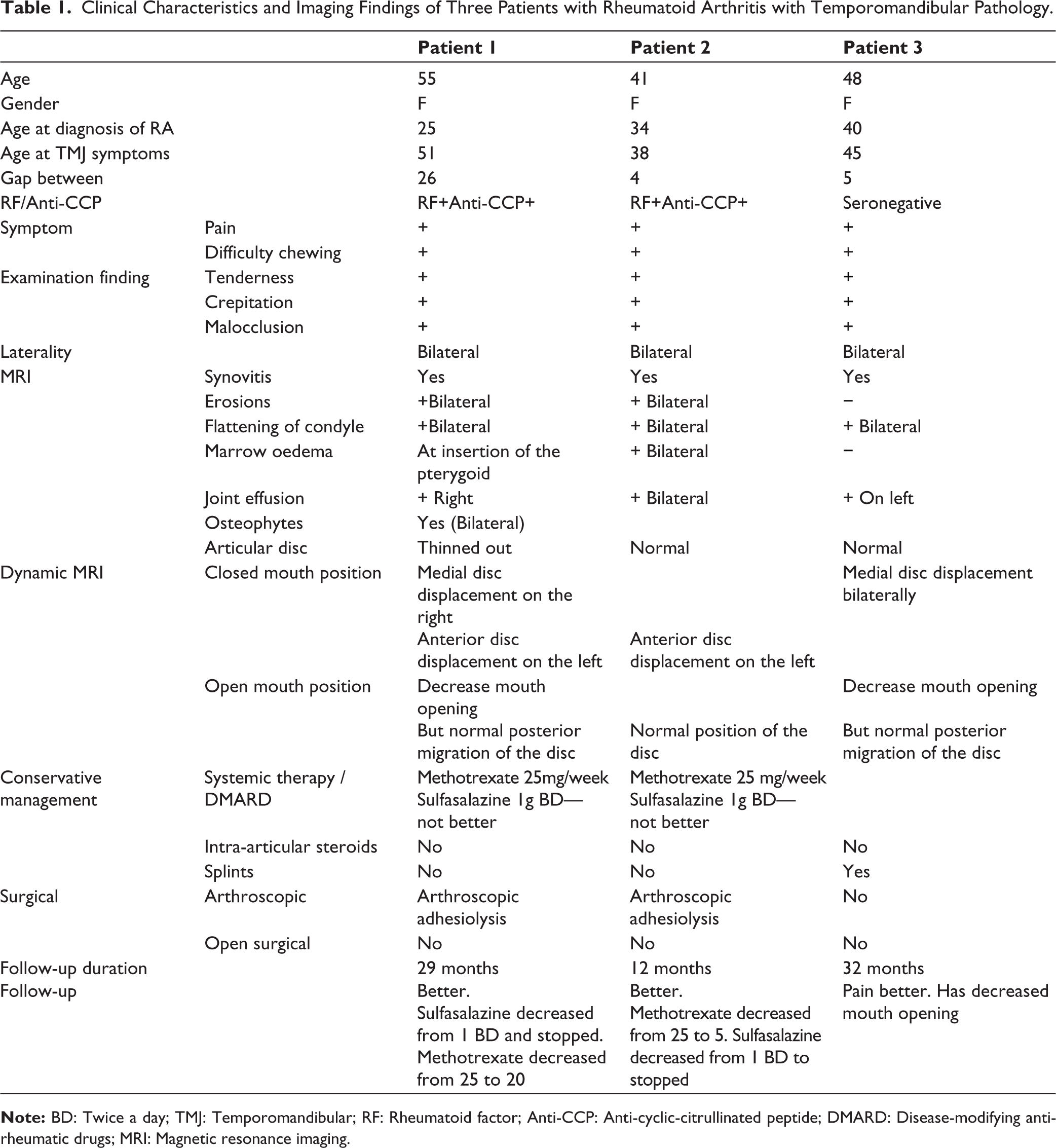
A 55-year-old woman with a 25-year history of seropositive RA, well-managed with disease-modifying antirheumatic drugs (DMARDs), presented with predominant right-sided TMJ pain. The pain was most noticeable during chewing and was accompanied by limited jaw opening, while other joints remained well controlled on her current DMARD regimen. Magnetic resonance imaging (MRI) revealed bilateral erosions and flattening of the condyloid process heads with associated sclerosis of the articular surfaces as well as thinning and degeneration of the intervening articular discs (Figure 1B). Additional findings included anterior disc displacement with a reduction in the articular disc space on the left side and mild medial displacement of the disc on the right side. Initially, TMJ pain was treated as a manifestation of active RA with escalation of DMARD therapy, including methotrexate (MTX) and sulfasalazine (SSA), for over two years. However, the patient responded inadequately to systemic therapy. A TMJ specialist’s opinion was sought, and the possibility of biomechanical dysfunction, rather than active arthritis, was considered the primary cause of TMJ symptoms. Subsequently, arthroscopic adhesiolysis was performed, and intra-articular hyaluronic acid was injected. This intervention led to significant pain reduction, improved TMJ function, and allowed tapering of the DMARDs. At the 29-month follow-up, the patient demonstrated sustained improvement with MTX 15 mg/week. This case highlights the importance of recognising the biomechanical contributions to TMJ symptoms in RA and underscores the efficacy of surgical interventions in conjunction with systemic therapy, particularly in cases refractory to conservative management.
Patient 2, a 41-year-old female patient with RA for the last four years, presented with left jaw pain and chewing difficulties. Although her peripheral joint symptoms were well controlled with MTX and SSA, TMJ symptoms significantly affected her quality of life. Dynamic MRI revealed mild contour irregularities, flattening of the condylar heads, small cortical erosions, marrow oedema and mild bilateral TMJ effusion with anterior displacement of the left TMJ disc in the closed-mouth position. Arthroscopic adhesiolysis surgery effectively relieved the symptoms and restored TMJ mobility, leading to a substantial improvement in oral function. DMARDs were gradually tapered, SSA was discontinued and the patient was well maintained on MTX monotherapy.
Patient 3, a 48-year-old female RA since the last three years, presented with left TMJ pain and malocclusions. Though her peripheral joint symptoms were well controlled on DMARDS, she continued to have issues with chewing and mouth closure. MRI confirmed synovitis, erosions and joint effusion with bilateral medial disc displacement in the closed-mouth position (Figure 1C-E). She chose against surgical management and was managed conservatively with splints. At 32-month follow-up, her pain had improved, but she still faced issues with mouth closure and chewing.
These three cases demonstrate typical clinical scenarios, MRI findings and treatment modalities and outcomes in patients with RA with TMJ involvement.
There is significant variability in reporting the prevalence of TMJ involvement in RA, with studies suggesting a prevalence of approximately 10% at disease onset, 2 and between 20% and 60% in long-standing RA patients.2-7 Women aged 35-45 are three to five times more prone to TMJ issues than men, 8 likely due to hormonal influences and stress. Oestrogen receptors in women’s TMJ may impact ligament laxity, potentially leading to TMJ involvement and heightened pain sensitivity. 9
Active synovitis with effusion of the TMJ joint may cause pain and decrease mouth opening, with early morning stiffness and decreased masticatory force. However, long-standing disease may cause erosion and flattening of the mandibular condyle, with articular disc thinning. This may lead to altered joint mechanics and malocclusion with pain during chewing. This can typically be observed on MRI, as seen in all three patients. In addition, chronic changes in the TMJ joint may lead to articular disc instability with adhesions, leading to a typical popping sensation during jaw movement and may lead to chronic malocclusion.
Various imaging techniques are available for assessing TMJ involvement in RA. The incidence of TMJ changes on conventional radiographs ranges from 19% to 86%, and they correlate with the severity and duration of RA.10,11 Computed tomography (CT) or cone-beam computed tomography (CBCT) may be considered alternatives in some cases but are unsuitable for early-stage arthritis assessment. 12 Ultrasound is currently not recommended for TMJ arthritis evaluation due to standardisation issues and limited evidence. 13 MRI is the preferred method to visualise synovitis and bone marrow oedema. 14 Additionally, dynamic MRI scans, conducted with both closed and open mouth positions, are recommended for evaluating articular disc conditions, particularly in cases involving locking and malocclusion. 15 Typical MRI findings were seen in all our three patients. Some, MRI features can help differentiate RA from other inflammatory arthritis with TMJ involvement. RA typically shows symmetric erosions, synovitis and disc degeneration, whereas SpA is characterised by asymmetric involvement, osteoproliferation, ankylosis and enthesopathy. Similarly, juvenile idiopathic arthritis (JIA) often presents with condylar hypoplasia, flattening and growth abnormalities and retrognathia due to early joint damage. 16
The treatment of TMJ involvement in RA follows a hierarchical approach, starting with conservative management and escalating to more invasive interventions based on symptoms and MRI findings. Initially, pharmacotherapy with nonsteroidal anti-inflammatory drugs (NSAIDs) and DMARDs targeted the underlying disease. However, in cases where chronic erosive changes occur leading to altered joint mechanics and potential secondary osteoarthritis, conservative approaches may be insufficient. Physical therapy and occlusive splints can offer relief from symptoms, but may not always improve jaw function. 17 Injections of corticosteroids or hyaluronic acid into the TMJ can provide subjective symptom relief and improve function.
If conservative management fails to alleviate symptoms, arthroscopic lysis and lavage may be performed to remove adhesions and debris from the joint space. In some cases, open surgical techniques including synovectomy and disc repositioning may be considered. These interventions aim to temporarily reduce pain, improve TMJ function and facilitate further diagnostic evaluation if necessary.18-20
Ultimately, open surgery involving discectomy, with or without replacement using alloplastic or autogenous materials, may be performed. However, the response to surgery can vary, and complications such as foreign body reactions to allografts may occur.21-24
In conclusion, TMJ involvement in RA poses complex challenges and often requires a multidisciplinary approach for its effective management. The presented cases illustrate diverse clinical scenarios, MRI findings and treatment outcomes. Pharmacotherapy, physical therapy and intra-articular injections offer relief, while arthroscopic and open surgical interventions are reserved for refractory cases. While surgical outcomes vary, understanding the hierarchical treatment approach and further research are crucial for optimising patient care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.