
Abstract
Background and Objectives:
Interstitial lung disease (ILD) is a common manifestation of connective tissue disease (CTD). (a) Pulmonary rehabilitation (PR) can be utilised to improve dyspnoea and quality of life in patients with chronic lung conditions, including both obstructive and restrictive lung diseases. (b) This study aims to determine if PR can be a useful therapy to improve functional capacity and self-reported measures of dyspnoea in patients with CTD-ILD.
Methods:
Patients with a diagnosis of CTD-ILD at a tertiary centre were prospectively enrolled to receive PR in this study. The primary outcome was a change in the 6-minute walk test (6MWT) between baseline and 8 weeks after PR. The secondary outcome measures included pulmonary function tests (PFTs) and Patient-Reported Outcomes Measurement Information System (PROMIS→) Dyspnoea, St George’s Respiratory Questionnaire (SGRQ), and Leicester Cough Questionnaire (LCQ), which were collected before and at 8 weeks after PR. P < .05 was considered statistically significant.
Results:
Twenty-one patients were included in the data analysis. The baseline characteristics are shown in Table 1. Following PR, there was a statistically significant improvement in the 6MWT (Figure 1). Improvement in scores was observed in LCQ and the symptom domain of the SGRQ. Trends towards improvement were noted in PROMIS→ Dyspnoea scores.
Conclusion:
In CTD-ILD patients, an 8-week course of PR led to improvements in functional capacity (6MWT) and certain quality of life domains (LCQ and symptom domain of SGRQ). Future studies are required to determine the longer-term benefit of PR in CTD-ILD patients and if these improvements are sustained.
Keywords
Introduction
Interstitial lung disease (ILD) is a common manifestation of connective tissue disease (CTD). ILD varies in prevalence and severity depending on the underlying CTD type. 3 Clinically significant associated ILD is estimated to affect about 10% of patients with rheumatoid arthritis (RA). Patients with RA-ILD have a poor prognosis, and ILD is one of the leading causes of death in RA.4,5 ILD affects approximately 35%-52% of patients with systemic sclerosis (SSc). 6 While some of the symptoms of CTD-associated ILDs may appear similar to idiopathic pulmonary fibrosis (IPF), different factors contribute to the prognosis of CTD-ILD. In patients with CTD-ILD, lung involvement can progress at varying degrees, while in IPF, lung involvement progresses rapidly. Due to a better prognosis, patients with CTD-ILD may tend to have better outcomes than patients with IPF with the same level of lung involvement. 7 Other manifestations of CTD that are not present in IPF can impact the prognosis, such as pulmonary arterial hypertension or restriction of the lungs due to extra-pulmonary factors like skin thickening around the torso or respiratory muscle inflammation. 8
Patients with CTD-ILD may notice increased difficulty with activities of daily living before they notice increased dyspnoea on exertion. The fibrosis that develops as the disease worsens is irreversible, and the patient’s health-related quality of life (HRQoL) can be adversely affected. Pulmonary rehabilitation (PR) is a programme consisting of exercises and educational sessions that aim to improve dyspnoea severity, exercise capacity and quality of life for patients. Commonly used as the standard of care in patients with chronic obstructive pulmonary disease (COPD), there is growing support for the use of PR in ILD.9,10 Patients’ degree of exercise limitation is inversely related to HRQoL. 11 Within the limitations of the ILD and symptomatic dyspnoea, the goal of PR is to increase exercise capacity with improvement in the HRQoL to some extent.
Previous studies have supported the utilisation of PR to show improvements in 6-minute walk distance (6MWD) and patient-reported outcomes (PROs), such as emotional and physical function in IPF and COPD, but very few address the potential outcomes of PR in CTD-ILD.12-14 In a randomised controlled study evaluating PR in 142 participants with ILD, 23 had CTD-ILD. Some participants continued with their standard of care, and others participated in 8 weeks of supervised exercise. CTD-ILD participants in the supervised exercise arm demonstrated a significant increase in the 6MWD between baseline and immediately after the completion of the 8-week exercise programme compared to the control group. 14
We hypothesised that a treatment course of PR in patients with CTD-ILD would lead to improvements in exercise capacity, as measured by 6MWD, and PRO measures of dyspnoea and generic health.
Methods
In this prospective, uncontrolled, observational study, we hypothesised that a treatment course of PR in patients with CTD-ILD would lead to improvements in exercise capacity, as measured by 6MWD, and PRO measures of dyspnoea and generic health. The primary outcome measure was an improvement in 6MWD. Secondary outcome measures were a change in the measure of dyspnoea as measured by the St George Respiratory Questionnaire (SGRQ), a change in HRQoL based on responses to patient-reported outcomes measurement information system (PROMIS) 29-item health profile, a change in the PRO measures of chronic cough using Leicester Cough Questionnaire (LCQ), and change in pulmonary function test (PFT) parameters: % predicted forced vital capacity (FVC) and % predicted diffusing capacity of the Lungs for Carbon Monoxide (DLCO) measured at week 8.
Patients with CTD-ILD, confirmed by high-resolution computed tomography of the chest, were identified at the University of Michigan Rheumatology clinics during standard-of-care visits from 2018 to 2020. Those deemed appropriate for PR were considered for participation in this study. This study was approved by the University of Michigan Institutional Review Board (HUM00146223) on 19 June 2018, and all subjects were consented prior to enrolment. Data collection occurred for 2 years, from July 2018 to June 2020.
Study Population
Participants needed to have rheumatologist confirmed CTD-ILD, abnormal PFTs with either FVC <80% or DLCO <80%, and a Grade-2 on the Magnitude of Task component of the Mahler Modified Dyspnoea Index, which indicates that the patient would become short of breath with moderate or average tasks such as walking up a gradual hill, climbing less than three flights of stairs, or carrying a light load on a level surface. All subjects were over the age of 18. Patients with clinically significant resting pulmonary hypertension, uncontrolled congestive heart failure, unstable ischaemic heart disease, severe peripheral vascular disease, serious concomitant illnesses that might compromise subject participation in rehabilitation, or medical conditions such as a lower extremity amputation that might affect PR or 6-minute walk tests (6MWTs) were excluded.
PR Programme
Participants attended a supervised outpatient PR programme either at the University of Michigan or a local hospital closer to their home. The PR programme was a comprehensive rehabilitation programme involving a small group of participants (6-8) that met three times weekly to engage in monitored exercise and educational sessions for a total of 8 weeks. Group exercises consisted of training under specified conditions including the same equipment, duration, and intensity measured by the Borg dyspnoea score. Exercises included a combination of aerobic exercise (such as cycling and walking) and upper and lower limb resistance training. Heart rate, oxygen saturation, perceived dyspnoea and perceived exertion were monitored throughout the exercises. Supplemental oxygen was provided during training if necessary. Educational sessions covered disease management strategies, symptom control, breathing exercises and the use of oxygen.
Outcome Measurements
Patients enrolled in this observational study completed PRO questionnaires, PFTs, and 6MWTs at baseline before starting PR and after completion, at 8 weeks. Surveys used to measure the impact of disease, HRQoL, and general well-being included the SGRQ, PROMIS→-29 short form, PROMIS→ dyspnoea functional limitations, PROMIS→ dyspnoea severity, PROMIS→ dyspnoea characteristics, and LCQ.
Statistical Methods
We reported mean and standard deviation for efficacy measurements at baseline and week 8, including % predicted FVC, % predicted DLCO, resting oxygen saturation (SaO2), lowest SaO2, LCQ, SGRQ, PROMIS→-29 questionnaire, and PROMIS→ dyspnoea questionnaire. Change from baseline to week 8 was calculated for each of the aforementioned measures. Wilcoxon signed-rank tests were conducted to see if the changes were significant. For each efficacy measurement, we plotted a spaghetti plot from baseline to week 8, with a line of mean, to show the changing trend. We also drew a histogram of change values with a Kernel curve to show the distribution of change. A significance level of 0.05 was used for all tests. All statistical analyses were performed in SAS (version 9.4), and figures were created in RStudio (version 4.2.2).
Results
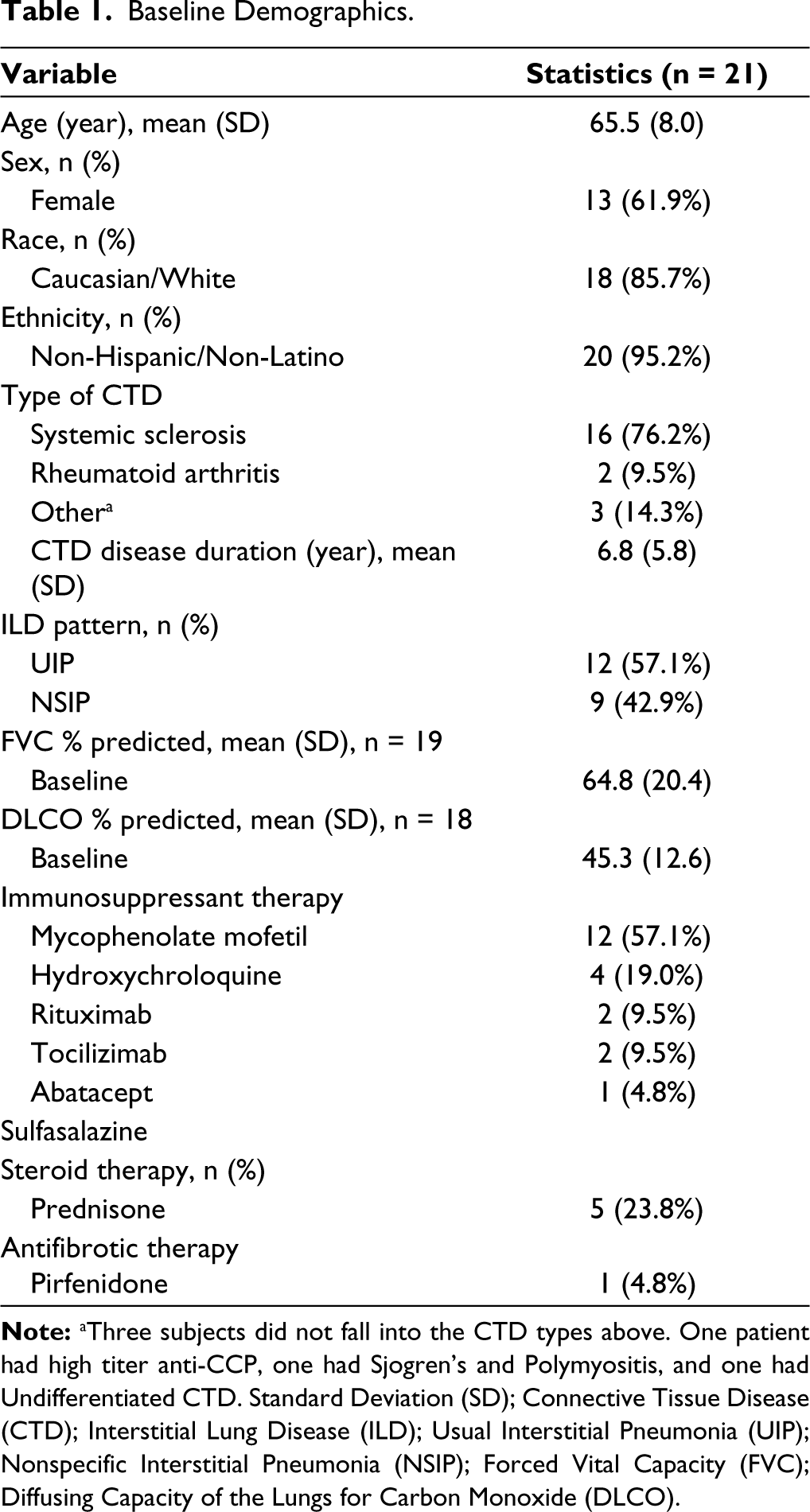
Of the 39 patients enrolled, 18 were excluded due to logistical constraints (n = 8), lost to follow-up (n = 9), and PR was not aggressive enough per participant feedback (n = 1). The remaining 21 patients were included in the data analysis. Baseline demographics are shown in Table 1. The mean age at the time of consent was 65.36 years; Majority of the participants were females (62%) and of Caucasian ethnicity (85.7%). Most participants (76.2%) enrolled in the study had systemic sclerosis-related ILD (SSc-ILD).
Baseline Demographics.
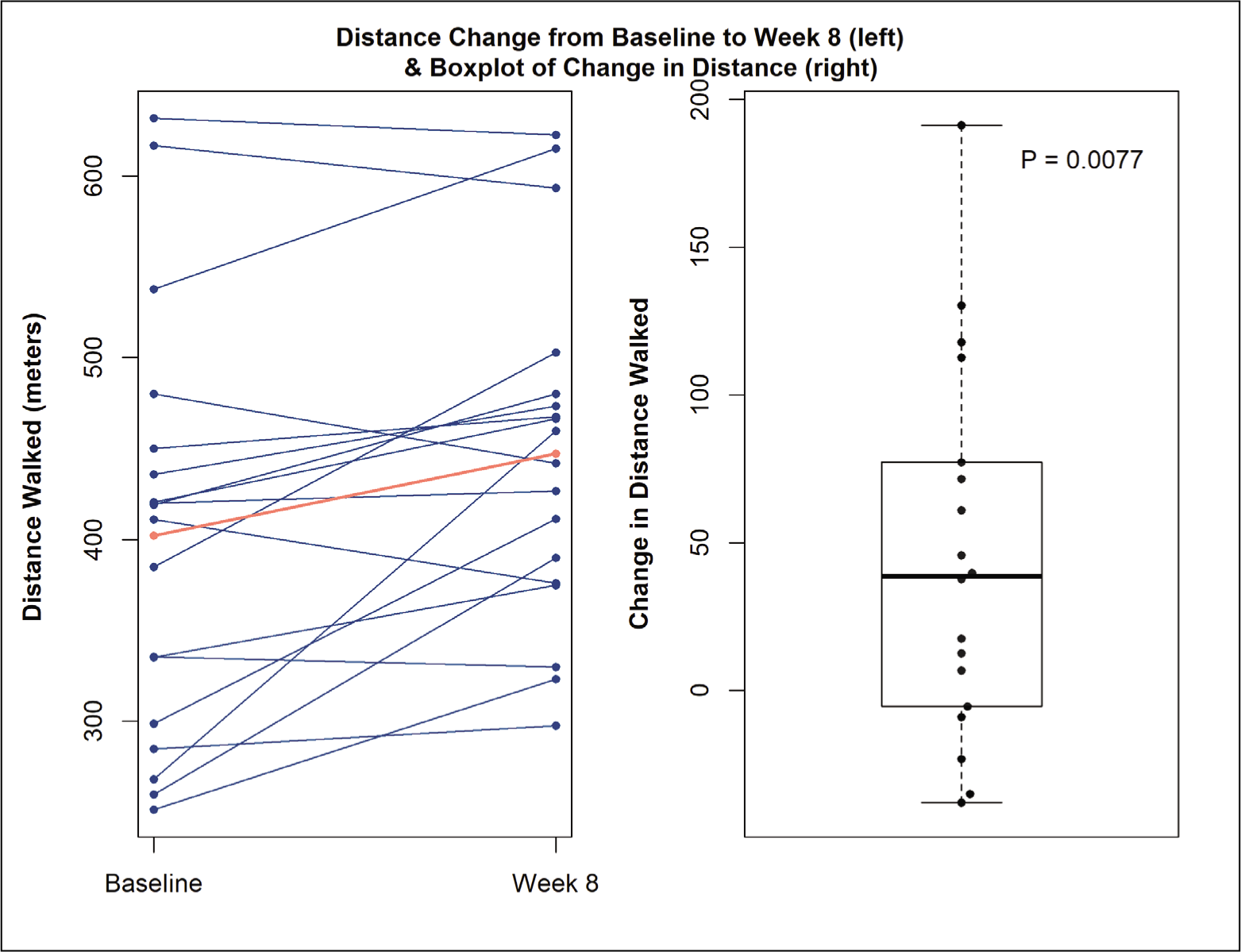
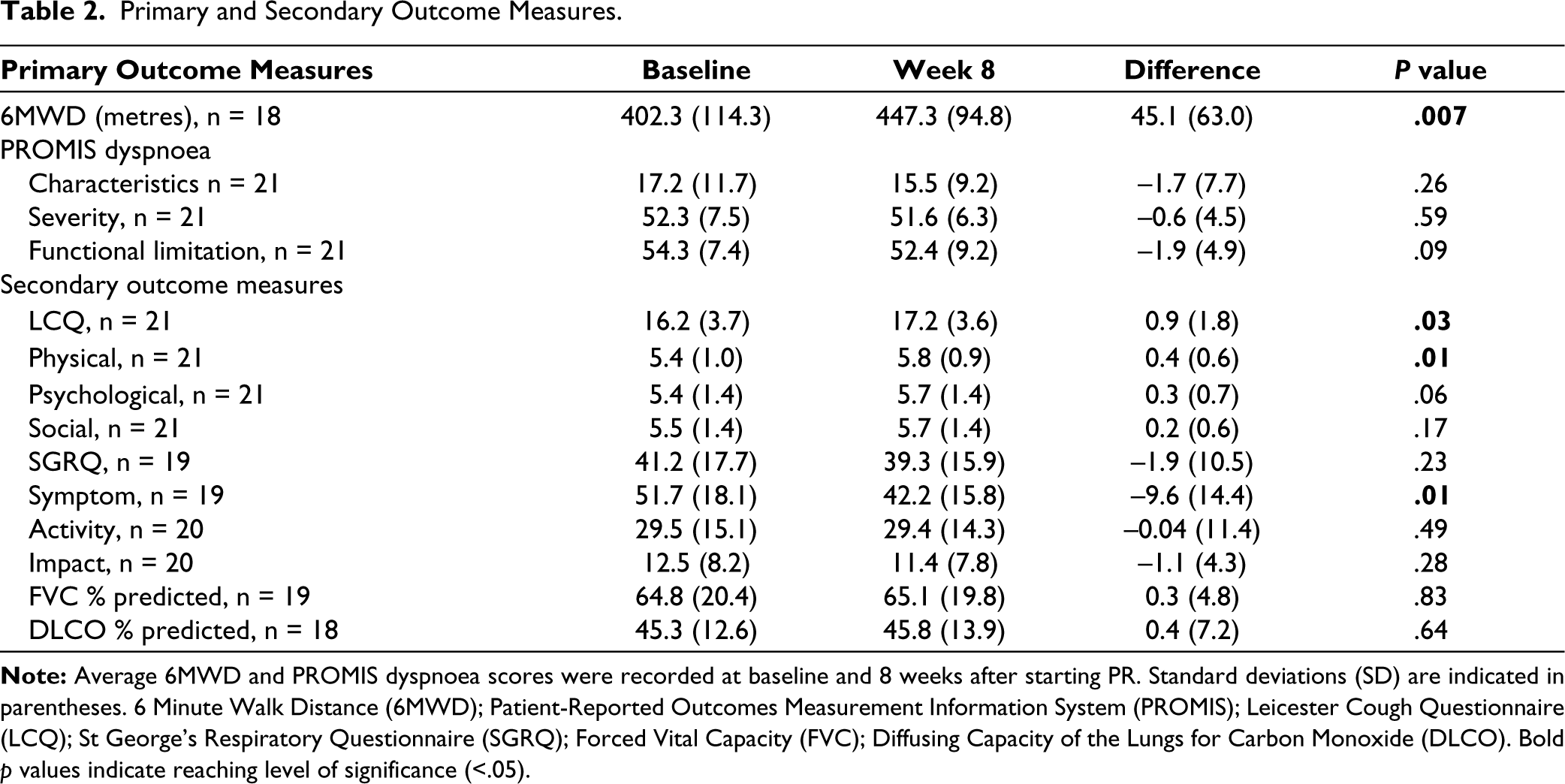
In comparing the primary outcome measure at baseline and week-8 there was a statistically significant improvement in the 6MWD of 45.1 m (mean at baseline 402.3 m, mean at 8 weeks 447.3 m, P = .007, Figure 1). See Table 2 for the results of the primary and secondary outcome measures. A small, non-significant increase in the lowest pulse oxygen saturation of 1.4% on average during the 6MWD was observed between baseline and week 8. No significant differences were seen in DLCO and FVC between week 0 and week 8.
Change in 6-minute Walk Test.
On the LCQ, where an increase in score indicates improvement, there was a significant 0.9-point increase in the average score between baseline and 8 weeks. Significant improvement was seen in the physical domain of the LCQ, with modest, non-significant improvements in the psychological and social domains. On the SGRQ questionnaire, where a decrease in score indicates improvement, there was a significant decrease in score in the symptom domain of the assessment by 9.4 points on average. Surprisingly, no significant differences were observed in reported physician function on the PROMIS→ dyspnoea questionnaire between baseline and 8 weeks. As expected, significant Spearman correlations were observed in LCQ and SQRQ-Symptom scores and other surveys, since questions target similar domains.
Discussion
In this single-centre study of patients with CTD-ILD, an 8-week course of PR led to improvements in 6MWD (a measure of functional capacity), LCQ scores, and the symptom domain of SGRQ. We saw no significant changes in HRQoL indicated by PROMIS→ questionnaires. The study met the intended primary outcome of statistically significant improvement in 6MWD. There is a possibility of a ceiling effect in the 6MWD since some of the participants were able to walk the predicted distance even at week 0. SGRQ is designed to measure the impact on overall health, daily life and perceived well-being in patients with chronic lung diseases and has been validated in CTD-ILD as a key outcome measure. 15 LCQ is the most widely used of all cough-specific PRO measures in ILD clinical trials. 15 While 6MWD increased throughout PR, a small, group-level non-significant increase in FVC and DLCO was noted (Table 2: Absolute difference in the means for FVC% predicted 0.3 and DLCO% predicted 0.4). The increase in 6MWD after PR in this study validates the results in the sub-set of CTD-ILD patients produced by Dowman et al. 14 It reaffirms the potential for PR as an effective therapy for patients with CTD-ILD, and specifically SSc-ILD. This reaffirmation of PR efficacy in CTD-ILDs is novel to this study, given that the progression of ILD types can vary and other studies do not focus on CTD-related ILDs alone.
Primary and Secondary Outcome Measures.
In another study, patients with ILD experienced the benefits of PR, regardless of disease severity, compared to patients with IPF who require treatment earlier in the disease for PR to be effective. Of the 44 subjects with ILD in a study, only three had concurrent diagnoses of CTD. 16 Future studies in CTD-ILD should seek to validate that patients with CTD-ILD will experience benefits regardless of disease severity, determine how long these benefits of PR last in CTD-ILD patients, and to what extent continuity of PR is required to maintain these benefits.
The study does have some limitations to consider. This was an uncontrolled, observational study. PR was conducted as part of the standard of care. Patients were not limited to a specific centre for PR due to logistical constraints. This can lead to slight differences in protocols and schedules for PR programmes that patients participate in. However, it was important to allow flexibility in the choice of PR site for convenience and compliance purposes. The American Thoracic Society/European Respiratory Society defined PR in 2013 as
a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies that include, but are not limited to, exercise training, education, and behaviour change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence to health enhancing behaviors.
17
A recent publication in 2021 from the American Thoracic Society acknowledges that it is a very conceptual definition. 18 This study was designed to evaluate the potential benefits of PR in a real-world experience prioritising patient convenience and adherence to the protocols as long as the PR protocols satisfied the conceptual definition.
Long-term monitoring of patients following PR was not recorded as part of this study, so we cannot determine how long patients benefited from PR and whether patients were compliant with PR. Some skew toward participants in the study having SSc may be due to the high prevalence of ILD in SSc. The University of Michigan has a large Scleroderma Programme which may also contribute to the high representation of SSc in this study.
The sample size for this study was limited due to the constraints of COVID-19. When evaluating the significance of results, we utilised a confidence interval of 95%, leaving the potential for 1 in 20 results listed as significantly significant to be false positives. P values for measures outside primary and secondary outcomes were not adjusted for multiple testing as they are exploratory. Patients from this study were followed by the University of Michigan Rheumatology, allowing for procedures such as 6MWT or PFT to be locally completed at the University of Michigan for most subjects.
Future studies would benefit from a larger cohort and a control group or observer-blinded case-control study consisting of patients with CTD-ILD and the inclusion of COPD and IPF patients as comparators. Additional studies may consider utilising a standardised PR protocol for all participants. A longer follow-up should be conducted to determine the longer-term benefits of PR, compliance with the protocol, and whether there was a continuation of the at-home exercises after discontinuing PR. PROs should be collected both during PR and following discontinuation. It will be important to collect additional 6MWT in future studies to monitor 6MWD in the longer term. Additional confounding factors that should be controlled for in future studies include modified Rodnan Skin Score in patients with SSc, myopathy in patients with myositis, presence of contractures due to severe skin and joint disease, and other non-pulmonary symptoms that may impact physical function and hence, PRO and 6MWT measurements. Additional studies should also consider the use of activity monitors, to track how activity at home is affected by PR, which may in turn affect functional capacity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the University of Michigan Institutional Review Board (HUM00146223) on 19 June 2018 and all subjects were consented prior to enrolment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases K24 AR063120-10, to Dr Dinesh Khanna.
Informed Consent
Written informed consent was obtained for anonymized patient information to be published in this article.