
Abstract

Dear Editor,
Endocrine disorders, through their metabolic effect, cause bone and joint pathology resulting in the first presentation to a rheumatologist. Parathyroid disorders frequently present with joint pain and muscle weakness which may mask the underlying endocrine disorder. Recognising the interplay between endocrine disorders and rheumatic symptoms is crucial for accurate diagnosis and effective treatment.
Parathyroid hormone (PTH), a key regulator of calcium metabolism maintains optimal calcium levels in the blood. It promotes calcium release from bones, increases calcium absorption in the gut by increasing 1,25 dihydroxy vitamin D levels, and increases calcium reabsorption by the kidneys. It also maintains phosphate balance by reducing renal tubular reabsorption of phosphate. 1 Therefore, abnormalities in PTH, such as hypoparathyroidism (HoPT) and hyperparathyroidism (HyPT) lead to calcium and phosphate imbalances causing musculoskeletal symptoms.
PTH also promotes bone remodelling with direct effects on osteoblast and osteocyte and indirect effects on osteoclast. In HoPT, reduced remodelling leads to calcium deposition in the bones resulting in increased bone density. This can present with features mimicking Spondylarthritis (SpA) or Diffuse Idiopathic Skeletal Hyperostosis (DISH).2,3 Soft tissue calcifications in the basal ganglia, shoulder joints, cataracts, or subcutaneous tissue of the hands can be seen, but are usually asymptomatic. HoPT can also cause tetany and muscle weakness due to hypocalcaemia. 4
HyPT may present as asymptomatic mild hypercalcaemia, symptomatic hypercalcaemia with renal stones, or very high calcium levels with musculoskeletal features. Annual health check-ups result in early detection of hypercalcaemia making advanced bone changes uncommon. Classical features include subperiosteal bone resorption most commonly seen on the radial aspect of proximal and middle phalanx of the second and third finger; subchondral bone resorption, osteitis fibrosa cystica with brown tumours and pepper pot skull (diffuse lytic foci interspersed between regular bone).5,6 Generalised osteopenia with an increased risk of fragility fractures is a major concern. 7
Osteomalacia (OM) is a metabolic bone disease characterised by defective mineralisation of the osteoid matrix leading to soft weak bones in adults. The primary cause is vitamin D deficiency leading to impaired calcium and phosphate absorption. However, several genetic as well as acquired causes are also known. 8 Clinical manifestations can range from diffuse ache, bony pain, proximal muscle weakness, fragility fracture and deformities. 9 Subtle initial manifestations can lead to a delay in diagnosis. OM may cause inflammatory spinal pain and clinicians are likely to miss OM and treat for axial SpA instead. 10
Clinical Case 1
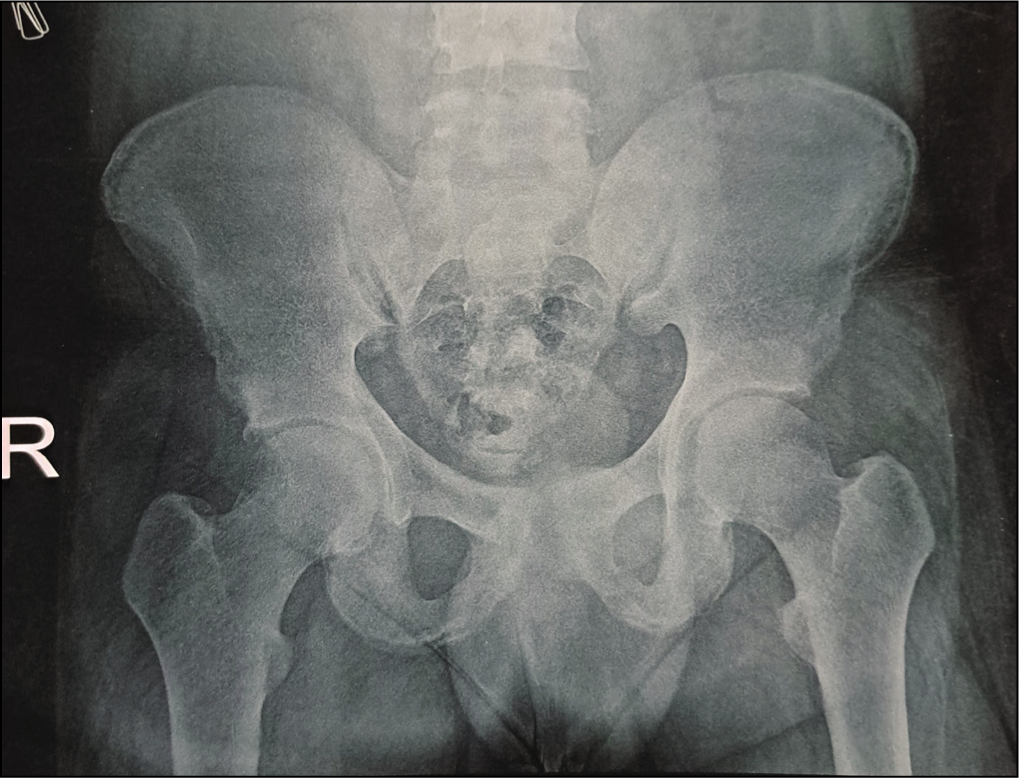
A 21-year-old man presented with progressive lower back pain and early morning stiffness lasting for 30 minutes over 4 years. This was unresponsive to non-steroidal anti-inflammatory drugs (NSAIDs). It was also associated with right hip pain and difficulty sitting cross-legged for 3 years with no signs of peripheral arthritis or extra-articular manifestations like uveitis, colitis and psoriasis. Examination revealed restricted spinal mobility, with a painful range of motion in the right hip. X-ray pelvis showed bilateral acetabular sclerosis with unremarkable sacroiliac (SI) joints (Figure 1). MRI of the SI joints revealed bone marrow oedema bilaterally with few erosions suggestive of active sacroiliitis. His HLA-B27 and CRP were negative. The patient was diagnosed with SpA and started on Tofacitinib, which he took for 6 months but had no relief.
The patient then presented to our centre for a second opinion. On investigation, the serum calcium was found to be very low <5.3 mg/dl (8.5–10.5 mg/dl), serum phosphorus was high 18.9 mg/dl (2.5–4.5mg/dl), serum creatinine was 0.84 mg/dl, and serum intact PTH (iPTH) was also low 5.51 pg/ml (17.3–74.1 pg/ml); diagnostic of primary HoPT. The patient was started on daily teriparatide injection 20 µg, high dose calcium (calcium carbonate 1 gram twice daily) and active vitamin D3 (Oral Calcitriol 0.25 µg twice daily). Within 6 months patients had significant improvement in their symptoms with normalisation of serum calcium and phosphate levels.
X-ray Pelvis with Hips Showing Bilateral Acetabular Sclerosis with Clear SI Joints.
Clinical Case 2
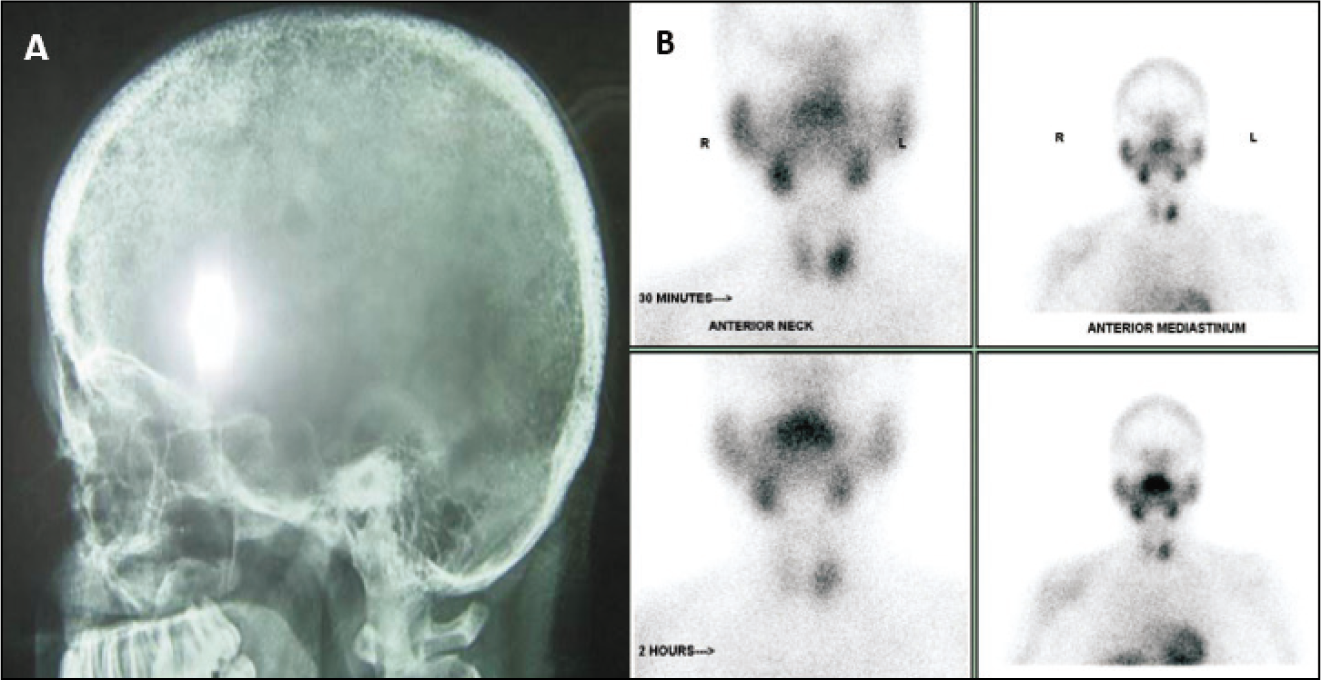
A 24-year-old woman presented with generalised bony and muscular pain for 1 year limiting her daily activities. This was followed by sudden onset vision loss in left eye. CT Brain showed a mass lesion in the ethmoidal sinus compressing the optic nerve. FNAC of the lesion showed non-specific lymphocytic infiltration with fibrosis and occasional giant cells. Her vision improved remarkably with high-dose steroids with slow tapering. However, she had a low-impact fracture of the left humerus. X-ray showed a cystic lesion at the distal end of the clavicle. On biochemical evaluation, serum calcium was 12.6 mg/dl, serum phosphorus 1.5 mg/dl, serum alkaline phosphatase 360 U/L and serum PTH was 1036 pg/ml. Parathyroid Sestamibi scan showed a left inferior parathyroid adenoma and X-ray skull showed a pepper pot appearance (Figure 2). Surgical excision of the parathyroid adenoma resulted in near-complete remission.
A: X-ray Skull Showing Pepper Pot Appearance, B: Sestamibi Scan Showing Left Inferior Parathyroid Adenoma.
Clinical Case 3
A 42-year-old woman presented with fatigue, bilateral lower limb pain and proximal muscle weakness involving mainly the pelvic girdle resulting in difficulty in ambulation. The thyroid function test, creatine phosphokinase (CPK) and electromyography-nerve conduction study were within normal limits. Muscle biopsy done in view of proximal muscle weakness revealed atrophy of type 2 muscle fibres. Biochemical studies revealed very low 25-OH vitamin D <3 ng/mL (normal >30 ng/mL), high iPTH 1084 pg/ml, serum calcium 8.2 mg/dl, serum phosphate 1.2 mg/dl, and serum alkaline phosphate 1235 U/L. X-ray pelvis showed rarefaction of the pelvic bones and decreased cortical density along the inner margin of the femoral neck suggestive of a looser zone. A diagnosis of OM due to vitamin D deficiency with secondary HyPT was confirmed. She received vitamin D and calcium supplementation. There was resolution of bony pains, proximal myopathy within the first 15 days with complete clinical and biochemical resolution within 3 months.
Discussion
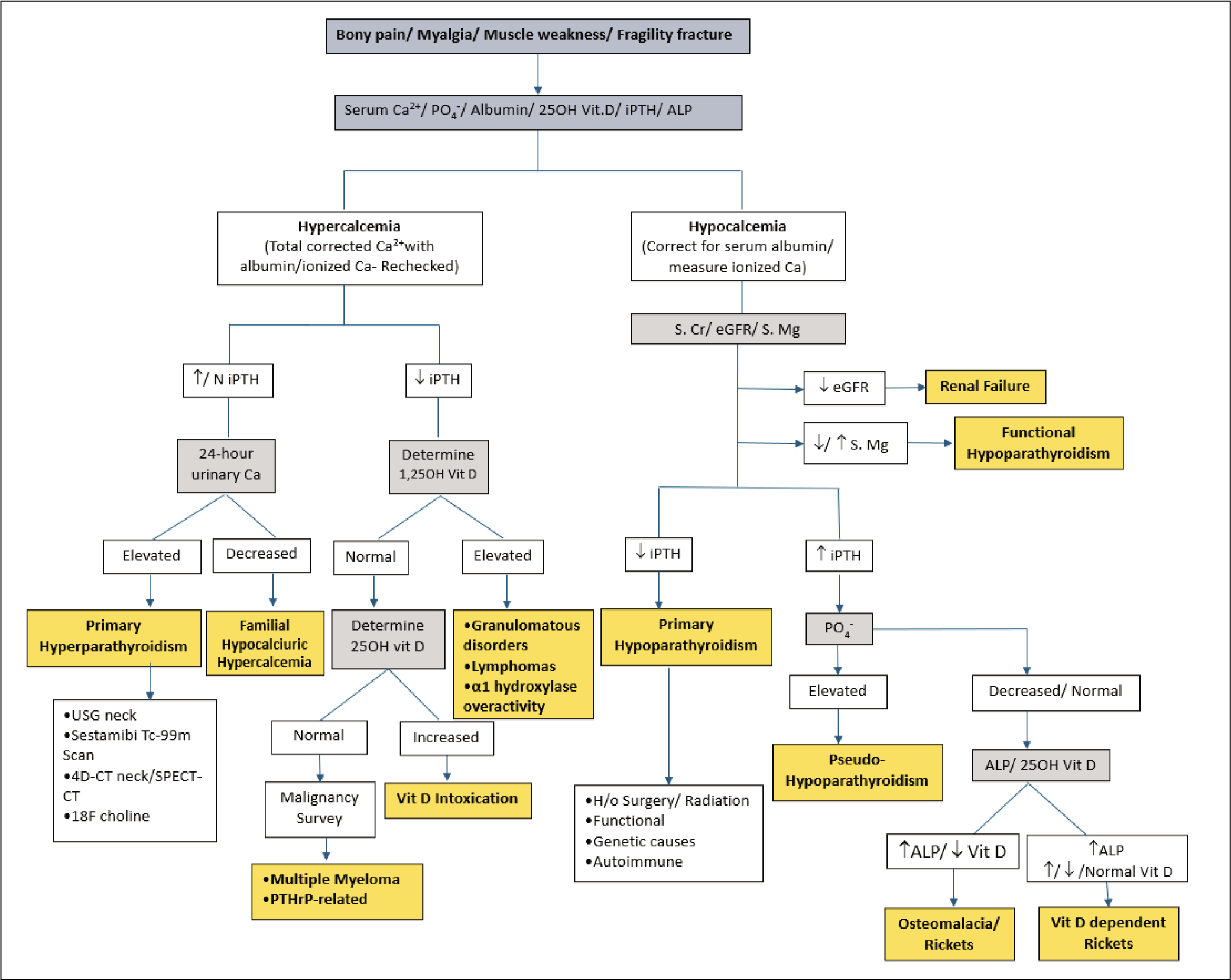
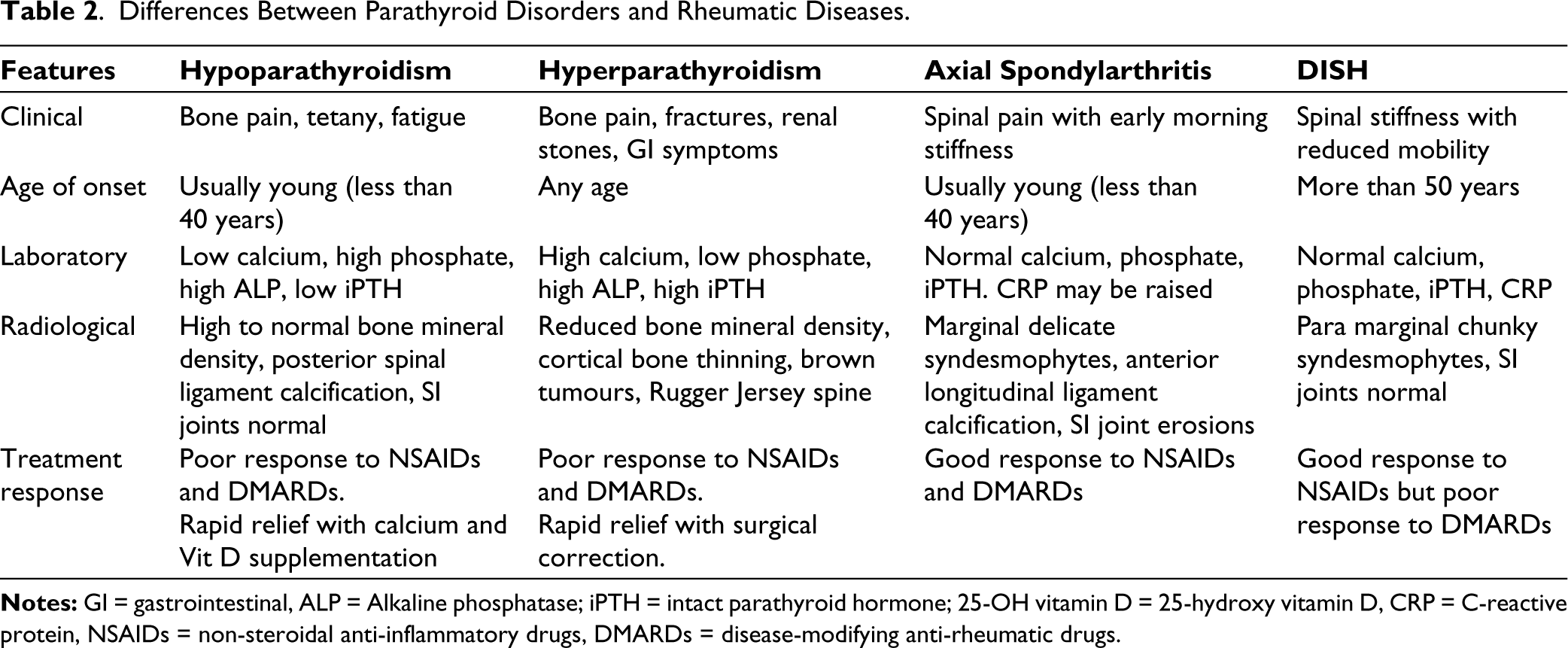
The approach to parathyroid disorders has been elaborated in Figure 3. Primary HoPT causes hypocalcaemia leading to neuromuscular excitability, tetany, and hyperphosphatemia resulting in ectopic mineralisation of soft tissues. X-rays show ossification of the iliolumbar ligament, calcification of acetabular margins of the hip joint, para-vertebral ossification, and SI joint sclerosis without erosions (Table 1). 3 Such features could be mistaken for SpA or DISH. Similarities with SpA are early morning stiffness, axial pain, and gait or posture abnormality. SpA-like syndesmophytes can be seen in HoPT but the involvement of posterior paraspinal ligament is more frequent, and SI joint erosions are rare. There is a poor response to NSAIDs and biologicals but dramatic improvement with calcium and vitamin D supplementation. HoPT is mostly seen in the young whereas DISH is rarely reported before 50 years of age (Table 2). 2 Low bone turnover results in bone mass that is relatively higher than age-and sex-matched controls, especially in the lumbar spine which can be confirmed using Dual-energy X-ray absorptiometry. 11
Approach to Parathyroid Disorders.
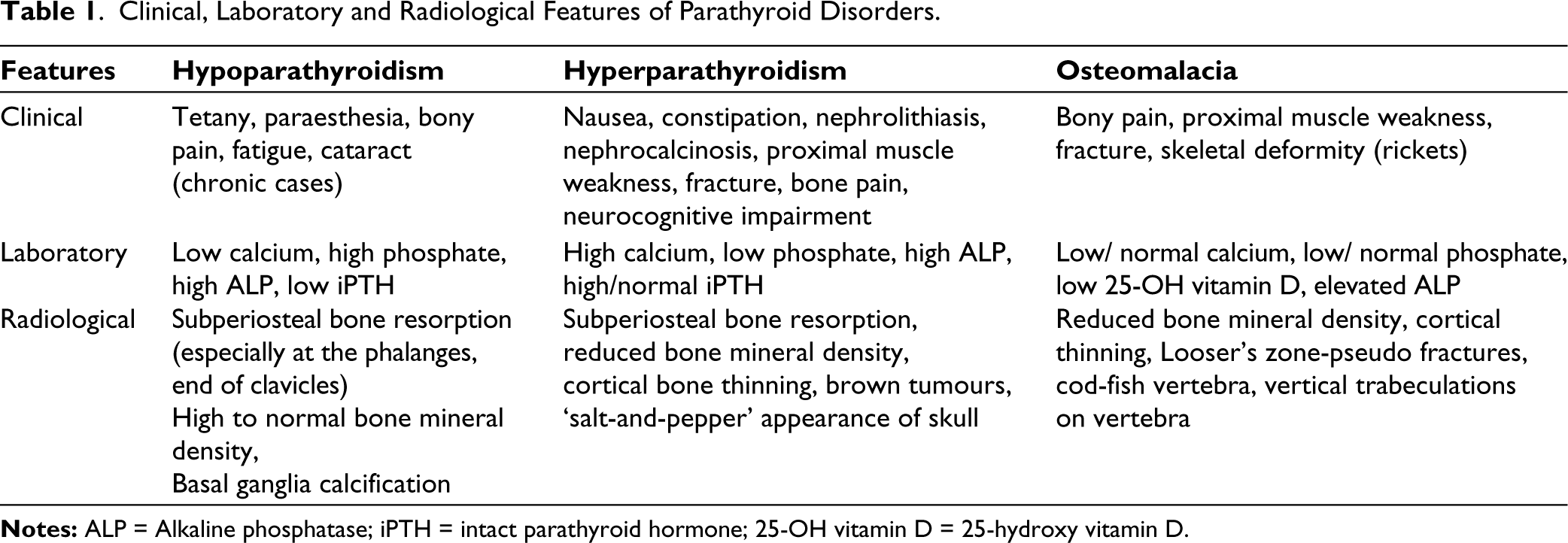
Clinical, Laboratory and Radiological Features of Parathyroid Disorders.
In HyPT, hypercalcaemia commonly presents with renal colic and stones. Classical lesions are rarely seen now due to early diagnosis and treatment. Common musculoskeletal symptoms include muscle pain and weakness due to hypercalciuria and dehydration due to polyuria. Bone pain due to cystic changes is commonly seen in the ribs, pelvis, mandible, long bones, and spine. Subchondral bone resorption results in the widening of the articular space with an irregular appearance of the articular margin. Such changes in the small joints of the hand may mimic rheumatoid arthritis whereas similar changes in the pelvis are likely to be confused with SpA. HyPT can also be associated with hyperuricemia resulting in gout and calcium pyrophosphate crystal deposition disease.5,7 Generalised asymmetric osteopenia is commonly seen in HyPT. Long-standing untreated disease can result in osteoporosis and an increased risk of fragility fracture. Osteopenia in HyPT is more peripheral in contrast to predominant axial bone loss seen in senile and post-menopausal osteoporosis. Surgical removal of parathyroid gland is a curative treatment for primary HyPT. It results in improvement in bone mineral density over time with complete resolution of all symptoms.12,13
Differences Between Parathyroid Disorders and Rheumatic Diseases.
OM can be an outcome of several pathogenic mechanisms, the primary cause being vitamin D deficiency. Altered mineralisation due to calcium and phosphate deficiency can ensue from chronic malabsorption syndromes, chronic kidney disease, chronic liver disease, medications like glucocorticoids/anticonvulsants, vitamin-D-dependent rickets, hypophosphatemic rickets, FGF-23 excess disorders. 10 Common symptoms include bony pain, proximal muscle weakness, and uncommonly fragility fracture.9,14 Non-specific signs and symptoms may lead to misdiagnosis of rheumatological disorders like fibromyalgia or ankylosing spondylitis and delay treatment initiation. Biochemical investigations favouring the diagnosis of OM include elevated ALP, low 25-OH vitamin D, low-normal calcium, low phosphate, elevated iPTH.8,15 HyPT secondary to vitamin D deficiency helps maintain the calcium in the low-normal range. Radiological manifestations of OM include pseudo-fractures, mainly affecting the weight-bearing bones like the proximal/sub-trochanteric region of femur, pelvis and metatarsal bones. Imaging may also reveal rachitic rosary, cod-fish vertebra, cortical discontinuities, vertical trabeculations on the vertebra. 16 OM is usually characterised by low BMD, however, some forms of OM like X-linked hypophosphatemic rickets may manifest as high BMD secondary to enthesopathy. Supplementation of vitamin D and calcium leads to resolution.
Conclusions
Disorders of PTH can closely mimic inflammatory arthritis and spondylitis leading to a delay in diagnosis and inaccurate treatment. The presence of atypical features or inadequate treatment response should prompt a search for parathyroid disorders.
Footnotes
Data Availability Statement
Further data can be made available on request from corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
In compliance with ethical standards consent was taken from all patients before data use.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.