
Abstract
Aim:
The aim of this study was to estimate prevalence of hand osteoarthritis (HOA) and identify patterns in female patients with symptomatic primary knee osteoarthritis (KOA) presenting in a rheumatology outpatient department (OPD).
Methods:
A hospital-based cross-sectional study was done among 145 female patients with primary KOA, as per American College of Rheumatology (ACR) criteria, utilising the right knee as the index knee. The presence of Kellgren–Lawrence (K-L) grade ≥2 radiological changes in two of three groups of hand joints in dominant hand was used to identify hand arthritis (HOA). Symptomatic HOA (SHOA) was defined as existence of hand discomfort within preceding month. Hand disability was measured using the Health Assessment Questionnaire (HAQ); a mean score of >0.5 was deemed to be a significant disability. Global Hand Kellgren–Lawrence Score (KLTOT) was used to assess radiographic severity of HOA.
Results:
The prevalence of HOA was found in 96 (66%) patients, with a higher prevalence in patients above 60 years of age. At the individual joint level, 102 (71.7%) patients had DIP involvement, 96 (66.2%) had PIP involvement, 40 (27.5%) had metacarpophalangeal (MCP) involvement, and 57 (34.4%) had involvement in the base of the thumb. SHOA was found in 48 (33%) patients, and significant disability was noted in 38 (26.2%) patients. There was a significant positive correlation between global KLTOT and body mass index (BMI) (P = .004) and between global KLTOT and HAQ (P = .002). A significant difference was found between HOA and the radiographic severity of the KOA (P = .003) in comparison to patients without HOA.
Conclusion:
HOA is common in elderly women, especially those with primary KOA.
Keywords
Introduction
The most prevalent joint disease is osteoarthritis (OA), which has significant social and financial consequences in addition to causing pain and functional impairments. It ranks among the most common musculoskeletal causes of disability in the globe. Although knee OA (KOA) is the most common site of primary site, hand osteoarthritis (HOA) is also a prevalent OA phenotype. 1 HOA frequently causes disability and may significantly affect the quality of life. 2 HOA is as significant as rheumatoid arthritis (RA) in affecting health-related quality of life. Some studies suggest that HOA can be as severe as, or even more severe than RA, impacting the quality of life equally or more. 3
With increasing life expectancy and an expanding elderly population, hand OA is likely to become a significant cause of morbidity in the Indian population. Despite this, there is a dearth of information on HOA in India. Just one study—published by Ghosh et al.—found that 40% of individuals with knee OA also had HOA. Data about the pattern of HOA or the degree of disability in patients was not studied. 4 This gap in knowledge highlights the need for further research on the prevalence and patterns of HOA, especially in the Indian context.
Hand OA can occur independently of knee OA; however, this study focused on female patients with symptomatic KOA. This subset was chosen because it allowed for a focused study within a hospital setting, where patient recruitment and data collection are more manageable. Female patients were specifically chosen because women are more likely to suffer from OA. 5 The main aim of this study was to estimate prevalence and patterns of HOA among female patients with symptomatic KOA.
Material and Methods
Between June and August 2021, a cross-sectional prospective hospital-based study was conducted at the Hind Institute of Medical Sciences’ Rheumatology Clinic in Safedabad, Uttar Pradesh, India. Each patient provided written informed consent, and study was approved by authorised by the Institutional Ethical Committee. The study comprised 145 female patients with primary KOA who were over 40 years of age in consecutive order. The American College of Rheumatology (ACR) clinic-radiological criteria of 1987 for KOA used to make the diagnosis of primary KOA. 6 The right knee was taken as the index knee in the patients. Patients with congenital abnormalities of the hand or knees, a history of trauma to the knee or hand, or metabolic bone disease were excluded to participate in the study. Data regarding demographic profiles, duration of disease, disease characteristics and associated risk factors for chronic diseases, menstrual history and medical and drug history were obtained from each patient.
Evaluation of Patients
The right knee was looked for presence of tenderness, swelling and crepitus. A visual analogue scale (VAS) ranging from 0 to 100 mm was used to measure intensity of pain in knee. Every patient’s dominant hand was examined. When asking patients if they had experienced hand pain in the previous month, the VAS was used to measure the degree of pain on a scale from 0 to 100 mm. The 16 hand joints that were examined were: four proximal interphalangeal joints (PIP), five metacarpophalangeal (MCP) joints, five distal interphalangeal joints (DIP, including thumb interphalangeal joint or DIP 1), five bases of the thumb, including the thumb’s carpometacarpal (CMC) joint and trapezioscaphoid (TS) joint. Bony swellings in the form of Heberden’s and Bouchard’s nodes over DIP and PIP joints were noted. The disability was evaluated using the Stanford Health Assessment Questionnaire (HAQ). The HAQ’s eight hand function-related questions were utilised to measure hand disability. With the Indian population in mind, the fourth question about chopping meat was changed to chopping vegetables. From ‘no difficulty’ (0) to ‘unable to do’ (3), each question was given a score. On a scale from 0 (no hand disability) to 3 (severe hand disability), the scores were averaged to provide an overall hand disability score. A hand disability ranging from moderate to severe was indicated by a mean score of ≥0.5. 7
Radiographic Evaluation
A radiologist who was blind to the patient’s demographic and clinical features evaluated the radiographs. A posteroanterior radiograph of the dominant hand with the wrist and a standard anteroposterior radiograph of the knee was taken. The modified Kellgren–Lawrence scale, which was employed in the Framingham study, was utilised to grade each joint (knee, hand and wrist) for radiographic OA. 8
Definitions
Radiographic Hand Osteoarthritis at Individual Joint Level (ROA): A K-L grade of ≥2 was used to determine ROA for each joint. DIP, PIP, MCP and CMC1/TS joint groups were regarded as positive if at least one joint in the group had a K-L grade of ≥2.
HOA: Characterised as having a K-L grade of ≥2 in two of each hand’s three groups of hand joints (DIP, PIP and CMC1/TS).
Symptomatic Hand Osteoarthritis at Individual Joint Level (SHOA): At the hand joint level, SHOA was defined as the presence of HOA at that joint, along with pain/aching/stiffness for most days of the last month.
Global Hand Kellgren–Lawrence Score (KLTOT): Calculated by summing the respective K-L scores at each of the 16 hand joints, with a maximum score of 0–64 for the dominant hand.
Statistical Analysis
The SPSS software, version 25.0, was used to analyse the data. The clinical and demographic features of the patients were compiled using descriptive statistics. Categorical data were expressed as frequencies and percentages, and continuous variables were expressed as mean ± standard deviation (SD). The distributions of HOA by age and body mass index (BMI) were examined using chi-square testing and cross-tabulations. To examine the association between KLTOT and other variables, including BMI and HAQ scores, Pearson’s correlation coefficient was employed. Utilising independent t-tests for continuous variables and chi-squared tests for categorical variables, the connection between HOA and KOA variables (duration and degree of knee pain, radiographic severity of KOA) was examined closely. Utilising a chi-square test, the relationship between HOA and the radiographic severity of knee. A P < .05 was considered significant.
Results
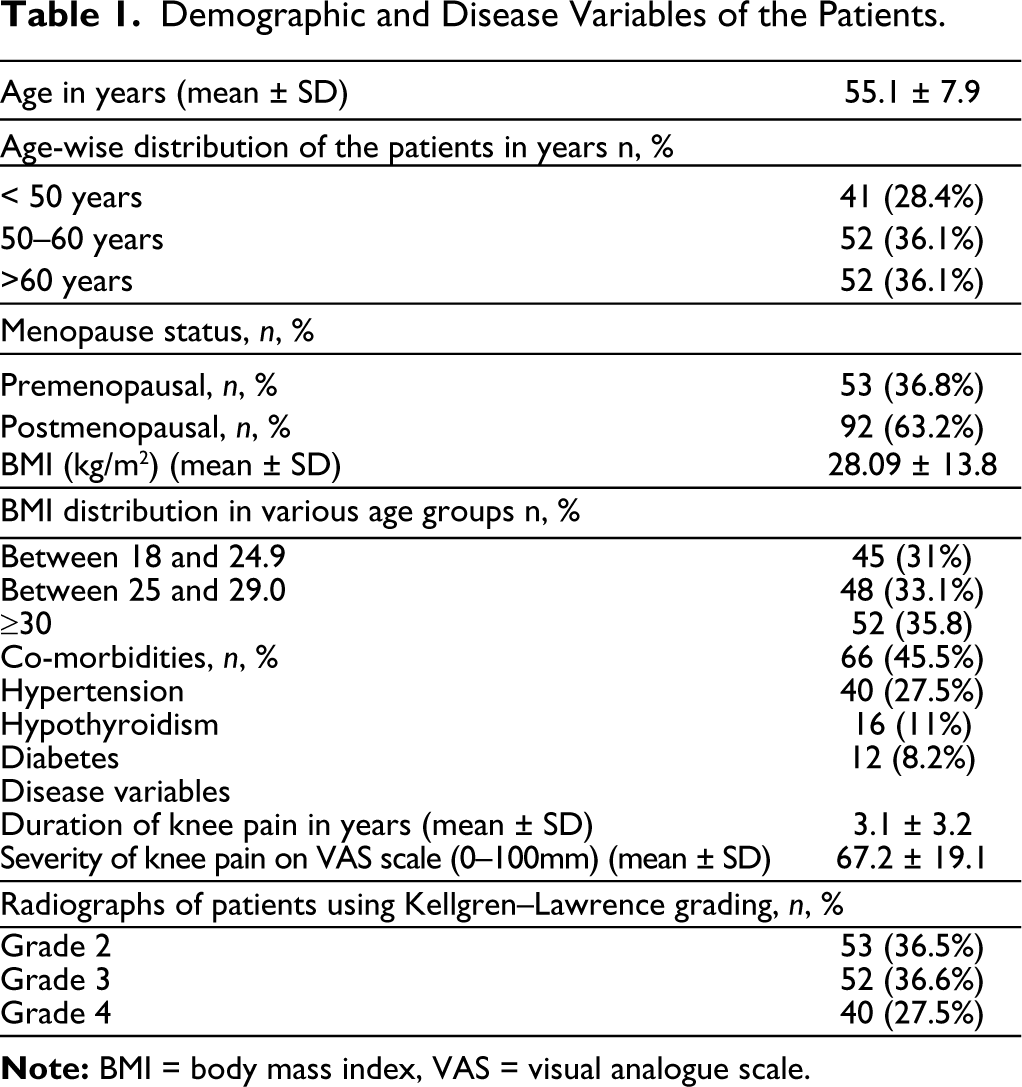
The study comprised 145 female patients of primary KOA with right-sided dominance. Table 1 displays the characteristics related to disease and demographics.
Demographic and Disease Variables of the Patients.
Prevalence and Patterns of HOA in the Patients
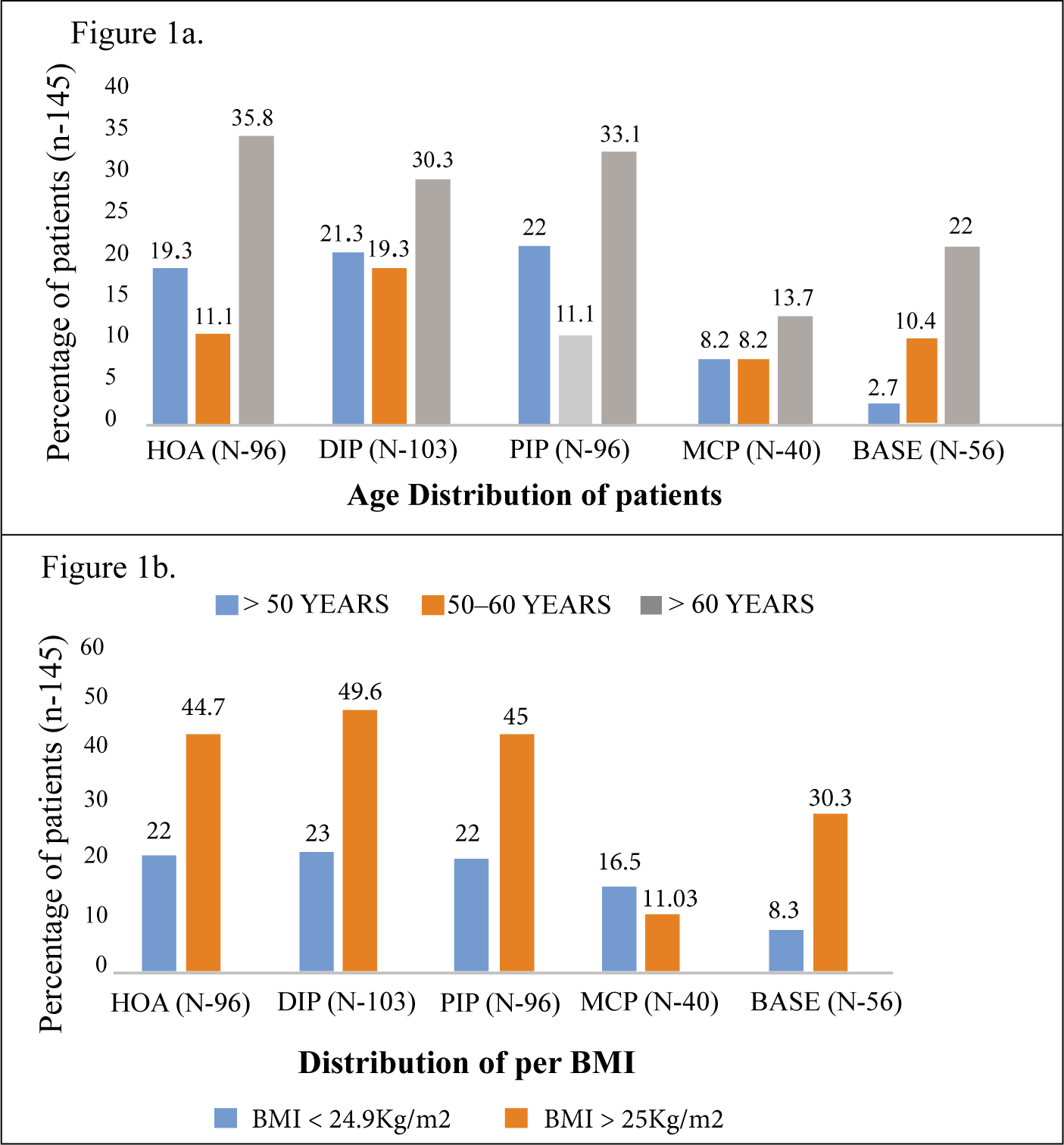
HOA was found in 96 (66.6%) patients. At the individual joint level, 102 (71.7%) patients had DIP involvement, 96 (66.2%) had PIP involvement, 40 (27.5%) had MCP involvement and 57 (34.4%) had involvement of the base of the thumb. In twenty (13.7%) of the patients, there were Heberden’s and Bouchard’s nodes.
HOA patients had mean age of 57 ± 6 years. The prevalence was higher in patients above the age of 60 years and lowest in patients between 50 and 60 years. The age-wise distribution of HOA and as per involvement at individual joints is shown in Figure 1a. The mean BMI of patients with HOA was 26.3 ± 10 kg/m². The distribution of patients according to BMI is shown in Figure 1b. The prevalence was higher in patients with a higher BMI, except at the MCP joint.
SHOA was found in 48 (33.1%) patients with HOA. The severity of pain was 24.1 ± 26.4 mm on the VAS scale. Significant functional disability was found in 38 (26.2%) patients, with a mean HAQ score of 0.64 ± 0.9. The mean combined hand KLTOT was 33 ± 21.
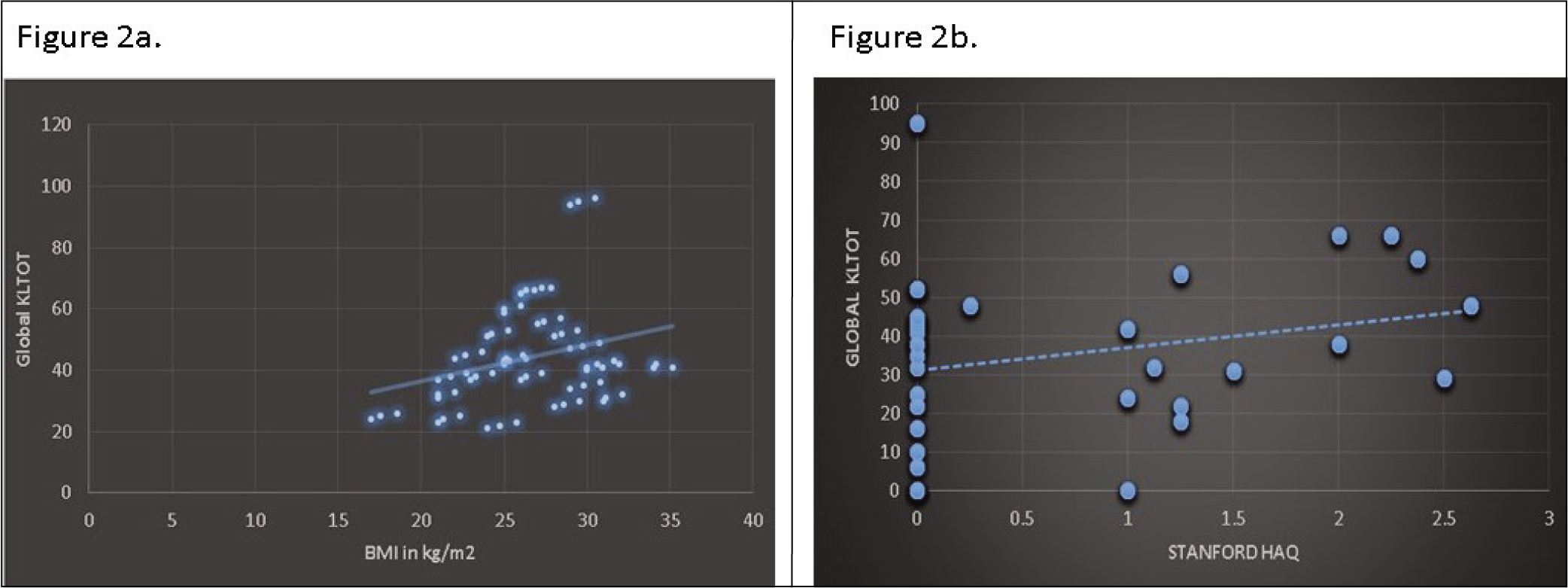
The KLTOT was then compared to various other parameters of HOA. A positive correlation was found between BMI and KLTOT (r = 0.286, P = .004) and between HAQ and KLTOT (r = 0.248, P = .002) (Figure 2a and b). There was no relationship between disease duration (r = 0.0004, P = .9) and the severity of pain (r = 0.12, P = .4) with KLTOT.
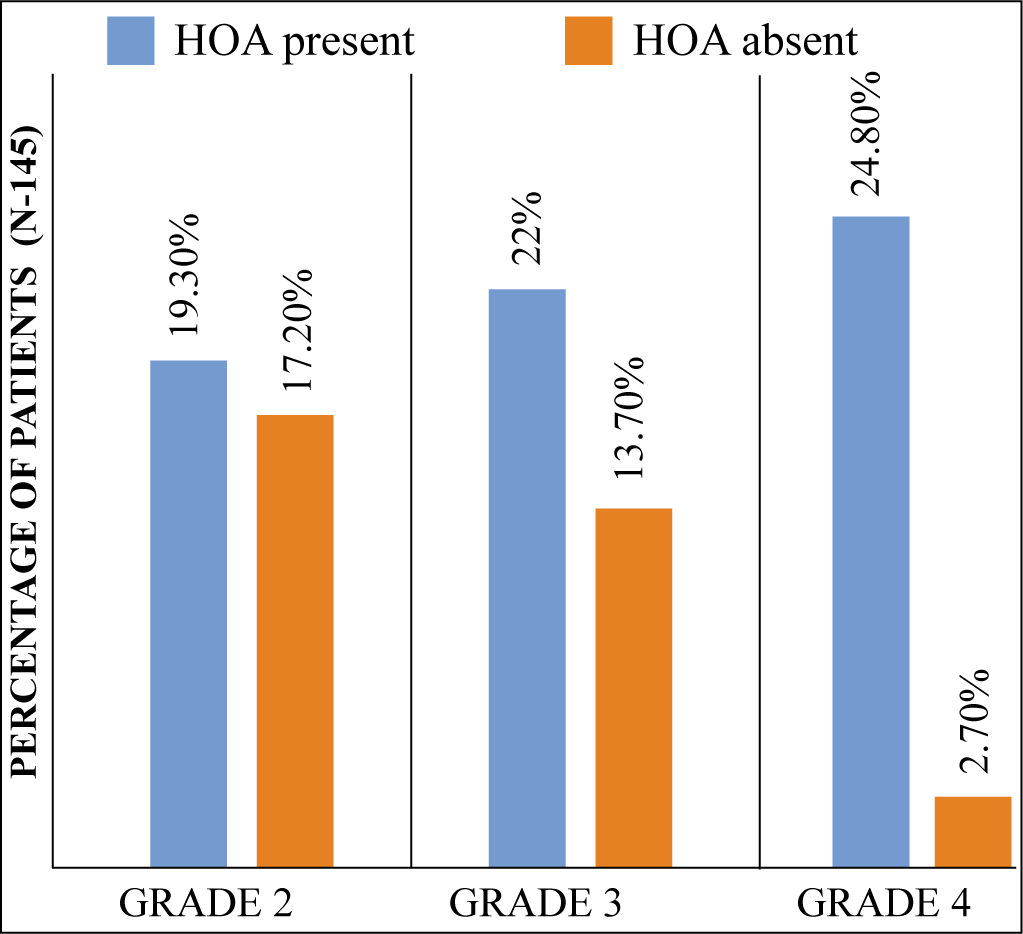
Patients with HOA were compared to KOA variables, such as the duration and severity of knee pain and the radiographic severity of KOA. There was no significant difference in the severity and duration of knee pain between patients with HOA and those without it. However, a notable difference was observed in the radiographic severity of KOA between the two groups, as indicated by a chi-squared value of 16.21 (P = .003) (Figure 3).
Discussion
This study looked at the prevalence and patterns of HOA in female patients with symptomatic primary KOA attending a rheumatology clinic. It is well-known that OA is more common in females, and Polyarticular phenotypes exist in many cohorts studied to date, including the simultaneous presence of hand and knee joint involvement. 9 The association between KOA and HOA has also been studied, which was the rationale for focusing on HOA in female patients with symptomatic KOA.
The prevalence of HOA in this cohort was found to be 66.6%, which is higher than the 40% prevalence reported by Ghosh et al. in a similar cohort of Indian patients with KOA. 4 This disparity could be attributed to differences in study populations, diagnostic criteria, and regional variations in lifestyle and genetic factors. The pattern of joint involvement in this study is similar to previous findings, except for a higher PIP involvement than CMC involvement and MCP involvement in these patients. 7 The study population comprised both rural and urban females involved in farming practices, which could account for the higher MCP and PIP involvement in the dominant hand, although the relationship between occupation and joint involvement was not studied. 10
Age and BMI were significant factors influencing the prevalence of HOA. In this study, the prevalence was higher in patients under 50 years of age compared to those between 50 and 60 years. The prevalence was again high in patients over 60 years. Unlike knee and hip OA, where the prevalence increases with age, the prevalence of HOA peaks around menopause, then decreases before increasing again in later life. 11 This study shows similar results considering the fact that majority Indian females have menopause in the 4th decade. 12 Additionally, the mean BMI of patients with HOA was 26.3 kg/m². A higher BMI was associated with an increased prevalence of HOA, except at the MCP joint. 13 This highlights obesity as a modifiable risk factor in the development and progression of HOA, emphasising the importance of weight management in the prevention and treatment of OA.
Symptomatic hand osteoarthritis (SHOA) was present in 33.1% of patients with HOA, and these patients reported a mean pain severity of 24.1 mm on the VAS scale. Furthermore, significant functional disability was observed in 26.2% of patients, with a mean HAQ score of 0.64. These results demonstrate that a substantial proportion of patients with HOA experience considerable pain and functional impairment, severely impacting their quality of life. The positive correlation between HAQ scores and the global KLTOT indicates that higher radiographic severity of HOA is associated with greater disability, underscoring the importance of early diagnosis and intervention to mitigate the functional consequences of HOA. Interestingly, no significant correlation was found between the severity of hand pain and the KLTOT, suggesting that radiographic severity may not always correspond to clinical symptoms. This phenomenon is known in HOA, where radiographic findings and clinical symptoms can sometimes diverge. 14
Comparative analysis of HOA and KOA variables revealed no significant relationship between HOA and the duration or severity of knee pain. However, a significant association was found between the radiographic severity of knee OA and the presence of HOA. This suggests that patients with more severe radiographic knee OA are more likely to have concomitant HOA, possibly due to shared risk factors such as age, obesity and mechanical stress on the joints. 15
This study has some limitations. The cross-sectional design provides only a snapshot and does not establish a causal relationship or track the progression of KOA or HOA. Since the study was conducted only on female patients, the results cannot be generalised to the broader population. Apart from age and BMI, no other risk factors were assessed, such as genetics, occupation, or physical activity levels, which may have influenced the results.
Conclusion
In conclusion, this study demonstrates a high prevalence of HOA in female patients with symptomatic primary KOA, with significant age- and BMI-related trends. The substantial proportion of patients experiencing SHOA and functional disability highlights the need for integrated management approaches addressing both KOA and HOA. Future studies should explore the underlying mechanisms linking knee and hand OA and investigate targeted interventions to improve outcomes in this patient population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Patient Consent
Ethical approval was taken from the Institutional ethical committee and informed consent was obtained from every patient.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.