
Abstract

Dear Editor,
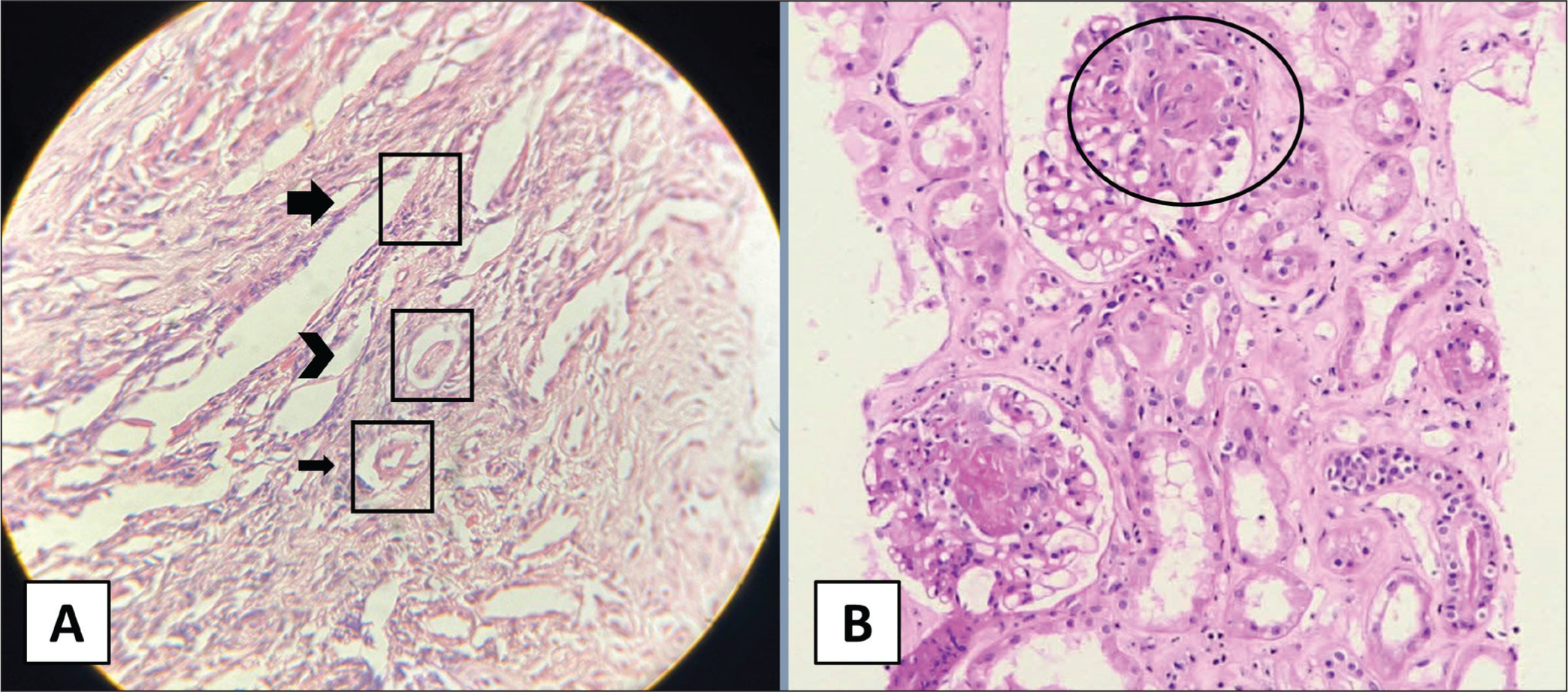
The letter by Mruthyunjaya P et al. reminded me of the following case that I had come across. 1 A 77-year-old male presented with a 10-month history of additive, symmetrical, non-deforming, polyarthritis, rheumatoid factor (RF) >80 IU/ml (>20 IU/ml being positive), a negative anti-cyclic citrullinated proteins (anti-CCP) test, inadequately controlled diabetes mellitus, a history of diabetic retinopathy, raised serum creatinine (1.7 mg/dl) and peripheral neuropathy in a glove and stocking distribution. He also had a non-healing ulcer over the lateral border of the tongue for 1.5 months. He was a previous smoker (stopped >10 years back) and teetotaller and did not use betel nut or related products. He had no other ear, nose or throat symptoms. At the time of presentation to the clinic, the patient had been initiated on low-dose steroids and hydroxychloroquine by a physician with only mild relief in arthritis and was under the care of an otorhinolaryngologist for his non-healing tongue ulcer. Initial presentation suggested seropositive rheumatoid arthritis (RA) with chronic kidney disease (diabetic nephropathy) with diabetic peripheral neuropathy. There were no other atypical features. Since the tongue ulcer could not be attributed to RA and considering the patient demographic, a biopsy was advised which revealed leukocytoclastic vasculitis. A further workup for systemic vasculitis was done which included an anti-nuclear antibodies profile (ANA profile) and anti-neutrophil cytoplasmic autoantibodies (ANCA). The urine protein creatinine ratio was 1.49 and the urine routine showed 20-25 pus cells/high power field (hpf), numerous red blood cells/hpf with a sterile urine culture. In the meantime, proteinase 3 (PR3)-ANCA returned positive 17.4 IU/ml (<10 being negative). A renal biopsy confirmed pauci-immune focal necrotising & crescentic glomerulonephritis with diffuse acute tubular injury (Figure 1). Patient was initiated on high-dose steroids and rituximab which led to the disappearance of arthritis, improvement in renal function and reduction in his paraesthesia. On follow-up his RF became negative.
(A) Biopsy of Tongue Ulcer Showing: broad arrow-nuclear dust, arrow head-intraluminal fibrin deposition, thin arrow-inflammatory cells infiltrating vessel wall (40× magnification); (B) early crescent formation of crescentic glomerulonephritis (10× magnification).
ANCA-associated vasculitis (AAV) can be missed in patients with high titre RF positivity with polyarthritis, who may be initially seen by physicians/orthopaedicians and labelled seropositive RA. A high index of clinical suspicion by the rheumatologist is essential. Cases such as the example above, in which other possible explanations could be present for the various clinical manifestations, make it harder to arrive at the right diagnosis. An important feature in these patients is the negative anti-CCP test and in most, RF becomes negative with treatment of the AAV. Moon J et al noted RF positivity of 39.1% in 128 patients of AAV. 2 Watanabe S et al. suggested an association of RF positivity with more severe disease and poor prognosis in AAV but Ahn S S et al. did not find a correlation.3,4 The presence of RF positivity could be due to increased immunoglobulin G (IgG) production (targeted by RF) in these patients. This case reiterates the importance of a detailed history & clinical examination even in today’s world dominated by artificial intelligence (AI).
Footnotes
Acknowledgements
The author acknowledges the support of Dr Priya M & Dr Greeshma Ann George in obtaining the pathology images.
Author Contributions
The author takes full responsibility for the integrity and accuracy of all aspects of the work.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance was exempted as this is an isolated clinical case and image presentation.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the patient for publication.