
Abstract

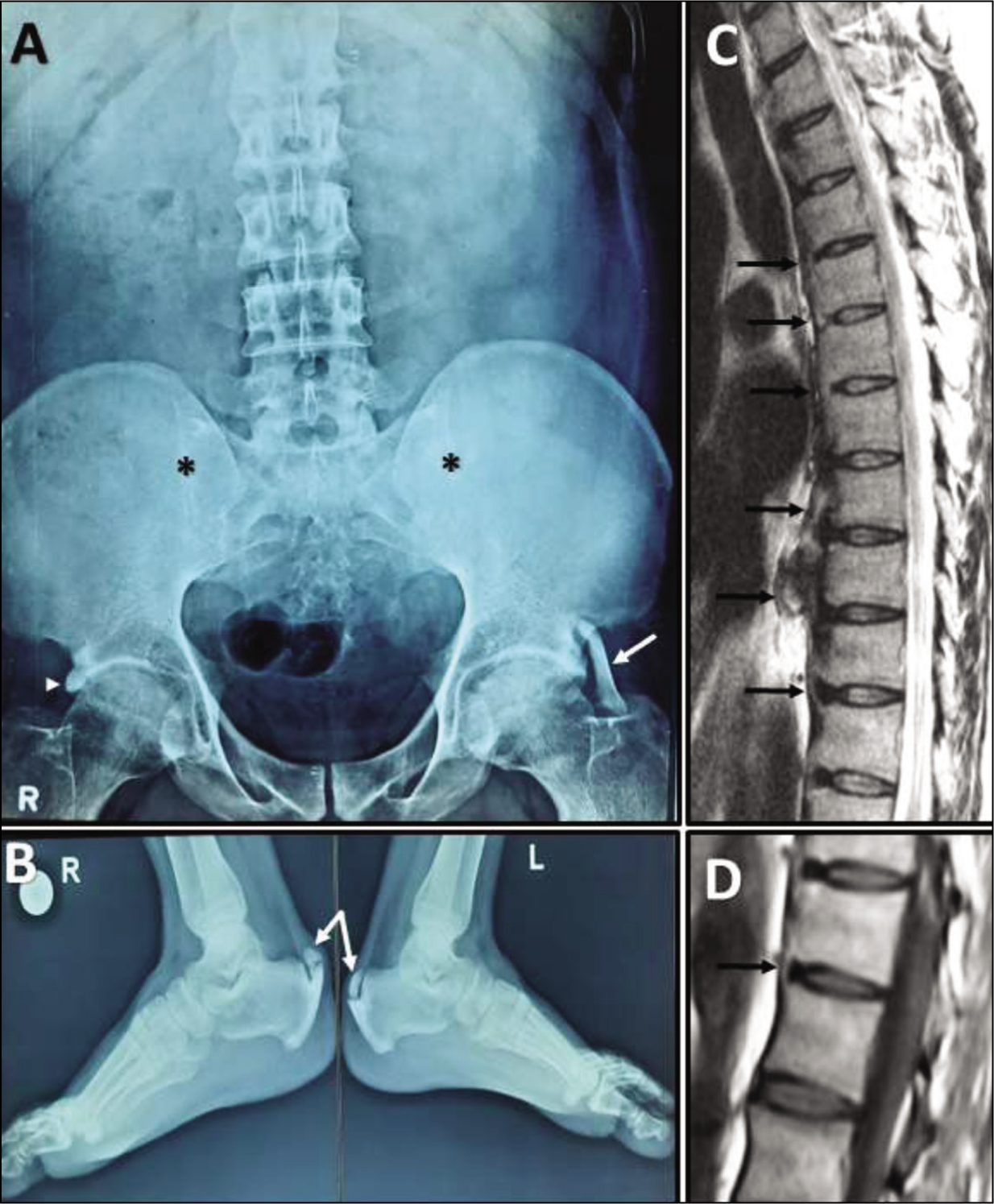
A 40-year-old male with ankylosing spondylitis (AS) of 16 years duration was doing well on intermittent non-steroidal anti-inflammatory drugs (NSAIDs); he now presents with worsening of his low-back pain (mechanical type) and associated bilateral heel pain for the past three years. He did not have any comorbidity or addictions. On examination, Flexion abduction external rotation (FABER) test was negative, modified Schober’s test was 4 cm and tenderness was present at both Achillis tendon insertion sites. His blood investigations showed a positive human leukocyte antigen B27 (HLA-B27) however, all other tests were normal including lipid profile, haemoglobin A1c (HbA1c), thyroid function test, insulin-like growth factor 1 (IGF-1) and inflammatory markers (erythrocyte sedimentation rate [ESR]: 18 mm/hr and C-reactive protein [CRP]: 1.2 mg/L). Radiographs of pelvis and both ankle joints (Figure 1A and B) showed bilateral grade 4 sacroiliitis, left iliofemoral ligament calcification, right acetabular entheseal hyperostosis and bilateral Achilles tendon ossification. The sagittal T2-weighted magnetic resonance imaging (T2W MRI) of dorsal spine (Figure 1C) showed ossification of the anterior longitudinal ligament involving more than four contiguous vertebral levels with preserved disc heights; sagittal T1W MRI at lower dorsal level (Figure 1D) showed syndesmophytes and MRI of bilateral sacroiliac joint showed chronic sacroiliitis with bony ankylosis. A diagnosis of AS with inactive disease (Bath AS Disease Activity Index (BASDAI) 2.1) and co-existing diffuse idiopathic skeletal hyperostosis (DISH) was made. He was prescribed NSAIDs along with regular physiotherapy and follow-up after three months showed significant improvement in his symptoms and was off NSAID therapy.
(A) Anteroposterior radiograph of the pelvis with both hip joints demonstrates symmetric, significant reduction in the bilateral sacroiliac joint spaces with ankylosis suggestive of grade IV sacroiliitis (asterisks), calcification of the iliofemoral ligament on the left side (white arrow) and acetabular entheseal hyperostosis on the right side (arrowhead). (B) Lateral radiographs of bilateral ankle joints demonstrate ossification of the bilateral Achilles tendons (white arrows). (C) Sagittal T2-weighted MRI of dorsal spine showing ossification of the anterior longitudinal ligament (black arrows) involving more than four contiguous vertebral levels with preserved disc heights. (D) Sagittal T1-weighted MRI at the lower dorsal level demonstrates fine, vertical bridging ossification at the outer disc limit extending only up to the adjacent end-plate margins s/o syndesmophyte (black arrow).
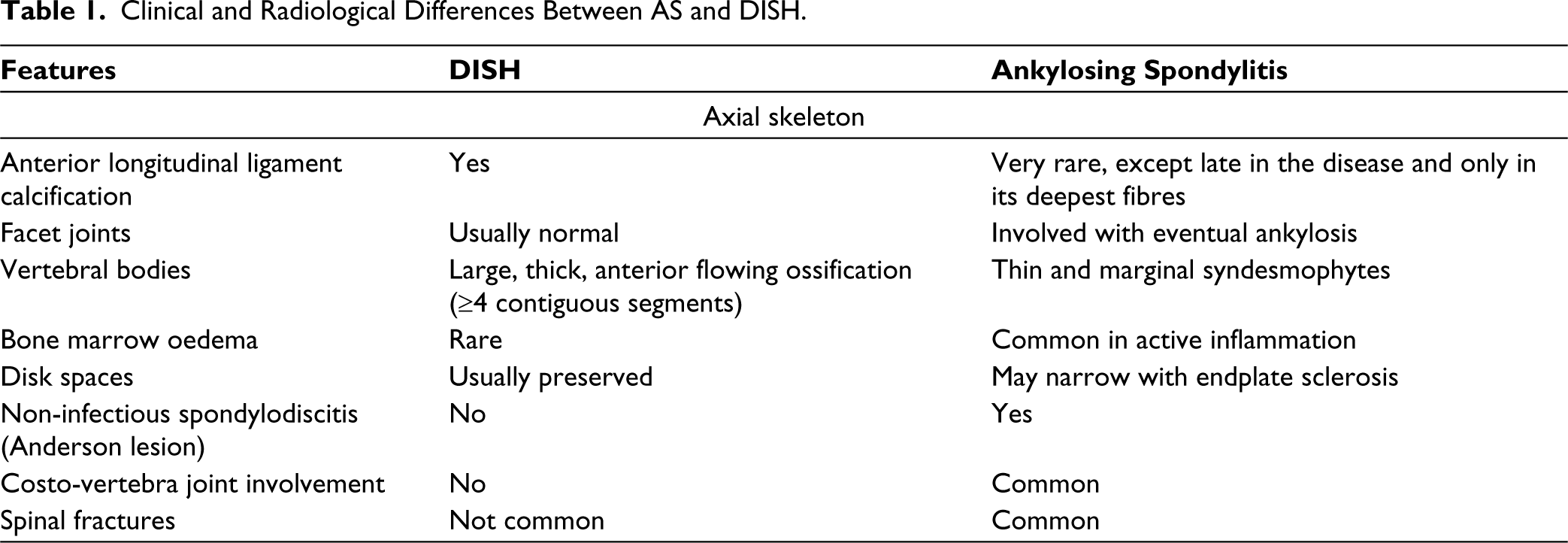
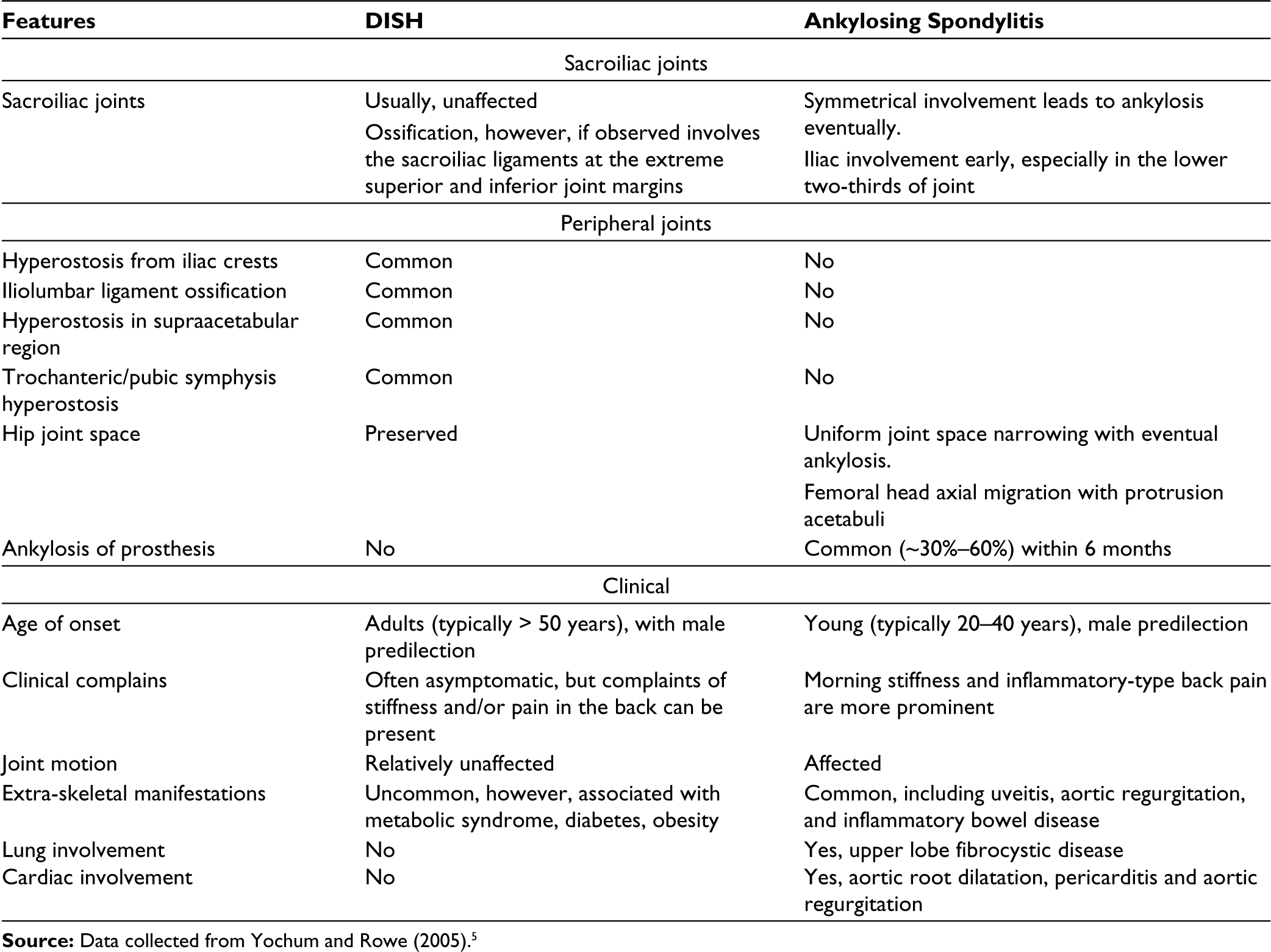
AS and DISH are two entirely separate pathological entities, characterised by ossification of the ligaments and tendons in both axial skeleton and peripheral sites. AS is an inflammatory disease, whereas DISH is considered as non-inflammatory/degenerative disease in which the advancing age and metabolic factors (such as obesity, arterial hypertension, type 2 diabetes, hypercholesterolemia and hyperuricemia) play a major role. 1 The origin or site of both diseases appears to be located within the entheses, resulting in new bone formation with markedly different radiographic patterns. 2 Recognising these radiological (on computed tomography [CT] and MRI) findings is necessary to differentiate between them. It is becoming clearer that the sacroiliac joint (SIJ) can be affected in DISH and this finding should not be mistaken for axial spondylarthritis (ax-SpA). Entheseal ankylosis (fusion within the ligamentous portion) and anterior para-articular bridging of SIJ are somewhat characteristic of DISH. However, intra-articular ankylosis, erosions, bone marrow oedema and subchondral sclerosis are also found in SIJ of DISH; but they are still considered more characteristic of AS. In DISH, facet and costovertebral joints undergo degenerative changes. Costovertebral joints can also be site of entheseal ossifications (radiate and costotransverse ligaments) and rib hyperostosis. Ankylosis of both these joints constitutes an argument for discerning it from ax-SpA even though some DISH patients were found to have intra-articular fusion of these joints. 1 In a study done by Weiss et al., MRI of the spine and SIJ has been suggested to discriminate between patients with AS and DISH, but despite the significantly more frequent facet and SIJ ankylosis in the AS group, ankylosis was also observed in some of the DISH cases. 3 Table 1 briefly describes clinical and radiological differences between these two diseases.
Clinical and Radiological Differences Between AS and DISH.
Co-existence of both these diseases in same patient is very rare, but there have been many published case reports and systematic reviews of their concomitant occurrences.1,2,4 It is important to be aware of this entity to avoid a misdiagnosis in such patients and treatment should be tailored according to the patient’s clinical symptoms, since treatment strategies differ between AS and DISH. Further studies are warranted to understand exact pathophysiology, prognosis and long-term complications in patients with these co-existing diseases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written consent has been obtained from the patient for publication.