
Abstract
Background:
IgG4-related disease (IgG4-RD) is a multi-organ, fibro-inflammatory disorder characterised by tumefactive lesions. Corticosteroids are the first line of treatment. Rituximab (RTX) has been reported to be effective in IgG4-RD. It is reserved as a second-line agent and is a useful treatment option for those with intolerance to corticosteroids or have steroid and immunomodulator refractory disease.
Objectives:
To assess the response to treatment with RTX in patients with IgG4-related disease at the end of 6 months.
Methods:
A total of 27 patients diagnosed with IgG4-RD and treated with at least 1g of RTX were included. Patient demographics, clinical data and investigations were noted. Response to RTX was noted at the end of 6 months in terms of clinical improvement, decrease in or normalisation of serum IgG4 levels, withdrawal of steroids or disease-modifying antirheumatic drugs (DMARDs) and the calculation of the IgG4RD responder index (RI).
Results:
Out of the 27 patients treated with RTX, one patient expired and two were lost to follow-up. Of the remaining 24 patients, nine are off steroids; four patients are off treatment. Among the nine who are off steroids, eight patients had orbital and periorbital involvement. Fourteen patients had elevated IgG4 levels. Post RTX, normalisation of IgG4 levels was achieved in six patients. The average RI before and after RTX was 4.79 (2–10) and 1.33 (0–4), respectively.
Conclusions:
Patients with IgG4-RD who were intolerant or refractory to steroids and other DMARDs showed significant improvement after RTX infusion, especially in orbital and periorbital involvement. It suggests that RTX may be beneficial in the management of IgG4-RD.
Introduction
IgG4-related disease (IgG4-RD) is a fibro-inflammatory disease affecting multiple organs, associated with tumefactive lesions of uncertain origin and distinctive histopathological features. The exact causative factors of IgG4-RD are not fully understood, but existing data suggest possible connections to genetic predisposition, bacterial infections, molecular mimicry, and autoimmune processes.
Individuals affected with IgG4-RD generally exhibit elevated levels of serum IgG4; nonetheless, they may be normal in approximately 30%–50% of cases.1,2 Specifically, individuals with retroperitoneal and isolated ‘head and neck’ involvement tend to exhibit lower IgG4 levels. 3 Biopsy is the gold standard for diagnosing IgG4-RD, marked by dense infiltrates of lymphoplasmacytic cells, a high proportion of IgG4-bearing plasma cells, abundant storiform fibrosis, obliterative phlebitis, and frequent tissue eosinophilia. 4
Timely diagnosis and intervention are crucial to avoid irreversible organ damage, whether it is directly from the disease or as a consequence of unwarranted surgical procedures. Corticosteroids are the primary choice for the initial treatment of IgG4-RD, and the response is characteristically excellent but unsustained. About 30%–60% of patients relapse during the tapering or after withdrawal of GC and will need steroid-sparing agents.
Non-corticosteroid pharmacotherapies have included immunosuppressants (azathioprine, methotrexate, mycophenolate, 6-mercaptopurine, cyclophosphamide, cyclosporine), biological agents (rituximab [RTX], tocilizumab, infliximab, adalimumab), and anti-neoplastic agents (imatinib, bortezomib). 5
RTX is a monoclonal antibody against CD20 and has been reported to be effective in controlling IgG4-RD.3,6-12 Typically reserved as a second-line agent because of cost and potential toxicity, studies indicate that it is a useful treatment option for IgG4-RD patients who are intolerant to or have steroid and immunomodulator refractory.13,14 Herein, we assess the response to treatment with RTX in patients with IgG4RD in our hospital.
Methods
All individuals aged 18 years and above, who presented to the Department of Rheumatology in Sir Ganga Ram Hospital between 2012 and 2023 and were diagnosed with IgG4 related disease based on the 2020 Revised Comprehensive Diagnostic (RCD) criteria for IgG4-RD, and subsequently treated with at least 1g of RTX, were included in this study.
This study was conducted in accordance with the ethical principles that are consistent with the Declaration of Helsinki, International Conference on Harmonisation Good Clinical Practices, and the applicable legislation on non-interventional studies. The study protocol was approved by Independent Ethics Committee prior to the commencement of the study.
Patient information, clinical manifestations, serum IgG4 levels, biopsy results, imaging reports, initial treatment plans, and the total dose of RTX administered were documented. Serum IgG4 levels were quantified using the nephelometric method. Biopsy specimens were examined for typical IgG4-RD findings, and immunohistochemical studies were conducted to identify IgG4-positive plasma cell infiltration. RTX was administered in two divided doses at 15-day intervals, with each dose containing one gram. For patients with an inadequate response, repeat RTX doses were given at 6-month intervals. The response to RTX was assessed based on clinical improvement, the decrease or normalisation of serum IgG4 levels, the discontinuation of steroids or disease-modifying antirheumatic drugs (DMARDs), and the calculation of the 2012 IgG4 responder index (RI) at the end of 6 months.
Subgroup analysis between those patients with normal and elevated IgG4 levels was done. Wilcoxon-Mann-Whitney Test was used to compare the two groups at each of the timepoints. Wilcoxon signed-rank test was used to explore the difference in IgG4 levels and RI between the time points within each group. The generalised estimating equations method was used to explore the difference in change in IgG4 levels and RI between the two groups over time.
Results
Out of the 27 patients included, total number of males were 14 (51.9%) as compared to females 13 (48.1%). The mean age of the patients was found to be 40.9 (18–73) years. The baseline characteristics of the study population are summarised in Table 1. Majority of the patients reported involvement of orbital and periorbital tissue (59.3%), followed by retroperitoneal fibrosis and paravertebral tissue (14.8%).
Baseline Characteristics of the Study Population.

IgG4, IgG4-related disease.
Amongst these 27 patients, 4 (14.8%) patients were diagnosed with definite IgG4-RD, 11 patients (40.7%) with possible IgG4-RD and 12 patients (44.4%) with probable IgG4-RD.
Serum IgG4 level was elevated (>135 mg/dL) in 14 patients (51.9%). Biopsy of the involved organ was performed in 20 patients (74.0%) of whom 16 of them had typical features suggestive of IgG4-RD.
Of all the patients, 11 (40.7%) were primarily treated with steroids and azathioprine, 8 (29.6%) with steroids and MMF combination, 5 (18.5%) were on a combination of methotrexate and steroids, while 3 (11.1%) were on steroids alone (Figure 1).
Primary Treatment in the Study Population.

A total dose of RTX given to patients has been shown in Figure 2. Majority of patients (96.3%) received an induction dose of 1g + 1g at an interval of 15 days. Only one patient, owing to very low body weight, received an induction dose of 500 mg + 500 mg at an interval of 15 days. Furthermore, 10 patients required maintenance treatment with RTX; four patients required one dose at the end of 6 months; five patients requiring two maintenance doses at 6 and 12 months; and one patient received three maintenance doses at 6, 12 and 18 months. Maintenance doses were decided based on overall clinical response, persistence of disease activity or elevated IgG4 levels as assessed at 6 monthly intervals.
Total Dose of Rituximab Administered to the Study Patients.

Of the 27 patients, one patient expired, which was unrelated to the illness and two patients were lost to follow-up. Out of 24 patients who had received RTX, steroids could be withdrawn from 9 (37.5%) and DMARDs and steroids were both discontinued in four patients. Among the nine patients who could tolerate the withdrawal of steroids, eight had orbital and periorbital involvement. The average duration after which steroids or DMARDs were withdrawn was azathioprine (17.2 months), MMF (7.7 months), methotrexate (15.6 months) and steroids (9.3 months).
Out of 14 patients with elevated IgG4 levels, post RTX infusion, IgG4 levels normalised in six patients, while a significant reduction in IgG4 level was noted in one patient, however, it was not within normal limits. The remaining seven patients showed a marginal reduction in IgG4 levels as compared to the baseline value (Figure 3).
Response to Treatment.

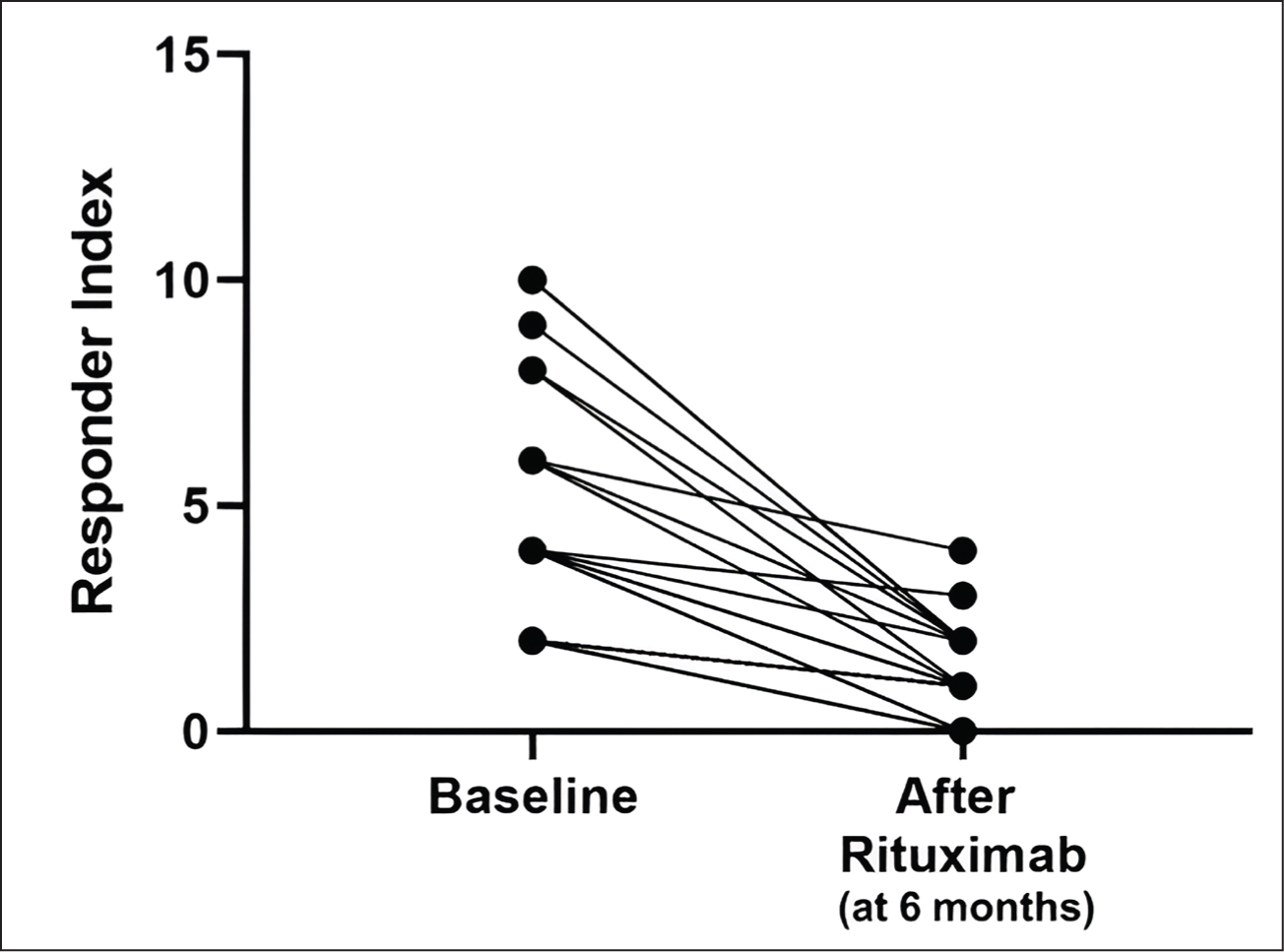
Serious adverse events to RTX were defined as adverse events requiring hospitalisation that were accountable to the use of RTX. No such adverse events were noted in any of the patient in our study. One patient experienced a relapse of disease after 2 years of RTX infusion. However, this patient was not compliant with his maintenance treatment. Response to treatment with RTX was also calculated using RI (Figure 4). The average RI before RTX was started was 4.79 (2–10); while the average RI after treatment with RTX was 1.33 (0–4).
Response to Treatment Using Responder Index.
In the subgroup analysis, the difference in terms of IgG4 levels or RI between the group with normal IgG4 levels was compared with those with elevated IgG4 levels.
As shown in Table 2, in IgG4: WNL group, the change in mean IgG4 levels from pre-treatment timepoint to post-treatment timepoint was not statistically significant (Wilcoxon test: V = 50.0, P = .780). Whereas in the IgG4: high group, this change was statistically significant (Wilcoxon test: V = 66.0, P = <.001). The overall change in IgG4 levels over time showed a significant difference in the trend of IgG4 levels over time between the two groups (P = <.001).
Comparison of the Two Groups in Terms of Change in IgG4 Levels Over Time.

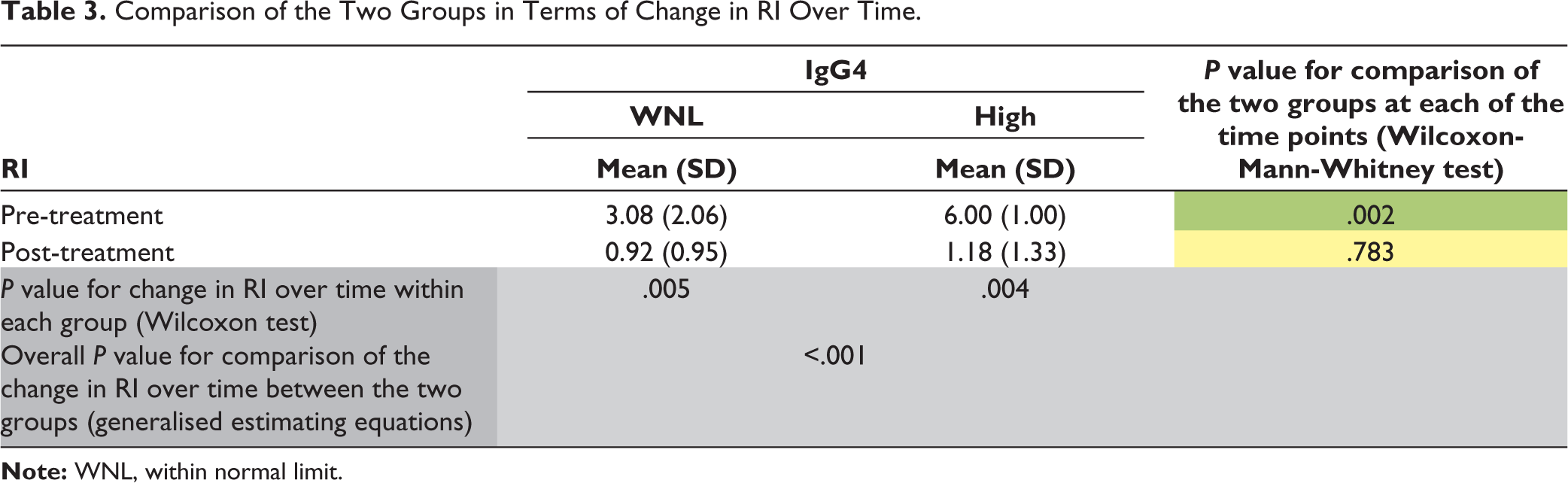
With regards to RI, as shown in Table 3, in IgG4: WNL group versus IgG4: high group, the mean change in RI from pre-treatment timepoint to post-treatment timepoint was statistically significant (Wilcoxon test: V = 75.0 vs. 66.0, P = .005 vs. .004). The overall change in RI over time in the two groups was significant (P = <.001).
Comparison of the Two Groups in Terms of Change in RI Over Time.
Discussion
To the best of our knowledge, this is the largest series from India to study the role of RTX in the management of IgG4-related diseases. Apart from this, there are only a few studies from all across the world and a few case series which have shown the benefit of RTX in IgG4-related disease.
In our study, out of a total of 27 participants, 14 were men, and 13 were women, resulting in a nearly equal gender distribution. In contrast, in Western literature, there is a higher incidence of IgG4-RD in males compared to females, with ratios ranging from 1.3 to 3.2:1. 15
The most frequently affected organ in our study were the orbit and periorbital tissue, followed by retroperitoneum. In contrast, Carruthers et al.’s study (USA) identified major salivary glands as the most common organ involved, followed by ophthalmic manifestation. 6 This variance could be attributed to referral bias within our institution, as many patients were referred from the ophthalmology department. Notably, our cohort did not encompass autoimmune pancreatitis reflecting a lack of referral from the gastroenterology department. Remarkably, one of our patients showed the base of skull involvement, a rare manifestation of IgG4-RD with limited case reports. Typically, such involvement is confined to the skull base and calvarium, although concurrent involvement of the spine and other systems has been documented. Challenges associated with obtaining biopsies from the base of the skull may contribute to diagnostic difficulties or delays. Cler et al. reported two cases of the base of skull involvement treated predominantly with corticosteroids, resulting in significant clinical improvement. 7 Other organs involved were the parotid gland, genitourinary system and sinuses.
Twenty patients in our study had undergone biopsies of the involved organ; 15% of these patients were diagnosed as definite IgG4-RD, 41% were possible and 44% were probable cases of IgG4-RD, respectively. The primary treatment in our patient cohort involved a combination of steroids and azathioprine (11 cases), followed by steroids with mycophenolate mofetil (MMF, eight cases), and methotrexate (five cases). In contrast, the Carruthers et al. study reported that the majority of their patients received corticosteroids alone, with only a small number undergoing treatment with other DMARDs, including MMF (three cases), azathioprine (three cases), methotrexate (one case), and RTX (six cases). This divergence suggests a potentially more refractory nature of the disease in our study, highlighting the significance of RTX in managing difficult or resistant cases.
Accumulating experimental evidence suggests a pivotal role for B lymphocytes in the development of IgG4-RD. This is attributed to their secretion of functional autoantibodies, provision of survival signals for potentially harmful CD4+ cytotoxic T cells, and direct involvement in distinctive tissue fibrosis. RTX, through B-cell depletion, disrupts these pathogenic mechanisms, resulting in rapid clinical remission for the majority of patients. 8
The absence of sufficient data on the use of RTX in managing IgG4-RD, particularly in the Indian context, contributes to the existing knowledge gap. With a lack of definitive guidelines for the management of IgG4-RD, uncertainty persists regarding the optimal timing and dosage of RTX administration for these patients. In our study, the majority of enrolled patients had previously undergone treatment with steroids or alternative immunosuppressive agents before receiving RTX. Notably, two patients were directly considered for RTX infusion alongside corticosteroids without prior exposure to other treatments, of which one had extensive renal involvement while the other one had involvement of the base of the skull.
All patients underwent an induction phase with 1g of RTX, followed by a second dose of 1g administered 15 days later except for one patient who received an induction dose of 500 mg + 500 mg at an interval of 15 days. Maintenance RTX was employed in 10 patients who exhibited an insufficient clinical response during the induction therapy with RTX. Within this subgroup, four patients received a single dose of RTX at the end of 6 months, five patients received two doses of maintenance RTX at 6 and 12 months, and one patient received three doses of maintenance RTX at the 6, 12, and 18 months. In the study by Carruthers et al., re-treatment with RTX was needed at 8 months for one patient, at 10 months for two patients, and at 1 year for another patient.
In a study conducted by Campochiaro et al., 14 patients underwent an induction regimen of RTX. Among these, seven patients received maintenance RTX solely in the event of disease relapse, while the remaining seven patients underwent scheduled maintenance therapy every 6 months. The group receiving regular maintenance therapy demonstrated a significantly lower relapse rate, suggesting that maintenance therapy with RTX could effectively prevent flares in IgG4-RD. 8 In our study, only one out of 24 patients experienced a flare, suggesting that RTX could be reserved for use as maintenance therapy as needed, either during flares or for those exhibiting an inadequate response to induction therapy. The need for RTX maintenance therapy in such cases requires further evaluation.
The response to RTX was noted in terms of the ability to withdraw steroids and other disease-modifying agents in IgG4 levels and by calculating IgG4RD- RI. Nine patients were able to discontinue steroids after RTX and 12 patients were maintained on low-dose steroids (<5 mg/day prednisolone equivalent), while seven patients achieved complete remission and were able to discontinue both steroids and DMARDs.
Among the 27 patients in our study, 14 showed elevated IgG4 levels, while 13 had normal levels. Surprisingly, after undergoing treatment with RTX, only six patients experienced a normalisation of IgG4 levels. This observation raises concern about the reliability of serum IgG4 concentrations as a marker for monitoring disease activity or diagnosing IgG4-RD. Similar results were documented in a study by Carruthers et al., where 37% of enrolled patients did not have elevated serum IgG4 levels at the study’s outset and in those with elevated IgG4 concentrations, levels did not normalise even after RTX treatment, despite achieving an overall excellent clinical response. Notably, compared to the 2012 IgG4-RD RI that included serum IgG4 in its calculation, it was excluded from the 2018 IgG4-RD RI.9,10 In contrast to our findings, the study by Khosroshahi et al. showed that IgG4 levels were a reliable marker of disease activity. It also showed that RTX provided prompt clinical and serologic improvement in all their 10 patients. 11
In our group, significant improvement in RI from that of baseline was noted, with six patients achieving complete clinical response (RI – 0). In our study, the improvement in RI was found to be significant in patients with both normal or increased serum IgG4 levels. A difference of two points was considered significant. Five patients failed to show this response despite having a significant clinical response. This raises queries about the reliability of RI in assessing actual response to treatment as it gives equal weightage to both clinical and serologic parameters. Yet, Bakhus et al. showed that the RI serves as a reliable indicator to evaluate disease activity and identify individuals with IgG4-RD who could potentially benefit from B-cell-depleting therapy. 12
The strength of our study is that it demonstrates the efficacy of B-cell depletion in IgG4RD, as nearly all patients exhibited a response to RTX. The effectiveness of RTX as an alternative option for managing refractory cases was evident, especially considering that a significant portion of our patients had previously undergone treatment with other DMARDs.
However, there are limitations to our study. It was a single-centre study with a relatively small sample size, potentially impacting the reliability of the results. Referral bias may have contributed to limited knowledge about the effects of RTX on manifestations beyond orbital disease. Additionally, being a retrospective study, not all data may be available which includes that of radiological imaging at follow up and regarding adverse events noted following RTX. Also, our study could not evaluate the upfront use of RTX during its period of study, though 2020 management guidelines offer more clarity to its use.
Conclusion
In conclusion, RTX emerges as a viable treatment alternative for individuals with refractory disease or those who are intolerant to steroids and/or DMARDs. However, the need for a maintenance dose of this drug needs more clarification. The reliability of serum IgG4 levels as an indicator of disease activity appears questionable; hence, both clinical and serological responses are essential while deciding whether to continue or to stop treatment. Further research is needed to evaluate the advantages of using RTX as a first-line agent in the Indian population in managing IgG4-RD and to establish comprehensive guidelines for its use in this context.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval for the study was obtained from the Ethics Committee of Sir Ganga Ram Hospital, New Delhi. Institutional review board approval ID – EC/08/17/1211.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Since the study was retrospective and involved no additional interventions beyond the routine treatment plan, patient consent was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.