
Abstract
Background:
Animal models studies show the role of interleukin-22 (IL-22) in the pathogenesis of enthesitis. We analysed an association of IL-22 levels with enthesitis in Enthesitis-related juvenile idiopathic arthritis (JIA-ERA) patients.
Methods:
Patients with JIA-ERA, polyarticular JIA (Poly-JIA), and healthy controls (HC) were enrolled. The frequencies of Th1, Th17 and Th22 cells in peripheral blood (PB) and synovial fluid (SF) were determined by flow cytometry, and IL-22 levels in SF by ELISA. Data is shown as median with interquartile range.
Results:
T-cell frequency was determined in 40 JIA-ERA (33 boys, 16 [3.3] years), 10 Poly-JIA (3 boys, 14.5 [6] years), and 10 HC (9 boys, 18 [2] years). Among 40 JIA-ERA patients, 28 had enthesitis. In JIA-ERA, Th1 cell frequency was significantly higher in SF (8.6 [4.5]) than in PB (2.9 [0.55]; P = 0.007). Th22 cell frequency in PB was higher in active JIA-ERA patients as (0.2 [0.1]; JSpADA >2.5) compared to the inactive disease (0.15 [0.18]; P = 0.02). No association was observed between Th22 cell frequency and enthesitis.
No difference in serum IL-22 levels of 85 JIA-ERA (78 boys, 16 [4] years), 13 Poly-JIA (4 boys, 12 [7.5] years), and 31 HC (27 boys, 25 [8] years) was observed. SF showed higher IL-22 levels than corresponding serum samples (P = 0.04).
Conclusion:
High SF levels of IL-22 suggests its role in inflammation in JIA-ERA patients. The lack of association of PB Th22 cell frequency with enthesitis suggests that immune abnormalities at local site may not be reflected in PB.
Introduction
A category of juvenile idiopathic arthritis (JIA) called enthesitis-related arthritis (ERA) comprises patients with asymmetrical lower limb arthritis and is usually observed in boys older than 6 years of age. The other features include enthesitis, tarsitis, and acute anterior uveitis. Over time, children with JIA-ERA develop spine involvement as lower backache and clinical and radiological sacroiliitis. 1 About 70–75% of these children are HLA-B27 positive. 2 The JIA-ERA disease has a resemblance with adult spondyloarthropathies (SpA).
Entheses are specialised areas where tendons are attached to the bone and inflammation of entheses is referred to as enthesitis. 1 Enthesitis is often considered a hallmark of SpA but its pathogenesis remains elusive. An animal model expressing minicircle DNA (mcDNA) of interleukin-23 (IL-23) developed features of SpA such as enthesitis, arthritis, aortic inflammation and spine disease, suggesting that IL-23 is the key driver of inflammation in SpA. 3 Further, it was seen, that enthesitis was not mediated by IL-17 but by IL-23 induced IL-22 production. Thus, IL-22 seems to be an important cytokine for the development of enthesitis. In the same model, double negative T cells (CD3+CD4-CD8-) were shown to produce IL-22 in the vicinity of entheseal sites. 3 Later, γδ T cell ( Vγ6+CD27) present in entheses vicinity indicates a major role for innate immune pathways in the pathogenesis of enthesitis.4,5
IL-22 (IL-10 family of cytokine) uses IL-10 receptor 2 for signal transduction. 6 The IL-22 cytokine is produced by the immune cell but has very little effect on the immune cells. In humans, IL-22 is produced by immune cells such as NK (natural killer), NK-T cells, T cells, and innate lymphoid cells (ILCs). Its major effect is in epithelial cells in the gut, skin, and other mucosal sites, and it helps in maintaining barrier integrity. 6 The CD4+ T cells that produce IL-22 are termed as Th22 cells. 6
There is limited human data on IL-22 in rheumatic diseases. Variation in IL-22 gene copy number is linked with ankylosing spondylitis 7 and also to enthesitis and formation of new bone in SpA. 8 In Psoriasis, skin biopsies showed an increase mRNA expression of IL-22 in the dermis, which got normalised with cyclosporin treatment. 9 Further, serum levels of IL-22 were elevated in patients with psoriasis, and serum levels correlated with disease activity. 10 In patients with psoriasis, the synovial fluid level of CXCL4 strongly correlated with IL-22, suggesting that CXCL4 drives IL-22 production in immune cells. 11 In Crohn’s disease, IL-22-producing T-cells and T cells producing IL-22 are increased in inflamed mucosa and the disease activity correlates with IL-22 in serum. 12 Though IL-22 has a limited effect on fibroblasts, synovial fibroblasts from patients with rheumatoid arthritis (RA) produced receptor activator of nuclear factor κ B ligand (RANKL), alarmins, and chemokines in response to IL-22.13,14 In addition, IL-22 was associated with radiographic progression in RA, suggesting its role in inflammation. 15
Since IL-22 is the major mediator of enthesitis in an animal model of SpA and enthesitis is a major component of JIA-ERA, we decided to study the involvement of IL-22 in JIA-ERA. Our main objective was to see whether the level of IL-22 in serum or synovial fluid (SF) and the frequency of Th22 cells in peripheral blood or SF in patients with JIA-ERA are higher than those in healthy controls (HC) and its correlation with enthesitis.
Methods
Patients
Patients satisfying the International League of Associations for Rheumatology (ILAR) criteria, who were diagnosed with JIA-ERA were included in the study. 1 Patients having signs or symptoms suggestive of infection were excluded. Blood samples were collected from all patients and paired synovial fluids (SF) were collected from patients requiring aspiration of joint for intra-articular corticosteroid injection. Disease activity measurement was done by Juvenile Spondyloarthropathy Disease Activity Score (JSpADA), 16 and the enthesitis score was measured by the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES) index. Children with JSpADA scores >2.5 were classified as active disease. The patients with polyarticular JIA (Poly JIA) and healthy young adults were included as controls. The study was ethically approved by the SGPGIMS Ethics Committee (IEC number 2016-49-IMP-EXP dated September 14, 2016) and all patients and/or their guardians gave informed consent.
Frequency of IL-22 Producing T Cell by Flow Cytometry
Peripheral blood mononuclear cells (PBMC) and synovial fluid mononuclear cells (SFMC) were separated from PB and SF, respectively, using density gradient centrifugation. One million PBMC or SFMC were cultured in Rosewell Park Memorial Institute (RPMI) medium completed with 1% antibiotic-antimycotic mix (Gibco, Thermo-Fischer Scientific, USA) and 10% foetal bovine serum (FBS). Cells were treated with phorbol myristate acetate (PMA; 50 ng/mL, Sigma, USA)/ Ionomycin (1 µg/mL, Sigma, USA) and Golgi plug, Brefeldin A (10 µg/mL, Sigma, USA) for 6 h at 37 ºC in CO2 incubator.
To IL-17 and IL-22 producing CD4+ T cell frequency was determined by surface staining (30 min) with FITC mouse anti-human CD3 (UCHT1 clone) and PE mouse anti-human CD4 (RPA-T4 clone) antibodies (BD Biosciences, USA) was done. After fixation and permeabilisation, cells were treated with cytofix/cytoperm buffer (BD Biosciences, USA) for 20 min and intracellular staining (30 min) was done using APC mouse anti-human IL-22 (IL22JOP clone, eBioscience, USA) and PerCP-Cy 5.5 mouse anti-human IL-17 (N49-653 clone, BD Biosciences, USA) antibodies. To see for adequate stimulation of cells and for IFNγ+ T cell frequency, in a separate tube surface staining with FITC mouse anti-human CD4 (SK3 clone) antibody (BD Biosciences, USA) and after permeabilisation intracellular staining with PE mouse anti-human interferon-gamma (IFNγ) (4S.B3 clone, BD Biosciences, USA) was done. All incubations were done at room temperature in dark. Samples (200,000 cells) were acquired in BD biosciences Canto II flow cytometer and data analysis was performed by BD FACS Diva software (version 6.1.3, BD Biosciences, USA). We determined Th1 cell (CD4+IFNγ+) frequency in the lymphocyte gate and Th17 cell (CD3+CD4+IL-17+) and Th22 cell (CD3+CD4+IL-22+) frequencies were determined in CD3 gate (Supplementary Figure 1). Unstained tubes were taken as negative controls.
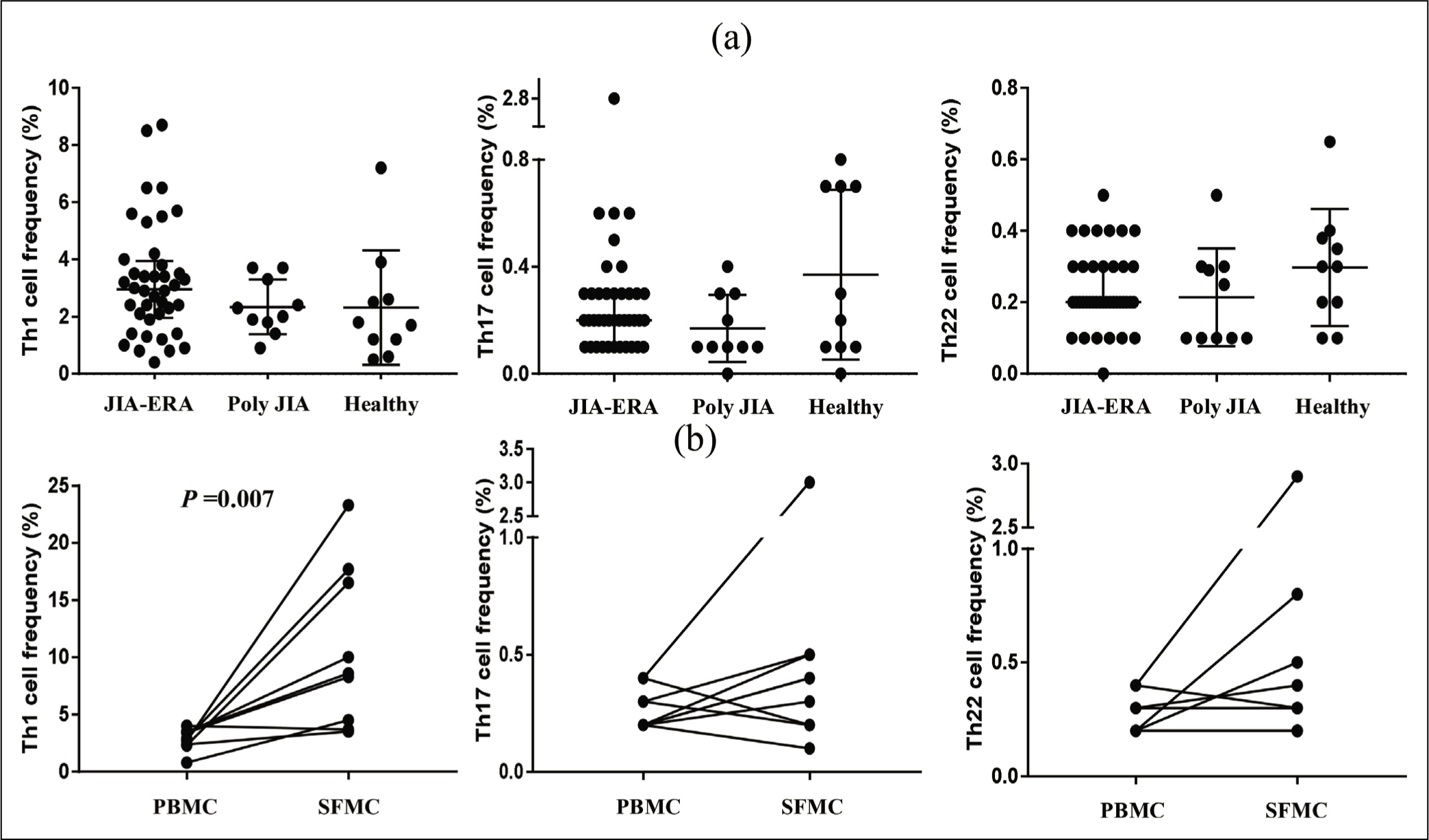
Frequencies of Th1, Th17 and Th22 cells in peripheral blood mononuclear cell cultures of (a) patient with juvenile idiopathic arthritis-enthesitis-related arthritis (JIA-ERA, n = 40), Polyarticular Juvenile Idiopathic Arthritis (n = 10) and healthy control (n = 10) (Mann–Whitney U test) and Th1, Th17 and Th22 frequencies in paired, peripheral blood mononuclear cell and synovial fluid mononuclear cell (n = 9) cultured samples of JIA-ERA patient (Wilcoxon signed rank test) by flow cytometry.
Serum and Synovial Fluid Levels of IL-22
Synovial fluid was centrifuged (1800 rpm x 10 min) and the supernatants were collected as cell-free SF and stored at –80 ºC until analysed. The serum was separated from clotted blood and stored at -80 ºC. In addition to samples from patients in this study, previously stored serum and SF samples from JIA-ERA patients, HC, and disease controls (Poly JIA) were also used. Serum and cell-free SF were analysed for IL-22 levels, using a sandwich enzyme-linked immunosorbent assay (ELISA) kit (Thermo-Fisher Scientific, USA) following manufacturers’ recommendations. The minimum detection limit of the assay was 6.55 pg/mL. Synergy H1 hybrid multi-mode microplate reader (BioTek, USA) was used to measure absorbance at 450 nm, and cytokine concentration was calculated using Gen5 data analysis software.
Statistical Analysis
Statistical analysis was done using SPSS 16.0 (SPSS Inc., USA). Non-parametric tests were used as the data was not distributed normally (by the Shapiro-Wilk test). The difference in frequencies of T cell subsets and serum IL-22 levels in JIA-ERA, Poly JIA, and HC samples was determined by Mann–Whitney U test. The Th22 cell frequencies in low and high disease activity patients were also compared by the Mann–Whitney U test . In paired samples (serum and SF) IL-22 levels of JIA-ERA patients were analysed by Wilcoxon signed rank test. Serum levels of IL-22 and Th22 cell frequency in the peripheral blood of JIA-ERA patients with or without enthesitis, sacroiliitis, and arthritis were compared by Mann–Whitney U test . The correlation of IL-22 levels in serum and SF was done by Spearman’s rank correlation test. P value <0.05 was contemplated as significant. Data are presented as median with interquartile range (IQR).
Results
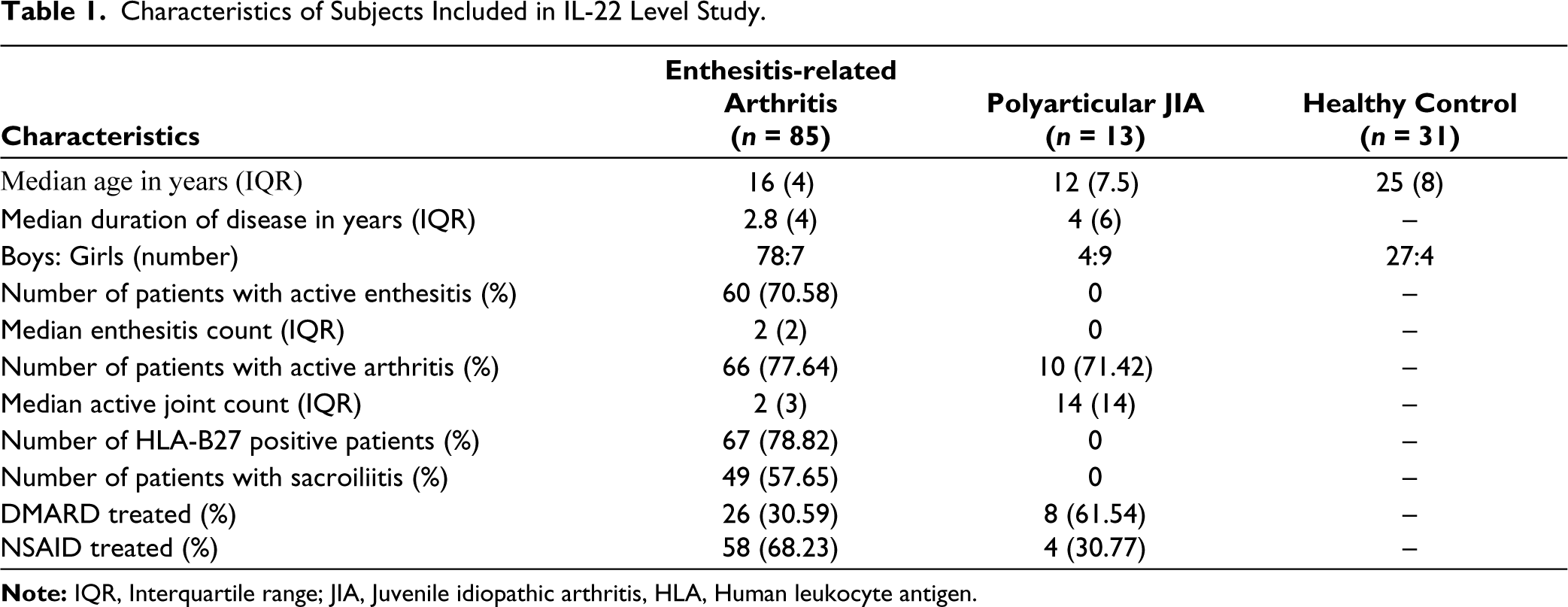
A total of 85 children with JIA-ERA, 13 with Poly-JIA and 31 HC, were enrolled in the study. The children with JIA-ERA had a median age of 16 years and a median disease duration of 2.8 years. Most were boys and 67 of them were HLA B27 positive. Nearly one-third were on DMARDs (Methotrexate or sulphasalazine). No patient was on biologic therapy (Table 1).
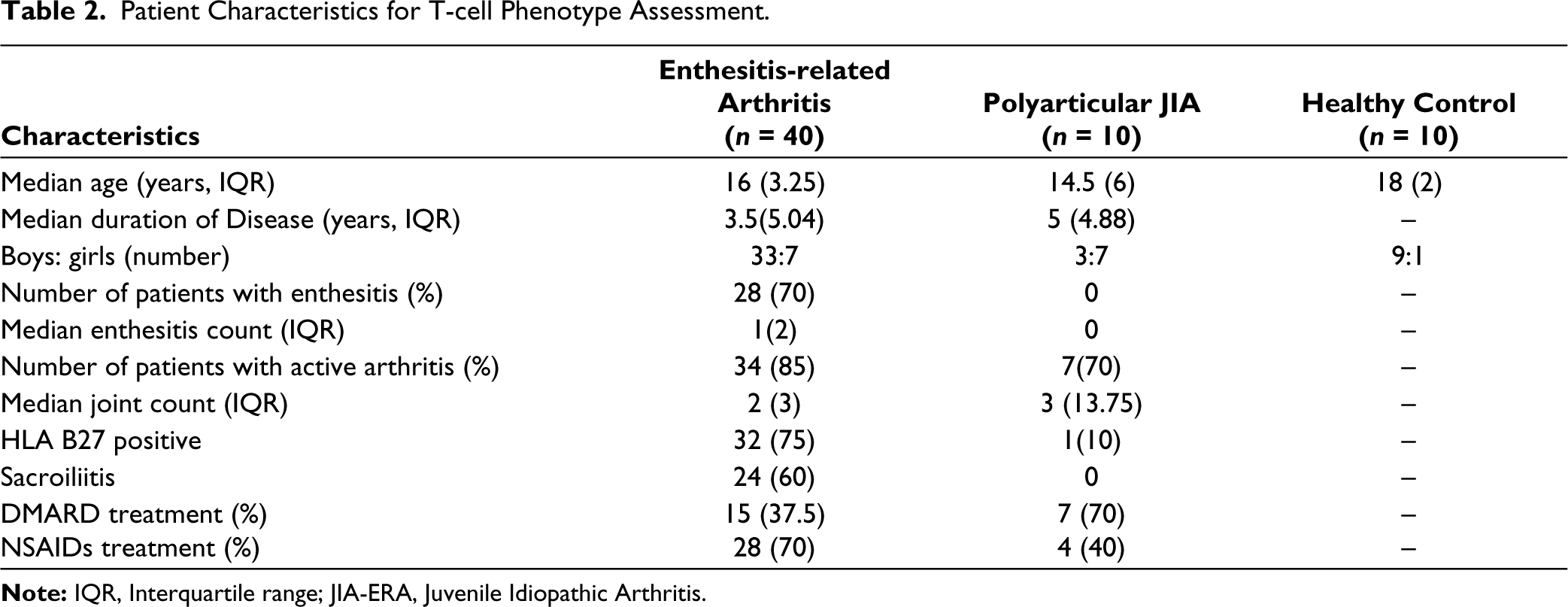
Among these cellular studies were done in 40 children with JIA-ERA, 10 with Poly JIA, and 10 HC. Among 40 JIA-ERA patients, 15 were treated with disease-modifying anti-rheumatic drugs (DMARD: mainly methotrexate or sulfasalazine). Most patients had the active disease (Table 2). The frequencies of Th1, Th17 and Th22 cells were comparable in PB in the three groups (Figure 1). On analysing paired samples, Th1, Th17, and Th22 cell frequencies were higher in SF than PB but only the Th1 cell frequency reached statistical significance (SF 8.6 [4.5], PB 2.9 [0.55]; P = 0.007; Figure 1).
Characteristics of Subjects Included in IL-22 Level Study.
Patient Characteristics for T-cell Phenotype Assessment.
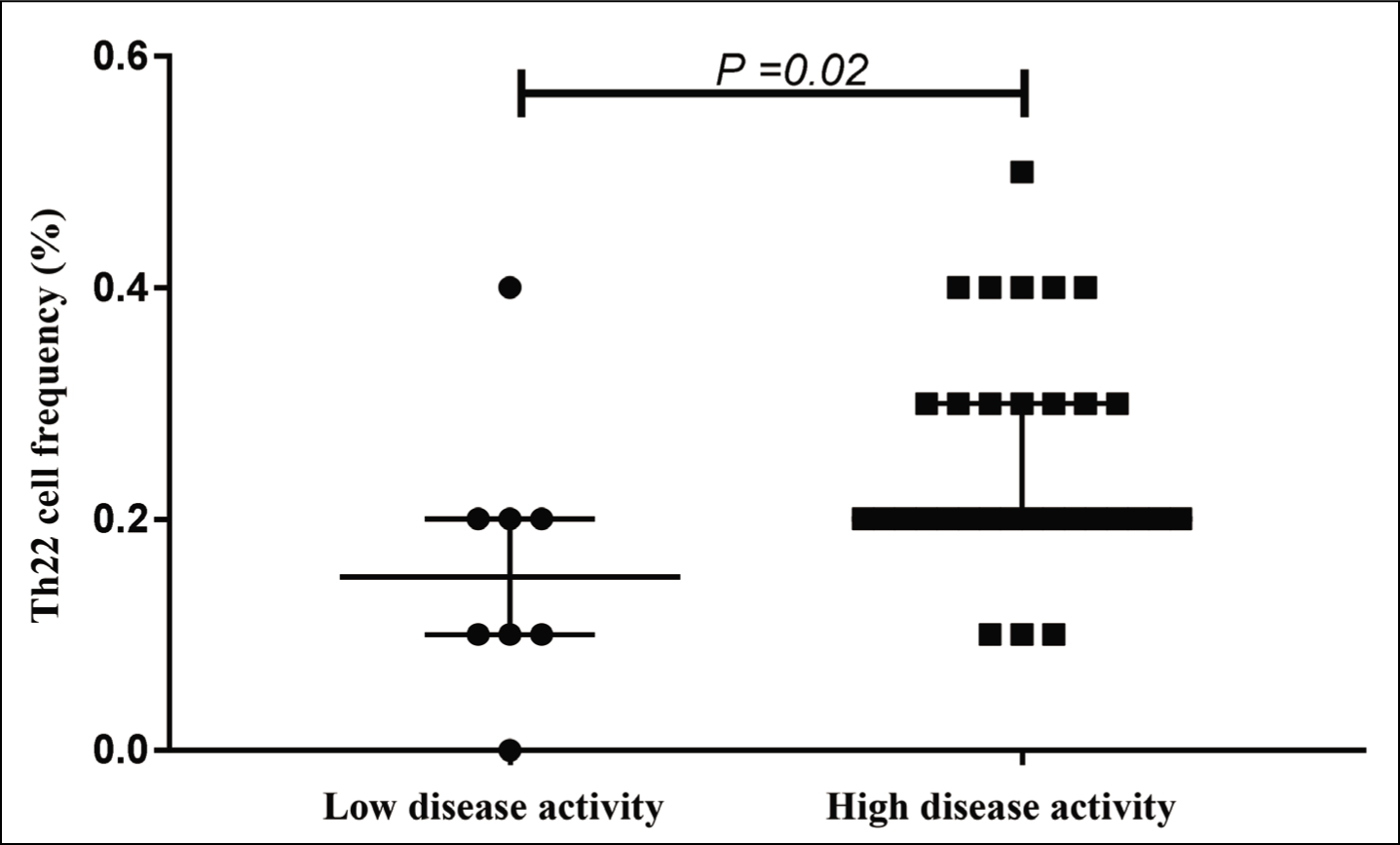
Children with active disease had higher median (IQR) frequency of Th22 cells in PB (0.2 [0.1]) as compared to those with inactive/minimally active forms of the disease (0.15 [0.18], P = 0.02; Figure 2). The Th22 cell frequencies in PB of JIA-ERA patients with or without enthesitis (0.2 [0.1] vs 0.2 [0.1], Supplementary Figure 2a), arthritis (0.2 [0.1] vs 0.2 [0.13], Supplementary Figure 3a) or sacroiliitis (0.2 [0.1] vs 0.2 [0.25], Supplementary Figure 4a) was not different.
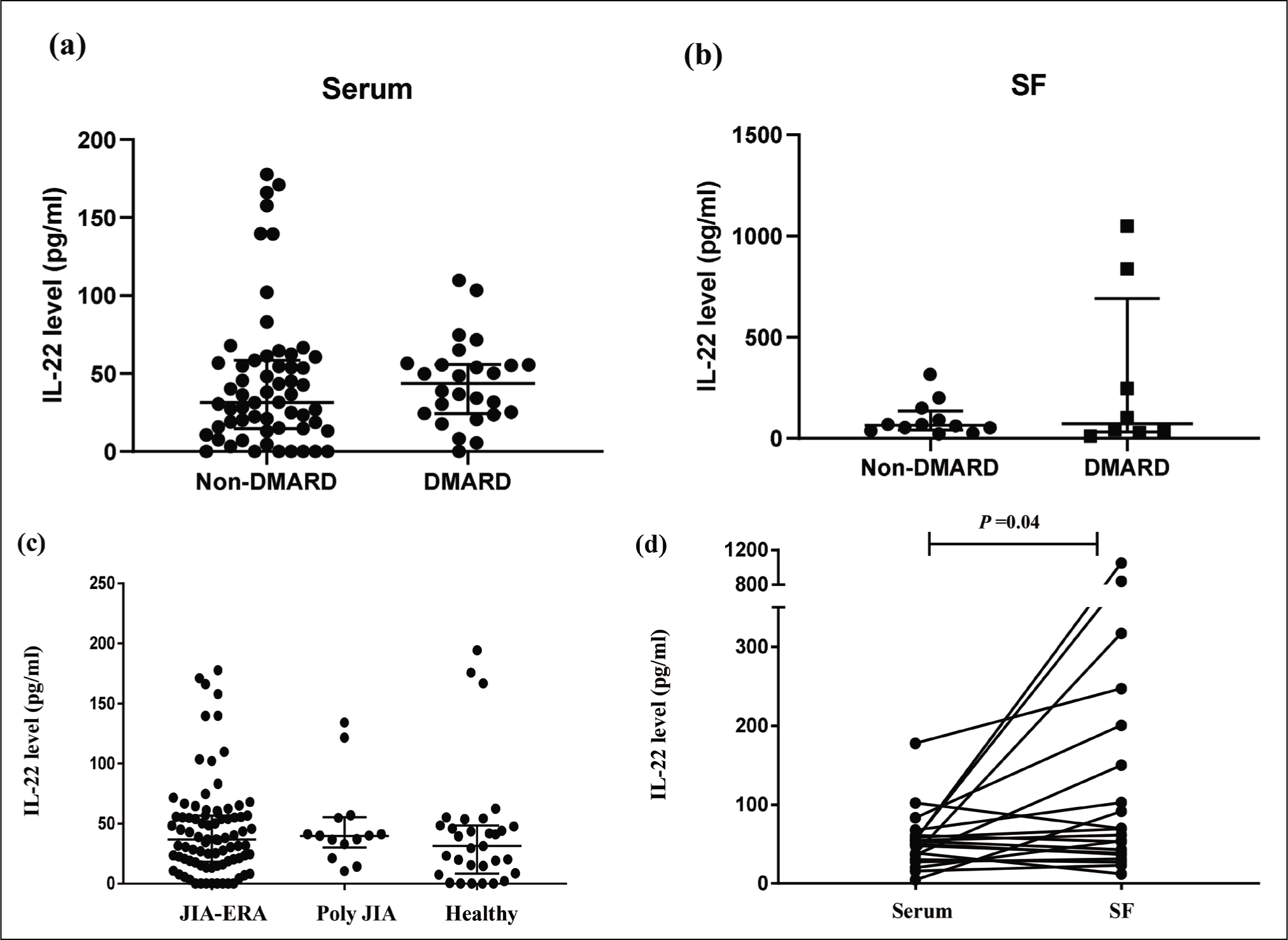
Measurement of levels of IL-22 levels in serum samples of 85 children with JIA-ERA (78 boys), 13 Poly JIA (4 boys), and 31 HC (27 boys) was done by ELISA (Table 1). Among 85 JIA-ERA patients, 26 were treated with DMARD (methotrexate, sulfasalazine, or leflunomide), 58 patients with NSAIDs and 20 patients with both. In the Poly JIA group, 8 were treated with DMARD, 4 patients with NSAIDs and 2 patients with both. We did not observe any difference in IL-22 levels in serum and SF of DMARD treated as compared to non-DMARD treated JIA-ERA patients (Figure 3a and b). No significant difference was observed in IL-22 levels among JIA-ERA, Poly-JIA and HC groups (Figure 3c). As compared to the serum sample, IL-22 levels were higher in SF (65.5 [113.4] pg/mL [SF], 52 [27.9] pg/mL [serum]; P = 0.04; Figure 3d). SF IL-22 levels correlated positively with serum levels (P < 0.05, r = 0.46). The IL-22 serum levels were not different in JIA-ERA patients with or without enthesitis (36.22 [39.11] pg/mL vs 43.46 [41.26] pg/mL; Supplementary Figure 2b).
Frequencies of Th22 cells in peripheral blood mononuclear cell culture of Juvenile Idiopathic Arthritis–Enthesitis Related Arthritis patients with low (n = 8) and high (n = 32) disease activity (Mann–Whitney U test).
No correlation was observed between serum IL-22 levels and frequencies of Th17 or Th22 cells. The blood Th22 cell frequencies and serum IL-22 levels were similar in those with or without arthritis (36.76 [36.62] pg/mL vs 30.56 [53.39] pg/mL) and sacroiliitis (26.92 [38.03] pg/mL vs 49.04 [39.69] pg/mL; Supplementary Figures 3b and 4b, respectively).
Measurement of IL-22 levels in (a) serum (n = 85) and (b) synovial fluid (n = 20) of Juvenile Idiopathic Arthritis-Enthesitis Related Arthritis patients treated with and without DMARD (Mann–Whitney U test). (c) Estimation of levels of IL-22 (pg/mL) in serum sample of patient with juvenile idiopathic arthritis-enthesitis-related arthritis (JIA-ERA, n = 85), Polyarticular Juvenile Idiopathic Arthritis (Poly JIA, n = 14) and healthy control (n = 31) measured by enzyme-linked immunosorbent assay (Mann–Whitney U test), (d) IL-22 levels in paired sample (n = 20) (serum and synovial fluid) of patients with JIA-ERA (Wilcoxon signed rank test).
Discussion
The peripheral blood Th22 cell frequencies and serum IL-22 levels in our JIA-ERA patients were not different from those in healthy subjects. Nonetheless, compared to patients with inactive or minimal disease, JIA-ERA patients with active disease showed a higher frequency of Th22 cells in PB.
Our findings are different from a previous report in SpA 17 wherein the IL-22 level and Th22 cell frequency were higher in AS patients than in healthy subjects, but they did not find any association with disease activity. 22 No data is however available for JIA and ours is the first study to look at the IL-22 level and Th22 cell frequency in JIA-ERA. A previous study in JIA had only shown that Th17 cells also produce IL-22. 18
Mechanical stress, microtrauma or microbial products can induce production of IL-23 from monocytes of these patients, which in turn, may lead to production of IL-22 at the local site. Lack of association of enthesitis with blood Th22 cell frequency or serum IL-22 level could mean that local (at entheseal site) production of IL-22 is not reflected in blood. The other reason could be that, in contrast to mouse models, IL-22 may not play a significant role in enthesitis in humans.
Level of IL-22 was significantly higher in SF as compared to serum. The Th22 cell frequency was also higher in SF, though it was not statistically significant. This suggests that IL-22 could be playing a role in inflammation associated with JIA-ERA. Newer antibodies like Fezakinumab that target IL-22 or drugs like Losartan that inhibit IL-22 production may therefore have a role in the treatment of JIA-ERA.19,20
We did not find any association between Th17 cell frequency and IL-22 levels. In patients with RA, serum IL-22 level has shown an association with Th17 cell (major producer of IL-22) and Th22 cell frequency. 21 Besides Th22 and Th17 cell, NK cell also produces IL-22, group 3 ILC, and γδ T cells.3,22 Indeed, in ERA pathogenesis innate immune cells seem to play a major role. 23
The study provides data on IL-22 levels and Th22 cell frequency in PB as well as SF in a large number of JIA-ERA patients, which has been studied less often. Limitations of the study are the inclusion of patients receiving drugs like methotrexate. A study shows that 12 weeks of treatment with MTX+ leflunomide significantly reduces Th22 frequency and IL-22 plasma levels in rheumatoid arthritis. 24 However, we did not observe any difference in IL-22 serum and SF levels of patients with JIA-ERA treated with or without DMARD. The number of paired samples is small.
To conclude, IL-22 apparently contributes to synovial inflammation in JIA-ERA. However, the lack of association of level of IL-22 or frequency of Th22 cells with enthesitis suggests that peripheral blood might not be the ideal site to look for abnormalities associated with enthesis. Study of cells or bursal fluid in the vicinity of entheses may help in discerning the role of IL-22 in enthesitis in humans. In addition, a study with recruitment of treatment naïve JIA-ERA patients may better predict an association of IL-22 with enthesitis.
Supplementary Material
The supplementary material for this article is available online.
Footnotes
Acknowledgements
We thank Dr Sudhir Sinha for the critical review of the manuscript. The project was funded by an intramural research grant to AA and AS received a Senior Research Fellowship from the Indian Council of Medical Research.
Author Contributions
AS performed key experiments and data analyses.
SK helped in patient recruitment, clinical data collection and analyses.
AA and RNM designed the experiments.
All authors discussed data, wrote and commented on the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The ethical approval was provided by the Institutional Ethics Committee of SGPGIMS (IEC Number 2016-49-IMP-EXP dated 14 September 2016).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was taken from legal guardians and patients as applicable
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.