
Abstract
Objective:
There is complete absence of sexual maturity data on patients afflicted with juvenile dermatomyositis (JDMS) from the Indian subcontinent. Hence, this study aimed to unfold the effect of this disease on the sexual development of JDMS children.
Methods:
In the Growth Laboratory/Clinic of the Department of Pediatrics, 60 (25 male and 35 female) sexual maturity-related observations were made on 35 JDMS patients, aged 10–17 years, enrolled from the Pediatric Rheumatology Clinic. Breast development stage and age of onset of menarche were recorded among female patients. In male patients, besides, determining the genitalia development stage, measurement of stretched penile length and testicular volume was done. Appearance of pubic and axillary hair among JDMS patients of both sexes was recorded.
Results:
Most girls with JDMS (34.28%) were in breast development stage-B2 (mean age 10.91 ± 1.08 years) and 22.86% had attained menarche. However, breast stage B5 was attained at 14.62 ± 1.06 years. JDMS girls reached stage B2 at the same age as their normal healthy counterparts. Onset of menarche was delayed by almost a year in JDMS girls. Age of attainment of genitalia stage G2 in JDMS boys (12 years) was delayed by 6 months as compared to well-off Chandigarh boys (11.5 years), whereas it was advanced by 1.5 years when contrasted with affluent Indian counterparts (13.3 years).
Conclusion:
Comparable pubertal attainments in JDMS males and somewhat delayed start of menarche in female JDMS patients as compared to their normal counterparts show that disease activity has a smaller effect on the sexual development of JDMS patients from north-western India.
Introduction
Juvenile dermatomyositis (JDMS) is a multisystem illness with an unknown aetiology that causes non-suppurative inflammation of striated muscle and skin, 1 increasing muscular weakening, and cutaneous rash and ulcerations, 2 presenting with a variety of complications and associations. Although this condition is relatively rare, with an annual incidence of 2–4 per million, it is the most frequent inflammatory myopathy in children, accounting for around 6% of children with severe connective tissue diseases in paediatric rheumatology clinics. 2 JDMS is more common in females and has been found to affect children of White ethnicity more frequently than those of other ethnicities. 3 The long-term consequence of JDMS is becoming increasingly important. Modern immunosuppressive treatments have dramatically increased survival rates, lowering active symptoms from 3.5 to 1.5 years. 4 However, JDMS can still have an impact on patients’ physical development, sexual maturation, and psychosocial well-being. 5 Until now, only one study has described the pubertal status of children with JDMS, 2 and there is no information on the effect of this disease on the pattern of pubertal attainments of JDMS patients from the Indian subcontinent. Due to the rarity of this condition and the scarcity of information, an attempt was made to investigate the sexual maturity of Indian boys and girls with JDMS.
Materials and Methods
A total of 60 observations made on 35 subjects, aged 10–17 years, diagnosed with JDMS according to Bohan and Peter’s (1975) criteria 1 and born to the parents representing mixed-socioeconomic strata served as actual database to achieve the study’s objectives. These children were enrolled in the Pediatric Rheumatology Clinic of the Department which they attend to seek regular treatment after taking informed written consent from either of the parent and assent from the participant. Each individual was examined for various signs of sexual maturity in the Department’s Growth Laboratory/Clinic at enrolment and after a 6-month age interval. Information on disease duration and disease activity as measured by the Manual Muscle Testing (MMT-8) score was recorded. The Institutional Ethics Committee of PGIMER approved the study, which was conducted from January 2021 to June 2022.
Pubertal assessment of male and female JDMS patients was performed using Tanner’s Sexual Maturation Scale 6 in a separate room of the Growth Laboratory, in the presence of either parent or guardian, as well as another laboratory staff member of the same gender posted in the unit. In the case of female subjects, information about the various stages of breast development (B1–B5) as well as the age at which menarche occurred was recorded. In the case of male subjects, information on genital staging (G1–G5), testicular volume (TV), and stretched penile length (SPL) was recorded. Prader’s Orchidometer was used to estimate testicular volume, and a sliding calliper (GPM, Swiss brand; least count: ± 1 mm) was used to measure the stretched penile length in the flaccid state. The presence of pubic and axillary hair in JDMS patients of both sexes was documented.
Statistical Analysis
Our data were skewed, and the sample size for each age group was limited, thus it was expressed as mean, standard deviation, median, and interquartile range. Categorical variables were reported using counts and percentages. The Spearman correlation coefficient was calculated to see the relationship between different quantitative data sets. Categorical data were compared using either the chi-square test or Fisher’s exact test, depending on their applicability. P values <0.05 were considered significant. The analysis was performed using IBM SPSS STATISTICS version 22.0.
Results
Mean age of attainment of menarche among JDMS girls (n = 35) was at 13.75 ± 1.38 years. The minimum and maximum age at which menarche was attained by our subjects were at 12 years and 16 years, respectively. However, appearance of pubic hair and axillary hair preceded the attainment of menarche, at a mean age of 12.06 ± 2.01 years and 12.88 ± 1.90 years, respectively. Pubic hair was noted to be absent in 5 girls; likewise the absence of axillary hair was noticed among 17 girls with JDMS. Around 22.86% of our JDMS girls were still in the pre-pubertal stage of breast development, that is, stage B1, and the rest 77.14% were in an advanced stage of breast development. Our JDMS females entered puberty, that is, stage B2 of breast development at a mean age of 10.91 ± 1.08 years, and reached breast stage B5 at a mean age of 14.62 ± 1.06 years, respectively. Interestingly, none of our study participants were in breast development stage B4 during the course of this study (Table 1).
Mean, SD and Percent Attainment of Different stages of Breast Development (Girls) and Genitalia Stages (Boys) in JDMS Patients.
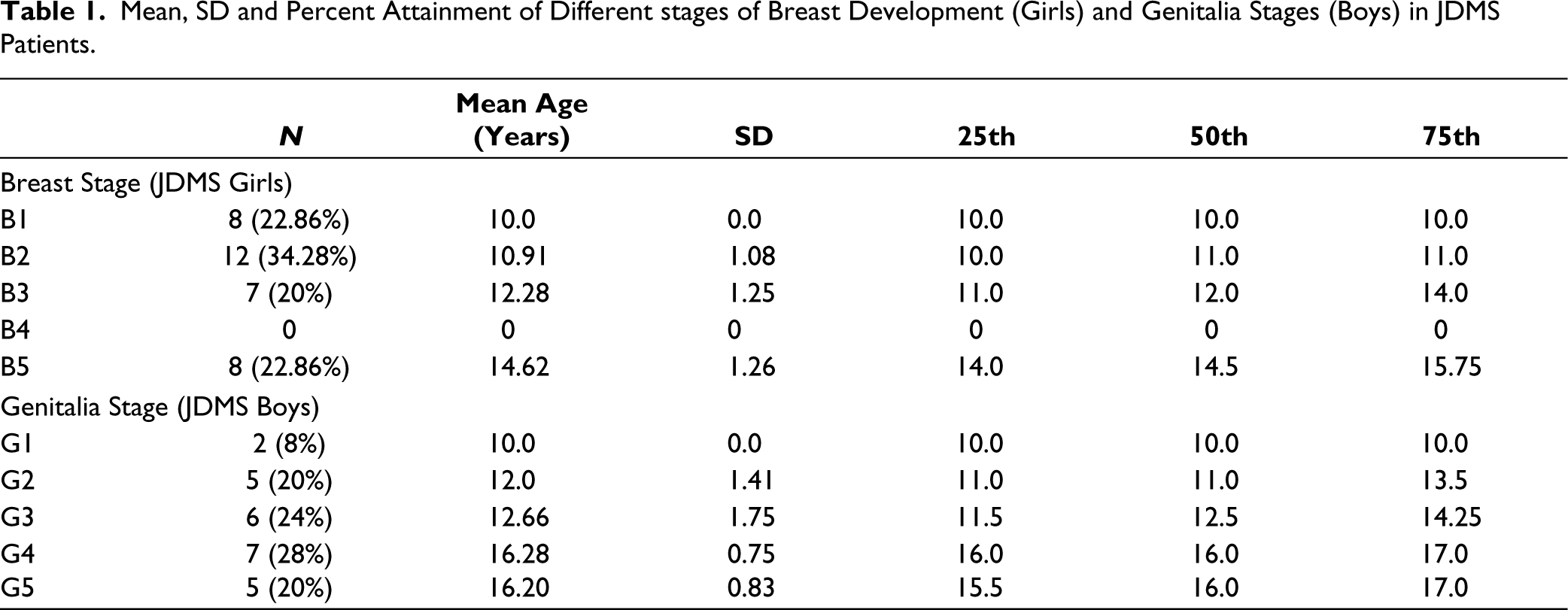
Among JDMS boys (n = 25), the mean age of appearance of pubic hair and axillary hair was noted to be 14.21 ± 2.53 years and 15.05 ± 2.07 years, respectively. It was also observed that pubic hair was absent in 8% of the JDMS boys, whereas the absence of axillary hair was noted among 28% of JDMS boys enrolled in our study. At an average age of 16.2 ± 0.83 years, 20% of JDMS males had reached adult genitalia stage, G-5. Approximately 8% of the participants were in the pre-pubertal stage of genitalia development (Stage G1) at a mean age of 10.0.
For our study boys, we observed a normal pattern of increase in testicular volume with age. A significant rise in testicular volume (bilateral) was observed between late adolescence (i.e., 16–17 years of age). In JDMS boys, the mean stretched penile length (SPL) increased from 3.83 ± 0.87 between 10–12 years and 6.79 ± 0.46 between 16–17 years (see Table 2).
Mean, SD of Testicular Volume-Right Side (TV-R), Testicular Volume- Left Side (TV-L) and SPL.

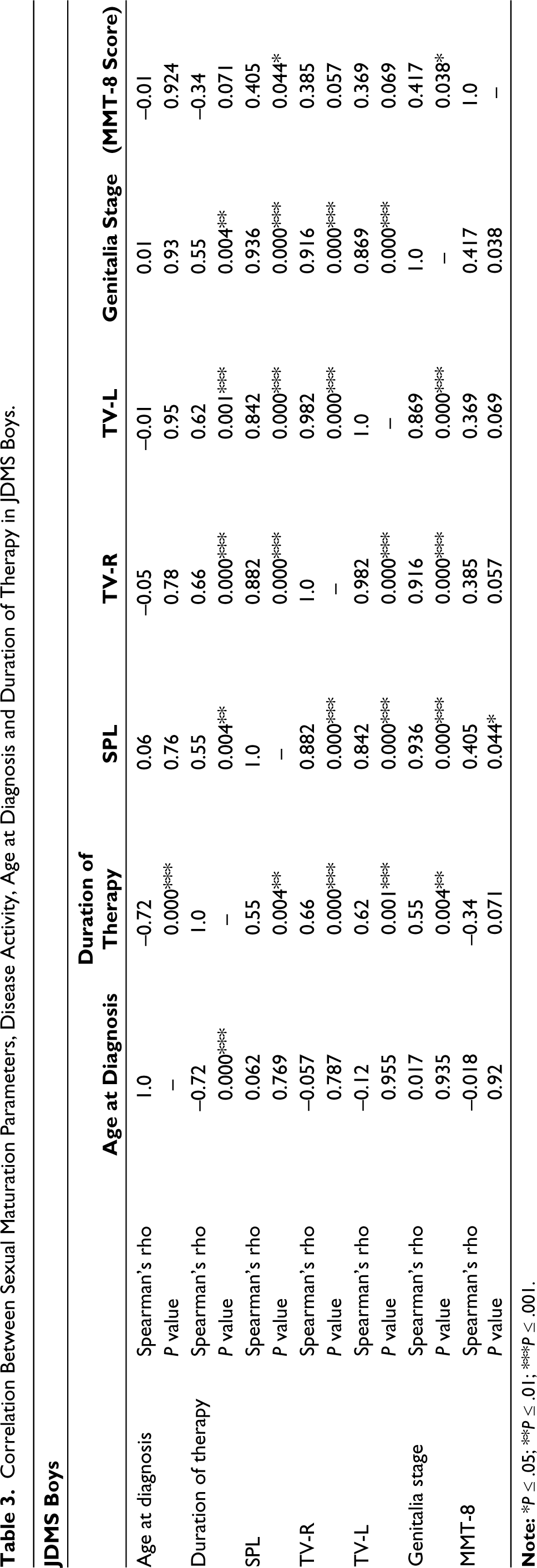
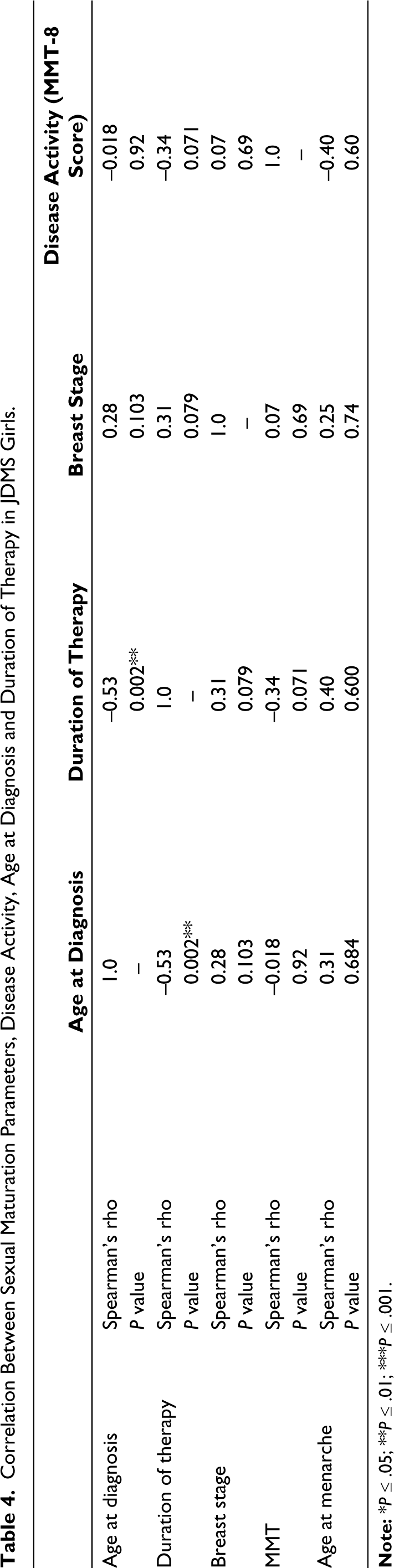
Non-parametric Spearman’s correlation coefficient was applied to study the strength and direction of association between variables of sexual maturation with age at diagnosis, duration of therapy, and disease activity (MMT-8 score) in boys and girls with JDMS (Tables 3 and 4). A significant correlation between different sexual maturation parameters (i.e., genitalia stage, testicular volume, stretched penile length) and duration of therapy was noticed among boys with JDMS. In contrast, no significant correlation could be noticed among JDMS girls.
Correlation Between Sexual Maturation Parameters, Disease Activity, Age at Diagnosis and Duration of Therapy in JDMS Boys.
Correlation Between Sexual Maturation Parameters, Disease Activity, Age at Diagnosis and Duration of Therapy in JDMS Girls.
Discussion
Through this study, we have tried to delineate the pubertal profile of children with JDMS. Ours is the largest cohort from Asia and no other study has been able to depict the true picture of sexual patterns in patients afflicted with JDMS, till date. Majority of our girls with JDMS (34.28%) had just entered puberty, that is, stage B2 of breast development, and 22.86% of JDMS girls had attained menarche. Our study girls were comparable in attaining breast stage 2 (10.9 years) with those recorded among normal affluent Indian girls (10.9 years), 7 whereas it was delayed by about half a year as compared to their normal Chandigarh (10.33) 8 counterparts. Our JDMS girls (3.7 years) developed their breasts to full maturity (stage B II to V) earlier than their normal Chandigarh (5.8 years), and affluent Indian (5.3 years) counterparts. Attainment of menarche in our study patients (13.75 years) was delayed in comparison to their normal affluent Indian (12.6 years) and Chandigarh (12.4 years) peers. Interestingly, the age at which our study females reached stage B2 and menarche was comparable to that of their other JDMS peers. 2 Age of attainment of genitalia stage G2 in our JDMS boys (12 years), was delayed by 6 months (11.5 years) as compared to well-off Chandigarh boys, 9 whereas it was advanced by 1.5 years when contrasted with affluent Indian counterparts (13.3 years). Interestingly, none of our study subjects depicted a delayed pubertal onset (i.e., B2 > 13 years of age in girls and G2 > 14 years in boys) in comparison to 18% of JDMS children with a delay in pubertal onset as reported by Nordal et al 2019. 2
Conclusion
The current study’s findings show that our JDMS children have comparable pubertal attainments; only female JDMS patients have a slightly delayed onset of menarche when compared to their normal counterparts, implying that disease activity has a lesser influence on the sexual maturation of JDMS patients from north-western India. Furthermore, it is probable that the availability of corticosteroid medication aided in the normal pubertal development of JDMS youngsters. Nutritional and socioeconomic factors may have had an additional impact. Nevertheless, this study was conducted during the COVID-19 pandemic and is based on a smaller sample size. Further longitudinal studies based on a larger sample need to be conducted to determine if this disease has an impact on puberty among JDMS patients. For these children with JDMS, we advise tracking SMR staging at every follow-up appointment to implement need-based medicinal, nutritional, and other interventions, promptly.
Footnotes
Authors Contribution
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Approval from Institutional Ethics Committee of PGIMER, Chandigarh was obtained prior to the conduct of this study (No.: INT/IEC/2020/SPL-1500, Dated: 1/12/2020).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent form either of the parents as well as assent from the patients was taken before enrollment in the study.