
Abstract

Dear Editor,
Peripheral neuropathies are the most common neurologic manifestations seen in rheumatoid arthritis (RA). 1 These include compressive neuropathies such as carpal tunnel syndrome (CTS) and non-compressive neuropathies such as mononeuritis multiplex, distal sensory neuropathy and autonomic neuropathy, wherein the distal sensory variant is more common.1,1,1 Mononeuritis multiplex is considered to be of vasculitic aetiology, while distal sensory neuropathy is non-vasculitic. 2 The prevalence of CTS in RA is around 10%, while that of mononeuritis multiplex is <1%. 1 Other factors contributing to neuropathy such as drugs, toxins, vitamin B12/folate deficiency or comorbid conditions like diabetes mellitus should be considered before attributing the neuropathy to RA.
Encephalopathy, on the other hand, in RA is extremely rare. The most common central nervous system (CNS) manifestation seen in RA is myelopathy secondary to Atlantoaxial dislocation, 1 followed by stroke. Other rare manifestations include aseptic meningitis, CNS vasculitis and rheumatoid nodules within the brain and meninges. Leukoencephalopathy in RA should raise suspicion of infectious (e.g., progressive multifocal leukoencephalopathy) or toxic aetiology. Toxic encephalopathy may be caused by various causes such as cranial irradiation, therapeutic agents, drugs of abuse or environmental toxins. 5 One of the toxins which can cause neuropathy and leukoencephalopathy in an acute or chronic fashion is arsenic. Common sources of arsenic toxicity are contaminated water or occupational exposure. 6 However, arsenic toxicity has been reported secondary to complementary and alternative medications (CAM) in many case series and reports.1,1 CAM use remains extremely popular among patients of RA. 9 A primary care survey in the United States has shown that the ‘ever use’ of CAM in RA is as high as 90%. The overall prevalence of CAM use in RA varies between 20% and 90% in most studies. 9 Here we report a case of RA presenting with neuropathy and encephalopathy, secondary to neurotoxicity, caused by inappropriate levels of arsenic present in CAM.
Case Report
A 25-year-old female patient of RA presented with painful distal sensory and motor neuropathy. Her illness started as bilateral symmetrical polyarthritis 1 ½ years ago, predominantly affecting small joints of hands. She was at 5 months of pregnancy during disease onset and hence had been treated elsewhere with paracetamol only. Her symptoms flared postpartum, at which point, she started taking complementary and alternative medications (CAM), prescribed by an Ayurveda practitioner, with partial relief of her symptoms. Two months before this presentation, she was transfused two units of blood for severe anaemia and generalised weakness. When she presented to us, she had been having progressive, distal, symmetrical weakness of both upper and lower extremities, associated with painful paraesthesia for the past 1 month. She was given pulse methylprednisolone elsewhere, in view of suspected vasculitis and referred to our centre. Clinical examination showed bilateral wrist and foot drop (Figure 1A), absent deep tendon reflexes and symmetrical, distal positive sensory signs. Her higher mental functions were normal without any cranial nerve involvement and there were no active joints. There was no history of vasculitic rash, ulcers, gangrene, sicca, cough or dyspnoea. The differentials considered were vasculitis, possibly anti-neutrophil cytoplasmic antibody (ANCA) related, polyarteritis nodosa (PAN), undifferentiated vasculitis or RA with concomitant acute inflammatory demyelinating polyneuropathy (AIDP). Her investigations revealed normal inflammatory markers with negative rheumatoid factor (RF), antinuclear antibody (ANA), anti-neutrophil cytoplasmic antibody (ANCA) and positive anti-cyclic citrullinated peptide (CCP) (248 IU/dl by ELISA). Hand radiographs were suggestive of erosive arthritis (Figure 1C). Nerve conduction study showed severe axonal and demyelinating sensorimotor polyneuropathy involving bilateral radial, ulnar, common peroneal and sural nerves. Her urine examination was normal. Timeline of her disease course is shown in Figure 2.
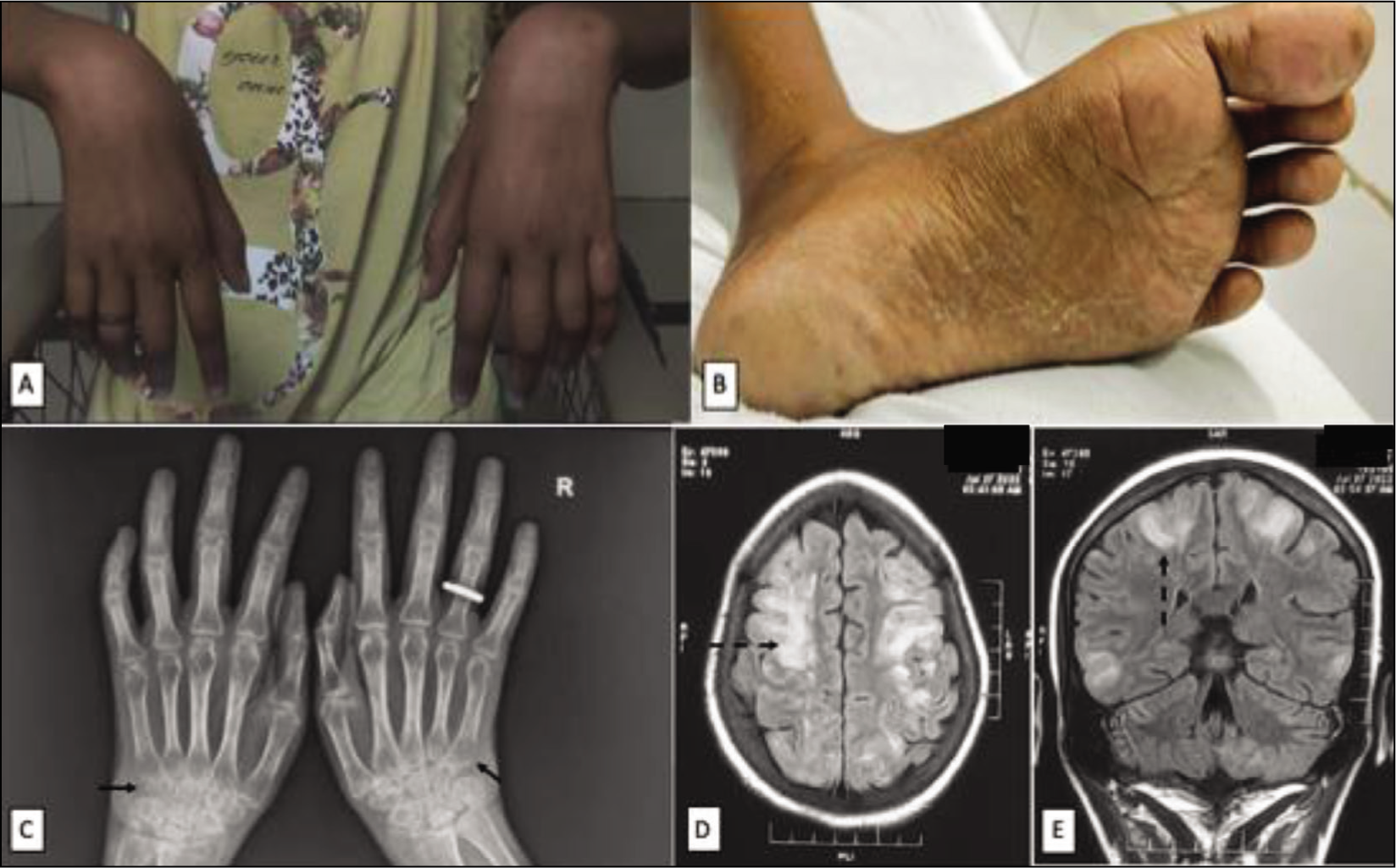
Timeline of Disease Course.
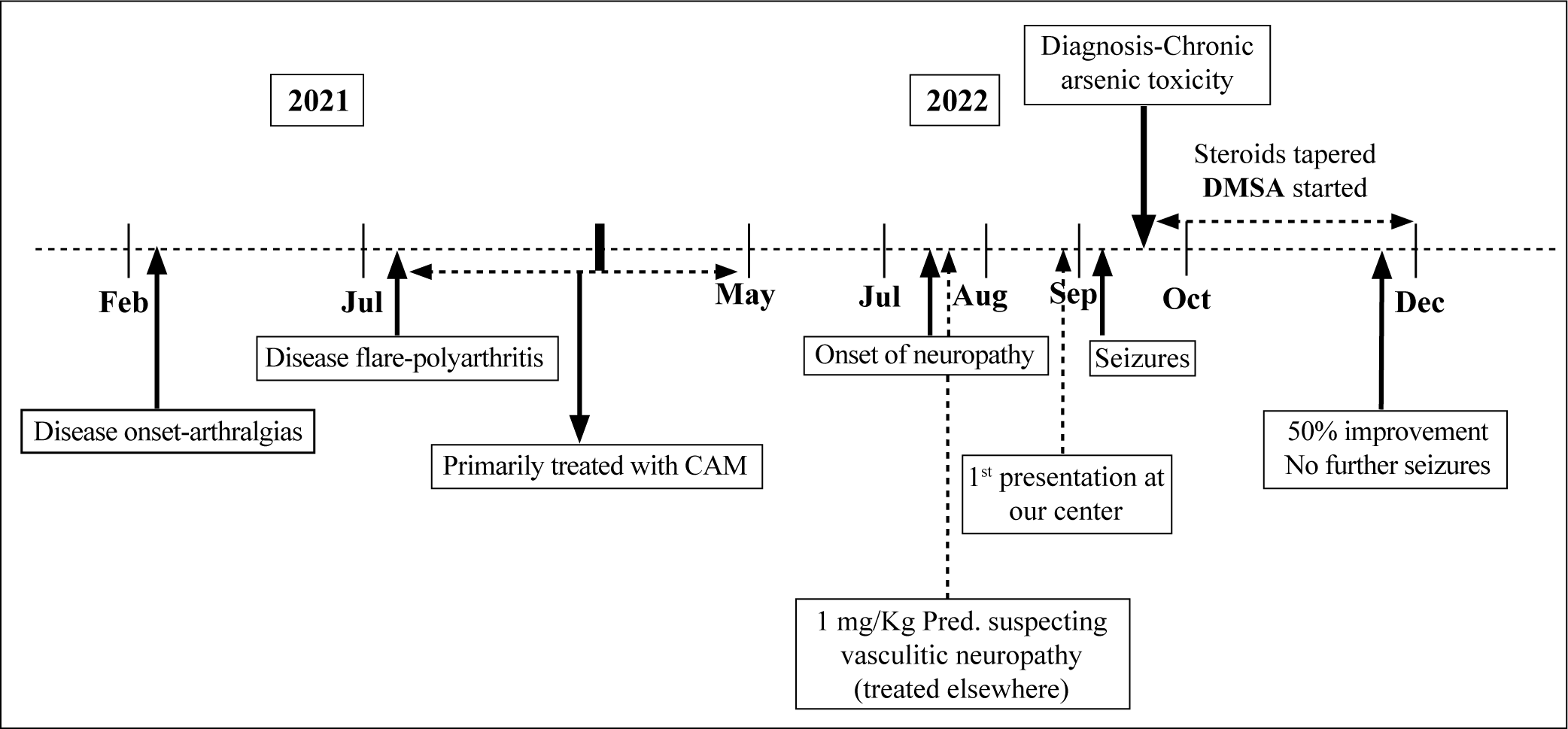
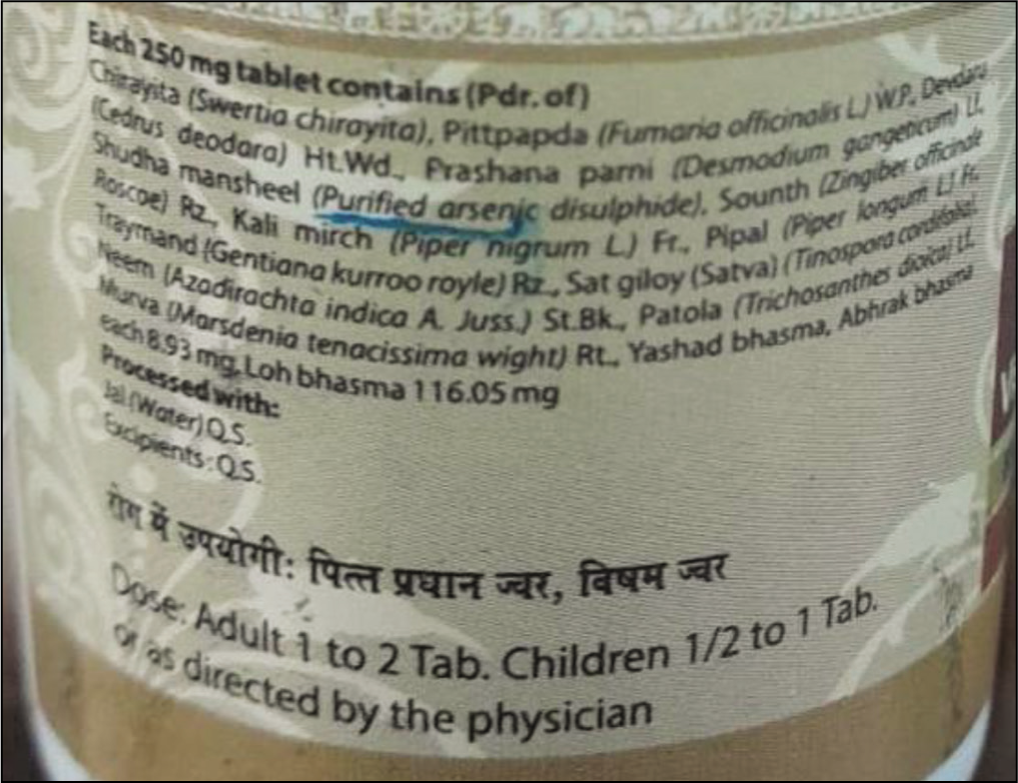
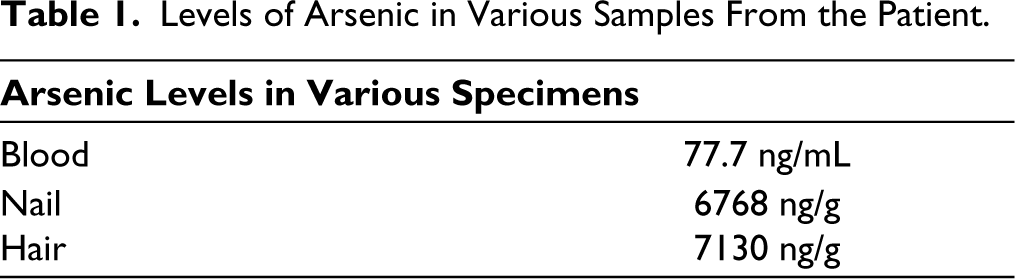
During the course of her hospital stay, she developed two episodes of generalised tonic-clonic seizures. Vitals signs, blood glucose and electrolytes were normal. Magnetic resonance imaging (MRI) of the brain revealed T2-hyperintense lesions in subcortical white matter, predominantly in the temporoparietal (Figure 1D and 1E) and cerebellar regions. 5 Electroencephalogram was normal. Cerebrospinal fluid (CSF) examination was unremarkable with normal protein (18.6 mg/dL), normal glucose and less than 5 leucocytes per high-power field (hpf). In view of the above atypical presentation of neuropathy, encephalopathy, we revisited our diagnosis. We did a thorough check of the patient’s Ayurveda medication, ‘Visham Jwarantak Lauh’ and found arsenic (purified arsenic disulphide, As2S3) and mercury in its contents (Figure 3). Examination of her feet revealed brownish hyperpigmentation with scaling and mild hyperkeratosis on the plantar aspect (Figure 1B) which further raised suspicion of chronic arsenic toxicity. Toxicological screen suggested high levels of blood arsenic (77.7 ng/mL; normal <1 ng/mL); 24-hour urine arsenic level was normal. She was diagnosed with chronic arsenic poisoning on a background of RA. The levels of arsenic in the hair and nails of the patient are mentioned in Table 1. She had taken 2 tablets a day for around 10 months and stopped using them 2 months ago. Urine arsenic levels are suggestive of recent exposure and it is likely why her urine arsenic levels were not high. 10 Her steroid dosage was tapered to 5 mg daily and thiamine and methylcobalamin replenishment was done. Although there are conflicting reports of its efficacy in chronic toxicity, chelation with dimercaptosuccinic acid (DMSA) was given, at a dose of 10 mg/kg per dose thrice daily for 5 days, followed by 10 mg/kg per dose twice daily for 2 weeks.1,1 At 3 months of follow-up, she has shown 50% improvement in motor and sensory symptoms. For the arthritis, she has achieved remission with low-dose steroids (≤5 mg prednisolone daily) and methotrexate 25 mg weekly. There have been no further episodes of seizures, while anti-epileptics have been tapered off.
Box of Complementary and Alternative Medicine (CAM) with Contents Showing Arsenic Disulfide.
Levels of Arsenic in Various Samples From the Patient.
Discussion
Complementary and alternative medicine use (CAM) is believed to be practiced in India for thousands of years and is commonly used by patients and physicians for a variety of indications. 12 CAM used in India is broadly described under the umbrella term, ‘AYUSH’, which stands for Ayurveda, Yoga and naturopathy, Unani, Siddha and Homeopathy. The use of AYUSH in India is actively promoted by the union ministry of AYUSH 13 and various traditional drugs have been tried for the management of RA. 14 Ayurveda involves the use of drugs of plant, animal or mineral origin. Ayurvedic preparations have been frequently found to have significant levels of arsenic, lead and mercury, which can potentially cause heavy metal toxicity and this practice, if not properly regulated, could lead to a significant public health problem. 15 On the other hand, heavy metals like gold were used earlier for the treatment of RA because of an immune-modulating role and, similarly, arsenic could have some immunomodulatory properties as well, as shown in this study on collagen-induced arthritis (CIA) mice model. 16
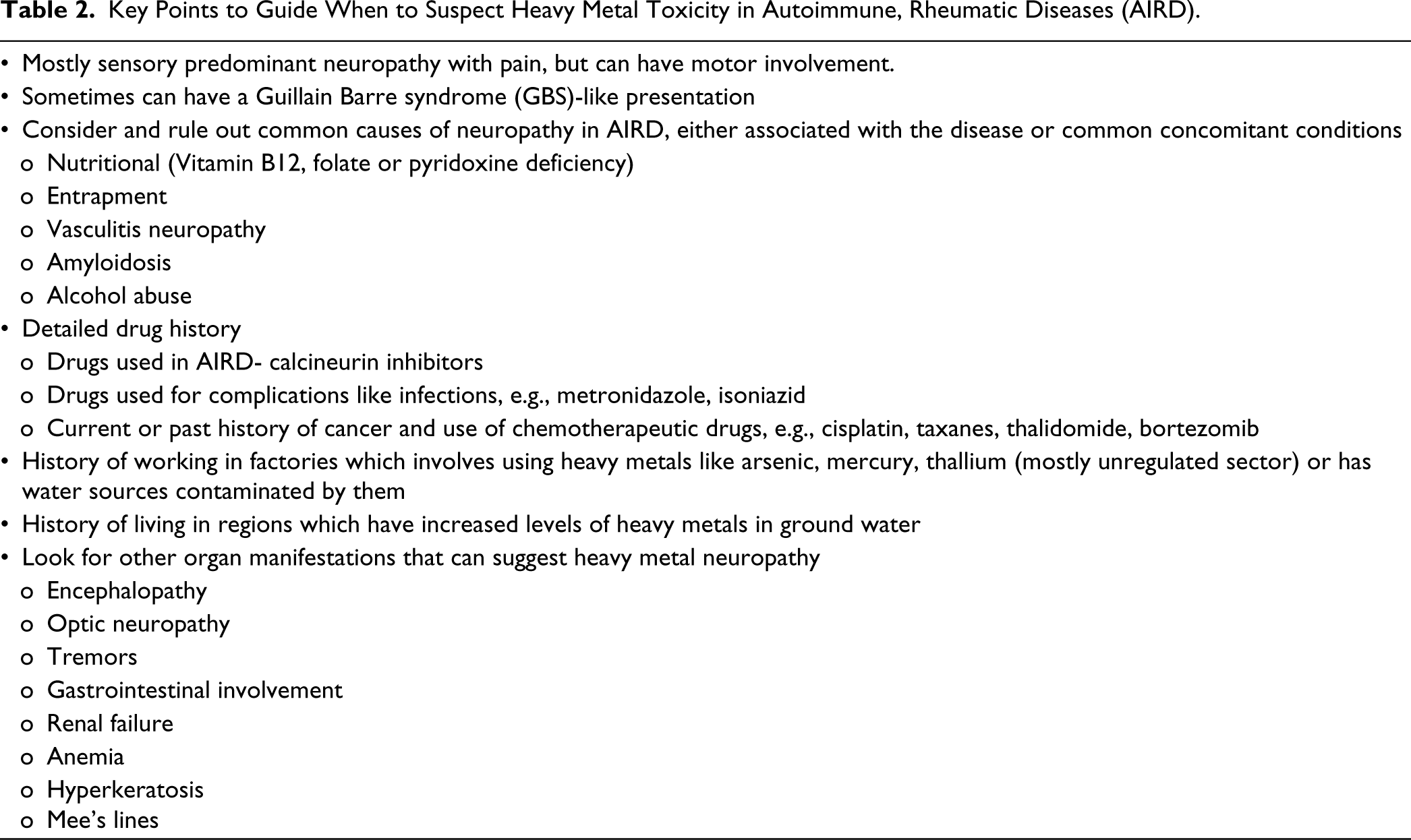
Arsenic exerts its toxic effects by inhibiting enzymes involved in DNA repair, replication and oxidative metabolism, thus generating reactive oxygen species (ROS) and causing DNA damage. Trivalent arsenic, which was present in the preparation described, is 60 times more toxic than pentavalent arsenic. 17 Arsenic toxicity can present in an acute or chronic fashion. Source of toxic arsenic is usually from contaminated water, seafood or industrial exposure. Acute toxicity generally results from accidental ingestion and presents with gastrointestinal (GIT) effects such as vomiting, colicky abdominal pain and watery diarrhoea. Chronic poisoning, on the other hand, presents in an insidious fashion, with involvement of skin, GIT, nervous system and increased incidence of cancer. 10 The typical skin finding is hyperpigmentation and keratosis of palms and soles (Figure 1B). Skin might also show the characteristic ‘rain-drop’ pigmentation and nails might have transverse white lines called Mee’s lines. 10 The most frequent neurological finding is a peripheral neuropathy mimicking Guillain-Barre syndrome (GBS). 18 This patient also had a GBS-like presentation, with glove and stocking anaesthesia. It can also cause encephalopathy, which predominantly affects the white matter and can present with seizures, confusion and dementia. 5 Key points to guide when to suspect heavy metal toxicity in autoimmune, rheumatic diseases (AIRD) are given in Table 2.
Key Points to Guide When to Suspect Heavy Metal Toxicity in Autoimmune, Rheumatic Diseases (AIRD).
Many case reports and series of arsenic toxicity from ayurvedic drugs continue to be reported, particularly from India.1,1 Manifestations of chronic arsenic poisoning can sometimes mimic features of rheumatic diseases and pose diagnostic dilemmas. In a case report by Wakhlu et al., 19 the skin rash seen in a patient of chronic arsenic toxicity mimicked the Gottron’s rash, typically seen in dermatomyositis. To the best of our knowledge, this is the first case report of chronic arsenic toxicity in a patient of RA. This case posed a diagnostic challenge because of its similarity with vasculitic neuropathy and AIDP, both of which can be associated with inflammatory arthritis in various rheumatic diseases. 20
Conclusion
Chronic arsenic neurotoxicity should be considered in the differentials, if patients of RA present with neuropathy, with or without encephalopathy, particularly if they have used complementary and alternative medicine. A thorough skin examination, particularly of palms and soles, and nails could provide valuable clues in the diagnosis.
Supplementary Material
The supplementary material for this article is available online.
Footnotes
Acknowledgements
We thank the CSIR-Indian Institute of Toxicology Research, Lucknow for their help in analysing blood and urine samples for heavy metals.
Author Contributions
SPB, SM, AKV, and STG cared for the patient, collected data and wrote the manuscript. SPB, SM and STG edited the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent has been taken from the patient and her primary caregiver.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.