
Abstract
Introduction:
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease with various clinical manifestations and approximately 50% of the SLE patients develop lupus nephritis (LN), which increases the risk of renal failure, cardiovascular diseases and overall survival.
Objectives:
Evaluation of neutrophil-derived parameters (Neut-X, Neut-Y and Neut-Z) as an inflammatory, disease activity marker and as a predictor of nephritis in SLE patients.
Material and Methods:
In this cross-sectional study, 3 ml K3EDTA blood was taken from 110 SLE patients presented in Department of Clinical Immunology to evaluate neutrophil-derived parameters in Sysmex XT2000i haematology analyser and their correlation with other inflammatory biomarkers like, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) as well as SLE disease activity index-2000 (SLEDAI-2K). 24-hours urine protein levels were also estimated as a marker of renal involvement. Records of renal biopsy were available in 73 SLE patients, who belonged to different morphologic classification of LN.
Results:
After performing bivariate Spearman correlation analysis (SPSS software, version 26.0), Neut-X (measures cytoplasmic granularity by side scattering) and Neut-Z (vector sum of Neut-X and Neut-Y) showed a significant positive correlation (r > 0.200, P < .05) with ESR, CRP and SLEDAI-2K while Neut-Y (measures nucleic acid content by sideward fluorescence) showed a significant negative correlation (r > 0.200, P < .05) with ESR and CRP. Receiver-operating characteristic curve analysis was used to evaluate diagnostic value of 24-hour urine protein and predictive values of neutrophil-derived parameters for renal involvement in SLE patients. Among neutrophil-derived parameters, Neut-X was found to be the best predictor of renal dysfunction with highest AUC of 0.710 (95% CI: 0.604-0.816; cut-off: 1344.50; sensitivity: 84.7%; specificity: 50%) followed by Neut-Z with AUC of 0.707 (95% CI: 0.600-0.813; cut-off: 1403.67; sensitivity: 87.5%; specificity: 50%).
Conclusion:
Our study shows that neutrophil-derived parameters may be used as novel cost-effective, non-invasive biomarker of disease activity as well as for predicting renal involvement in SLE patients.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disorder of unknown aetiology with incidence of 20–70 per 100,000 per year. 1 SLE is chronic disorder and characterised by remission and relapses of clinical symptoms and may present with various non-specific and organ-specific manifestations. The disease activity in SLE is usually assessed by SLEDAI-2K (Systemic Lupus Erythematosus Disease Activity Index-2000), which is a complex tool composed of 24 clinical and laboratory variables. 2 The complexity is indicated by diverse clinical features and laboratory abnormalities. Among various clinical manifestations of SLE, lupus nephritis (LN) is one of the most common with an incidence of 40%–60%. 3 LN is an immune complex mediated glomerulonephritis which develops either due to production of autoantibodies, complement activation or immune complex deposition which increases the risk of renal failure, cardiovascular diseases and overall survival. Low serum C1q, C3 and C4 have been associated with increased SLE disease activity, which is manifested by active nephritis and extrarenal involvement. 4 Renal biopsy is an invasive gold standard method for determining class of LN 5 because knowledge of the LN class is a relevant component of adequate treatment planning in SLE patients. 3 For this reason, there is a constant need for an non-invasive, sensitive as well as cost effective method for detecting or predicting renal involvement in SLE patients. The Renal Pathology Society/International Society of Nephrology (or RPS/ISN) classification include 6 classes: minimal mesangial lupus nephritis, mesangial proliferative lupus nephritis, focal lupus nephritis, diffuse lupus nephritis, membranous nephropathy and advanced sclerosing lupus nephritis. 6 Ultimately, early assessment of renal involvement leads to preservation of renal function as well as mortality and morbidity of SLE patients; this results in decrease in overall disease burden. The Sysmex XT200i automated haematology analyser has been used for this study. The Sysmex analysers used in our study measured the inner granularity by sideward scatter light and displayed as Neut-X whereas the nucleic acid content is measured by sideward fluorescence light and displayed as Neut-Y while Neut-Z is the vector sum of these two. Various studies on cell population data (CPD) like neutrophil-derived parameters (Neut-X, -Y and -Z) have been part of the relevant literature for the past two decades. There are few studies of Neut-X, -Y and -Z on sepsis, 7 myelodysplastic syndromes 8 and febrile patients of SLE. 9 There is paucity of studies on Neut-X, -Y and -Z in SLE patients with renal involvement.
This study was intended to explore the clinical relevance of neutrophil-derived parameters (Neut-X, Neut-Y and Neut-Z) as an inflammatory, disease activity marker and as a predictor of nephritis in SLE patients.
Material and Methods
Patients Selection
One hundred ten patients were included in this cross-sectional study with a diagnosis of SLE as per ACR (American College of Rheumatology Criteria) criteria from Department of Clinical Immunology and Rheumatology, Sanjay Gandhi Postgraduate Institute of Medical Sciences (SGPGIMS) Lucknow from January 2020 to July 2022 and disease activity were calculated by SLE disease activity index-2000 (SLEDAI-2K),
Patients with other autoimmune diseases, haematological diseases and who received recent blood transfusion were excluded from this study.
Patients’ demographic data including name, age, gender and medical history were recorded within 24 hours of admission.
This study was approved by the Institutional Ethics Committee (IEC Code: 2020-338-MD-EXP-34), SGPGIMS. Forty healthy adult age-matched donors were also included as controls
Laboratory Analysis
Haematological Analysis
A total of 3 ml K3EDTA blood sample was taken from all enrolled patients, for routine hemogram on fully automated Sysmex-XT 2000i haematology (Sysmex Co., Kobe, Japan) analyser. A plain blood sample (spray-coated silica) was also taken for biochemical and immunological investigations. Values of neutrophil-derived parameters (Neut-X and Neut-Y) and erythrocyte sedimentation rate (ESR) were evaluated directly. Vector sum of Neut-X and Neut-Y was used to calculate value of Neut-Z.
Urine Analysis
Mid-stream urine sample was collected as per standard protocol, for study of urinary casts (granular/ RBC cast), haematuria (>5 RBCs/hpf), proteinuria (>0.5 gm/24 hours), pyuria (>5WBCs/hpf) for chemical and microscopic examination.
Immunological Analysis
Samples for C-reactive protein (CRP), C3 and C4 as per standard case protocol, were sent on day of inclusion from immunology ward and OPD.
Data Extraction
In this study, all SLE patients were divided into two groups based on renal involvement (73 were SLE with LN and 37 were SLE without LN).
Statistical Analysis
Analysis was performed using SPSS software (version 26.0, IBM, Chicago, IL, USA). The normality of distribution was checked by Kolmogorov-Smirnov test. Quantitative variables were expressed as median and interquartile range (IQR) and tested by nonparametric test (Mann–Whitney independent sample U test and Kruskal–Wallis test). Statistical significance was defined as p < .05. The Spearman rank correlation coefficient was calculated to examine the association between two continuous variables. Receiver-operating characteristic (ROC) curve analysis was then performed to determine the sensitivity and specificity of possible parameters (Neut-X, Neut-Y and Neut-Z) for discriminating renal involvement in SLE patients from without renal involvement.
Results
The Demographic Characteristics and Laboratory Variables
The median age of 110 SLE patients was 31 years (range: 18–64 years) with predominance of females (94.54%). A total of 70% SLE patients belonged to the age group of 21–40 years.
The duration of illness and distribution of SLE disease activity index (SLEDAI) in SLE patients are shown in Table 1.
Demographic and Disease Variables of SLE Patients.
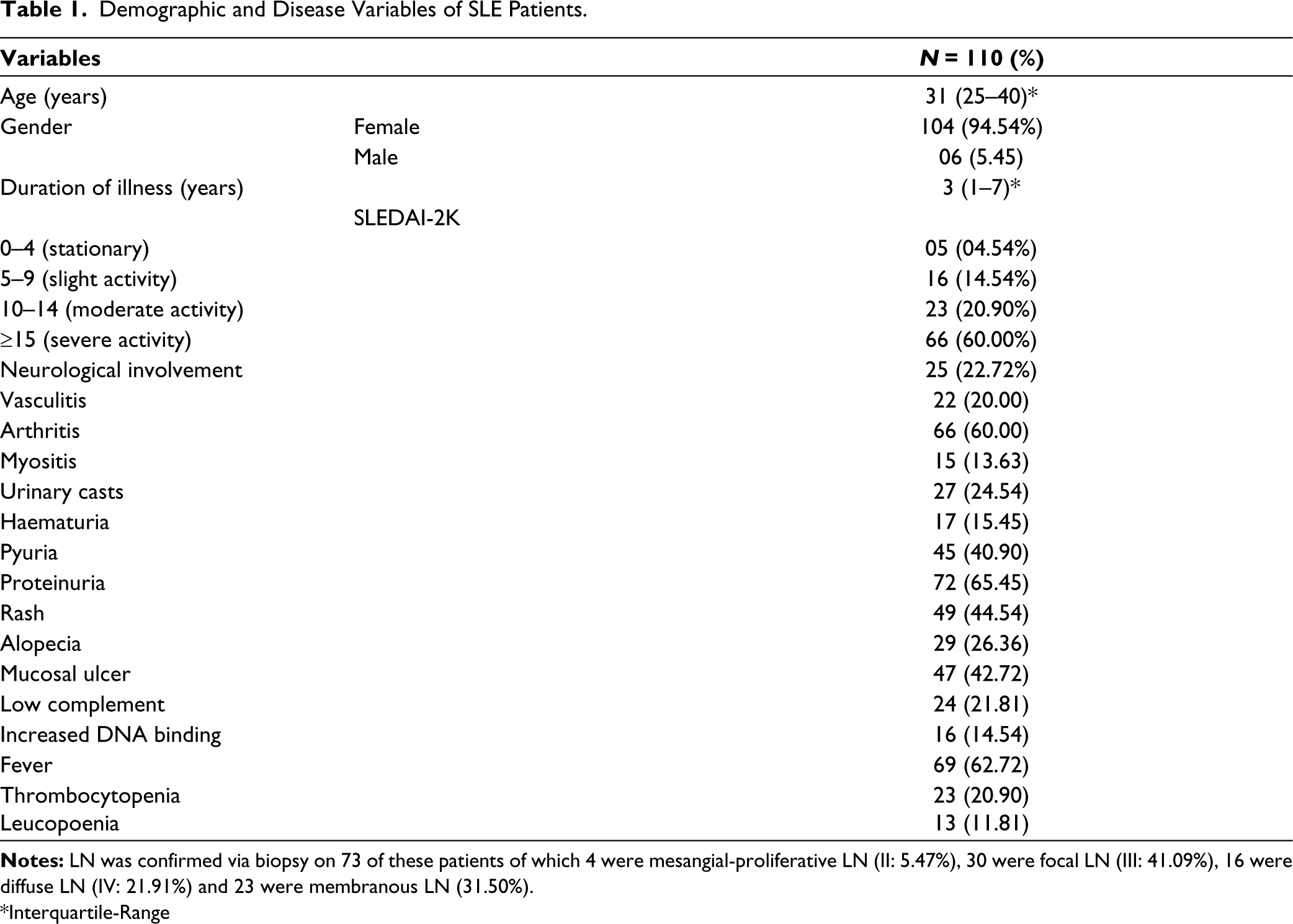
*Interquartile-Range
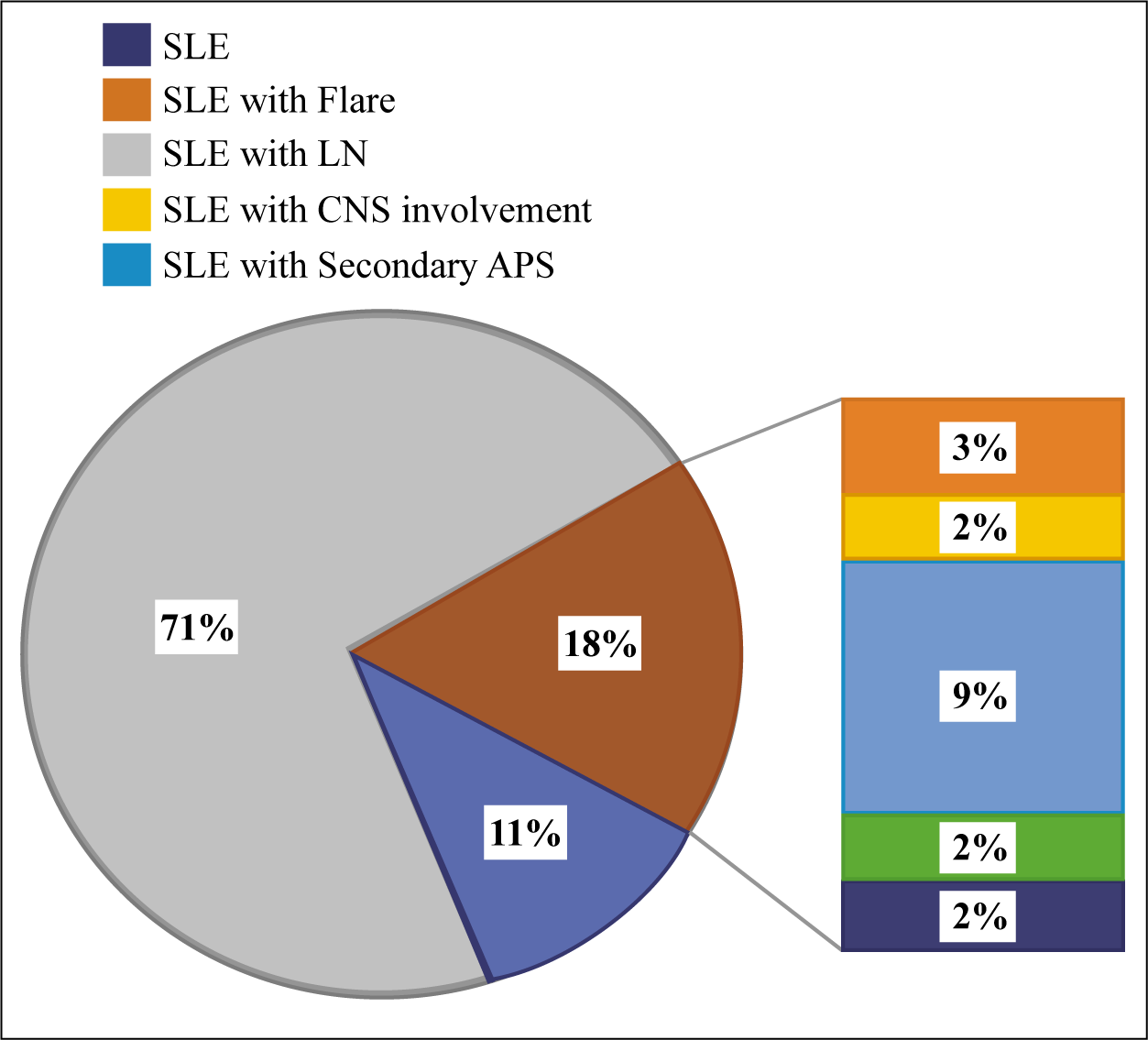
Among the remaining 37 SLE patients, 11 patients were presented with SLE only, 9 presented with a primary diagnosis of SLE with secondary antiphospholipid syndrome and 7 had vasculitis (Figure 1).
Distribution of Primary Clinical Diagnosis.
Laboratory Parameters
Medians of ANC, Neut-X, Neut-Y and Neut-Z showed statistically significant (P < .05) difference among SLE patients with LN as compared to those without LN and healthy controls (Table 2).
Laboratory Parameters in SLE Patients With, Without LN and Healthy Controls.
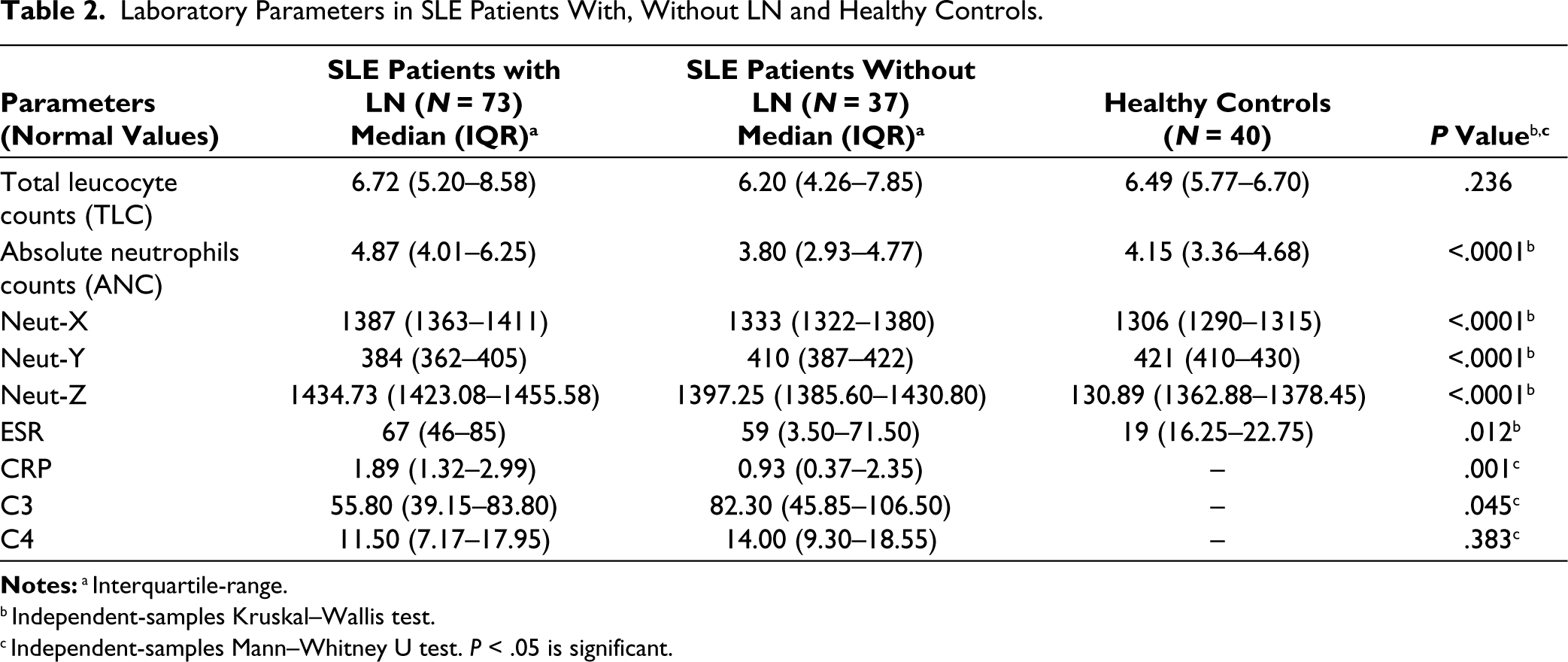
Notes:a Interquartile-range.
b Independent-samples Kruskal–Wallis test.
c Independent-samples Mann–Whitney U test. P < .05 is significant.
There was a statistically significant (P < .05) difference in neutrophil-derived parameters between SLE patients with and without LN. Medians of Neut-X and Neut-Z were high, while Neut-Y were low.
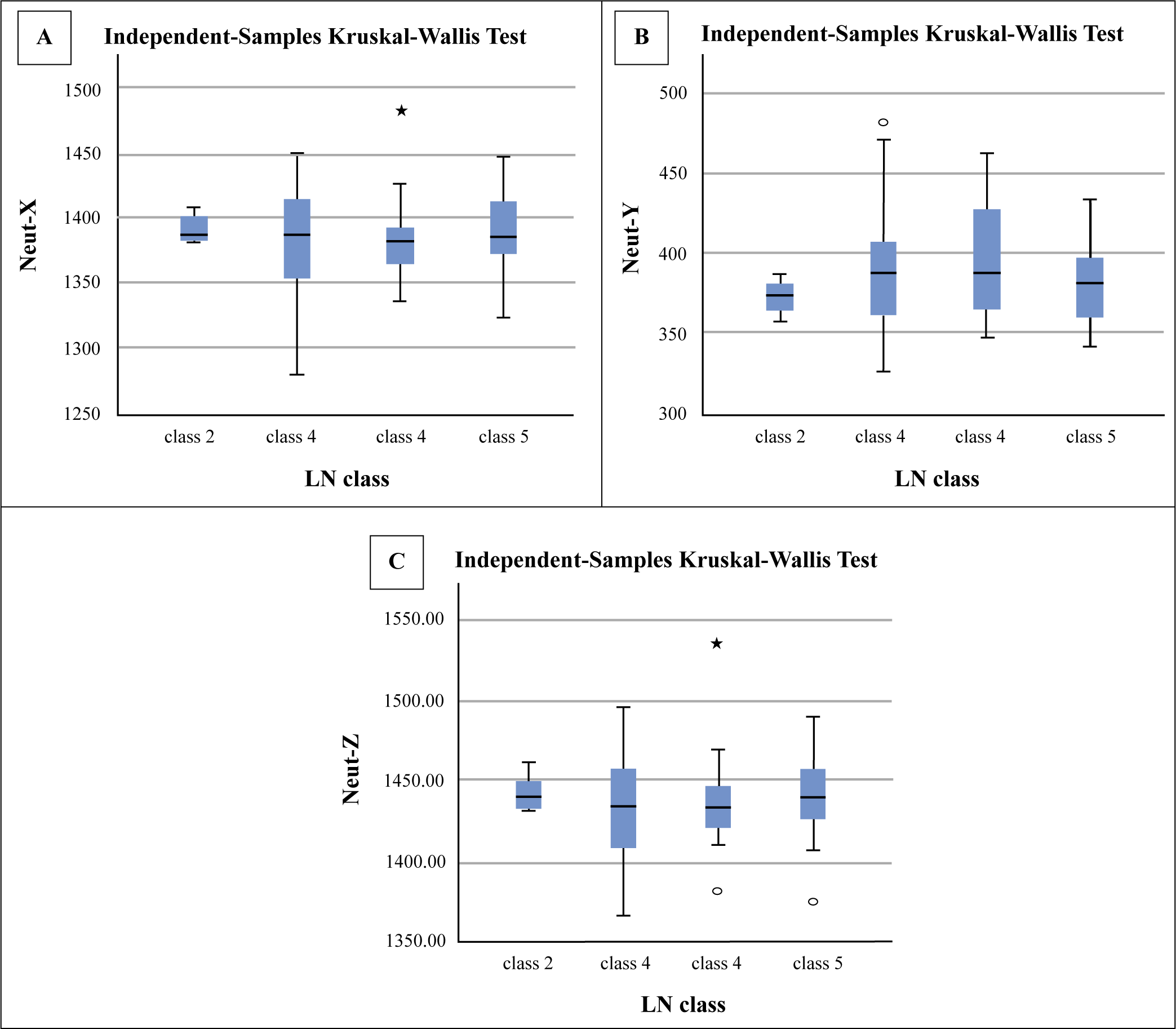
However, neutrophil-derived parameters showed no statistically significant difference among different classes of LN (Figures 2(A)–(C)).
Comparison of Neutrophil-Derived Parameters in SLE Patients Among Classes of Lupus Nephritis (A) Neut-X, (B) Neut-Y and (C) Neut-Z.
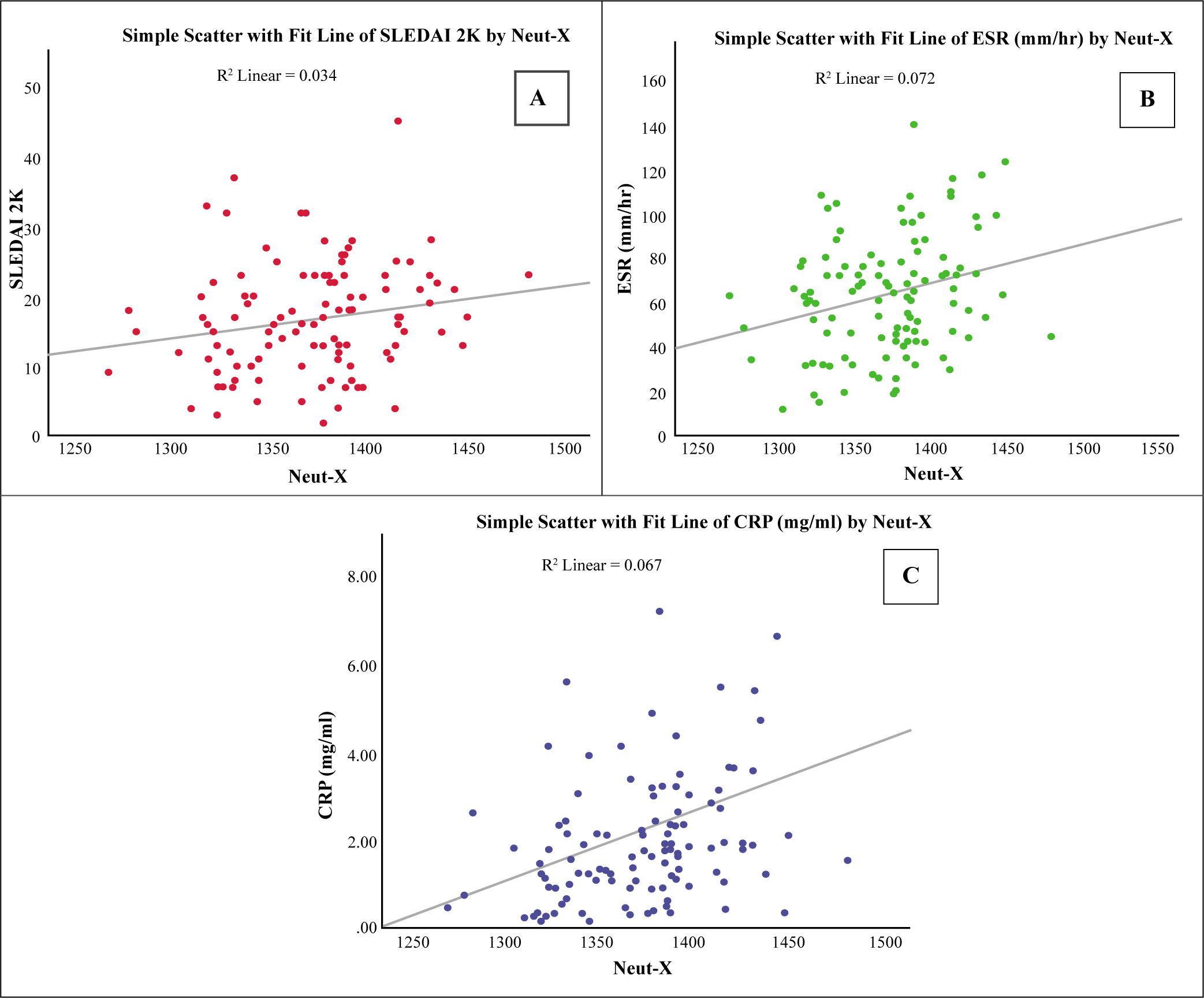
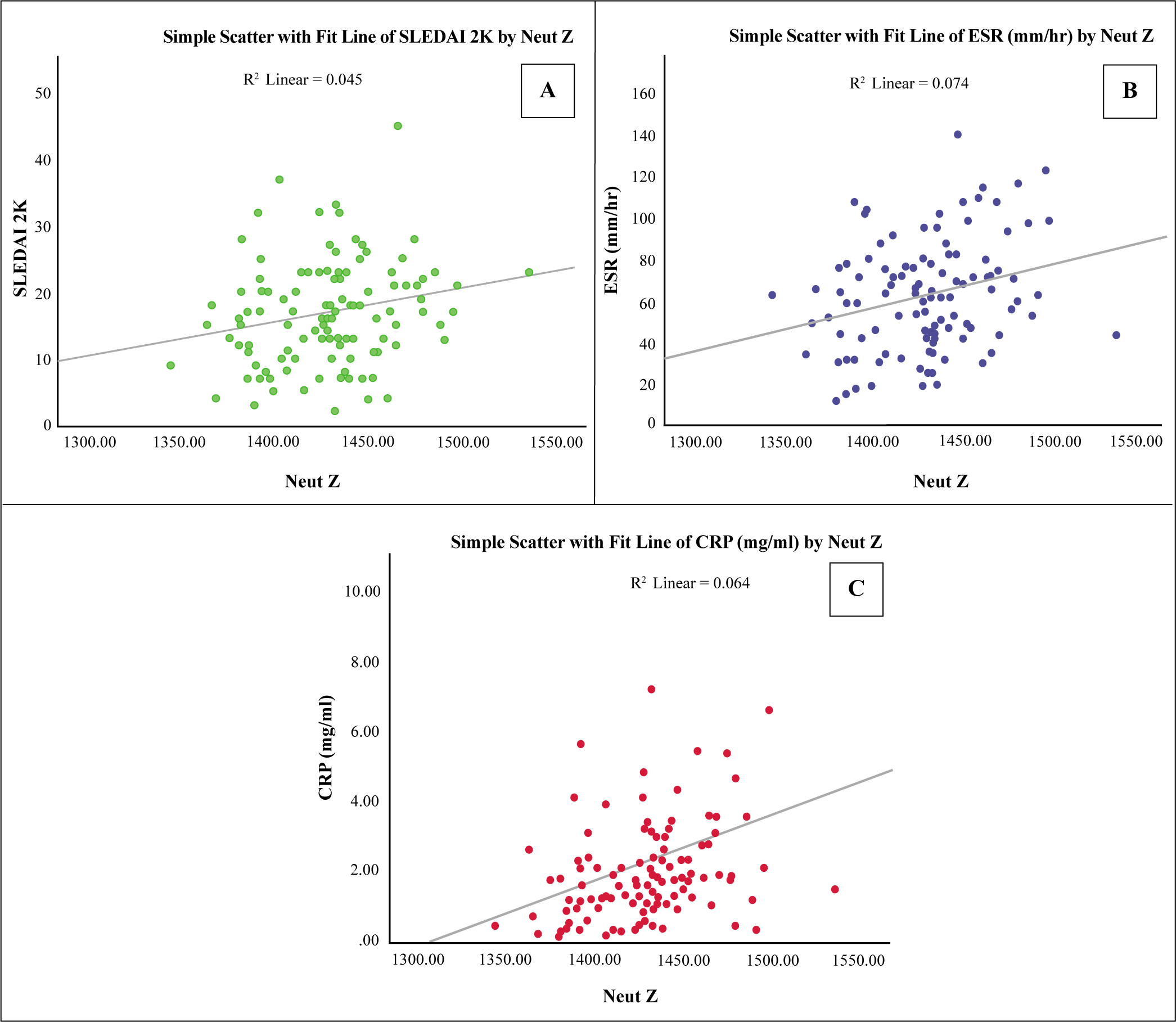
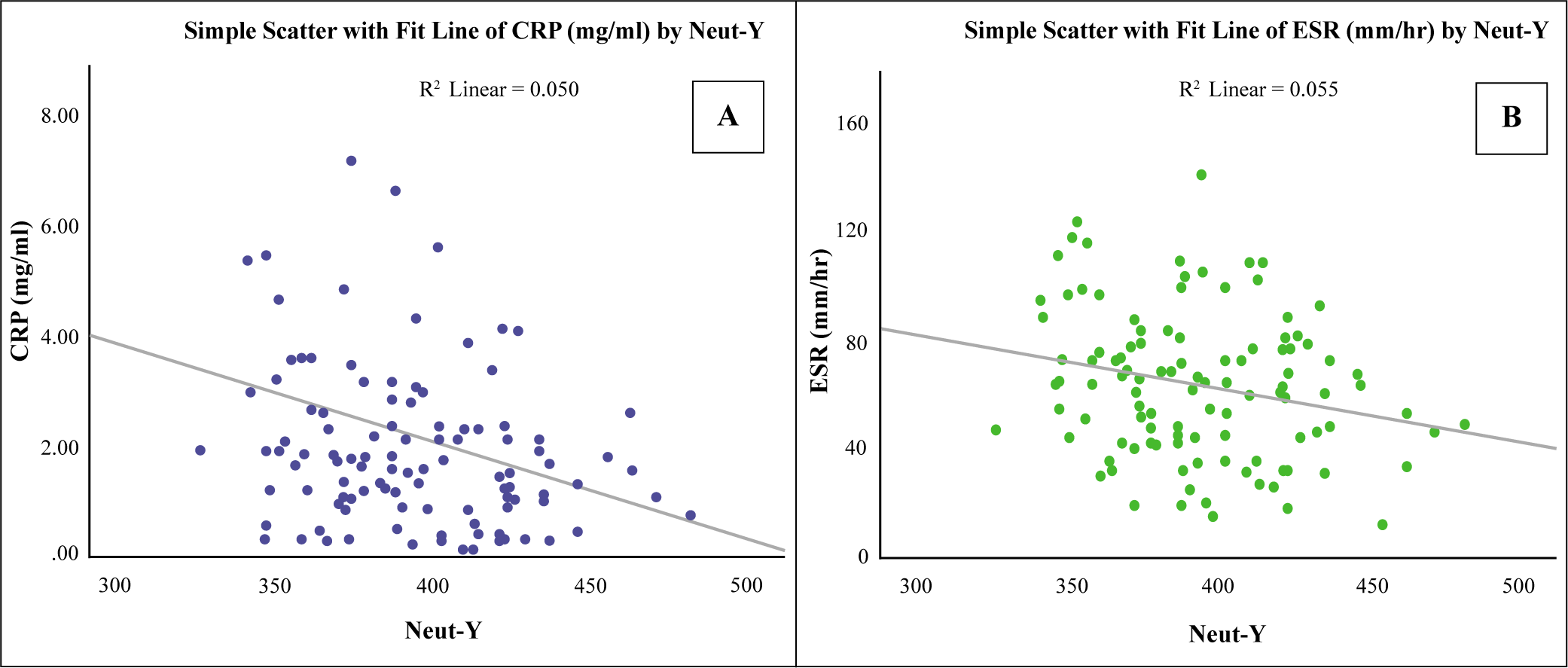
After performing bivariate Spearman correlation analysis, Neut-X and Neut-Z showed a significant positive correlation, while Neut-Y showed a significant negative correlation with disease activity and inflammatory biomarkers like ESR and CRP (Figures 3 (i)–(iii)).
Neut-X Level Was Positively Correlated with (A) SLEDAI-2K, (B) ESR and (C) CRP.
Neut-Z Level Was Positively Correlated with (A) SLEDAI-2K, (B) ESR and (C) CRP.
Neut-Y Level Was Negatively Correlated with (A) ESR and (B) CRP.
Furthermore, LN patients showed a statistically significant positive correlation with ESR and CRP, while patients without LN did not exhibit any significant correlation.
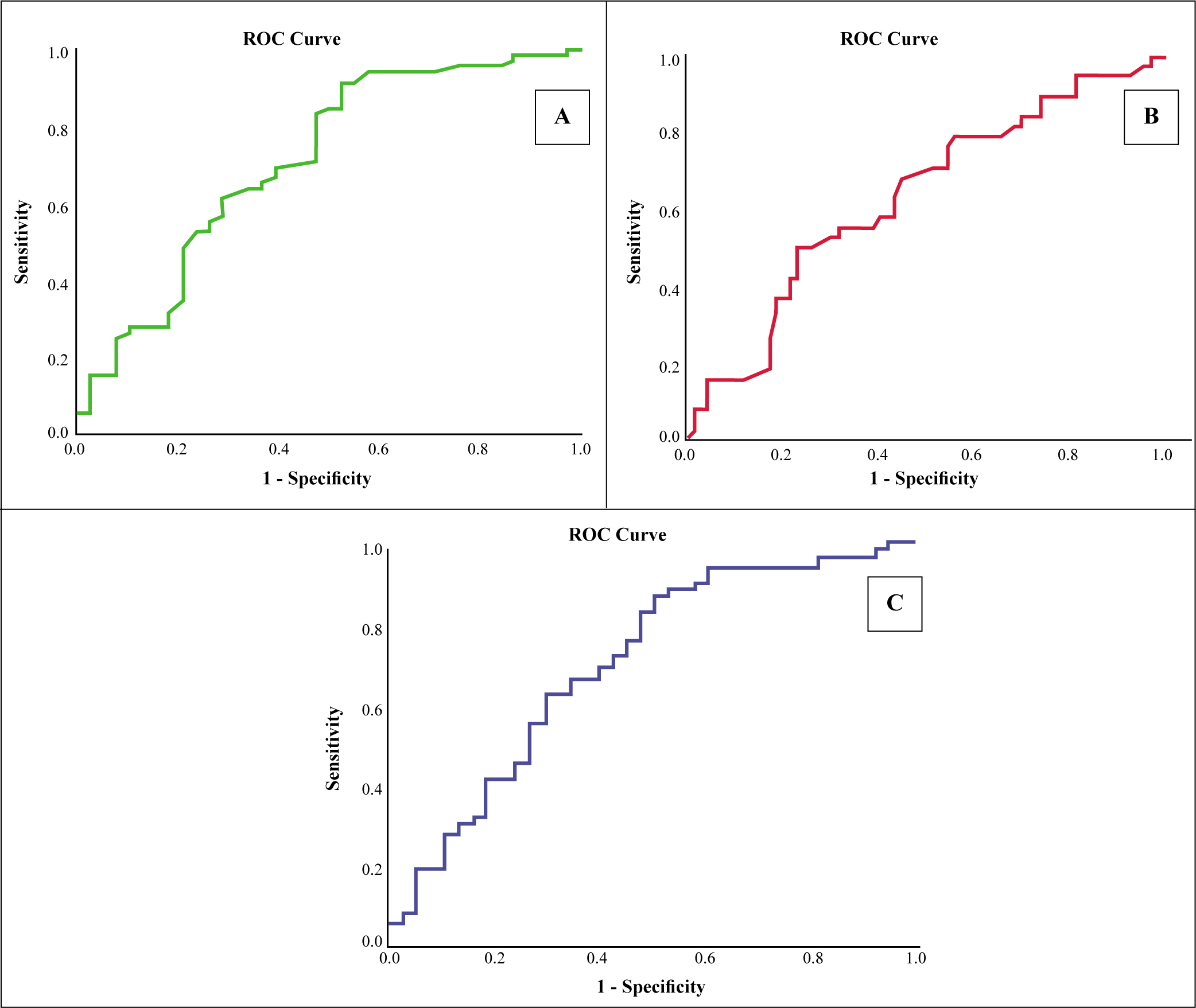
Based on the ROC analysis, the Neut-X value (using a cut-off of 1344.50) differentiated SLE patients with LN from without renal involvement, with a sensitivity and specificity of 84% and 50%, respectively. Moreover, the Neut-Z (using a cut-off of 1403.67) differentiated LN from without LN with a sensitivity and specificity of 87% and 50%, respectively. These results indicated that Neut-X (AUC: 0.710) and Neut-Z (AUC: 0.707) were sensitive and specific markers for discriminating renal involvement in SLE patients (Figures 4(A)-(C)).
ROC Curve Comparing. (A) Neut-X, (B) Neut-Y and (C) Neut-Z for Predicting Lupus Nephritis in SLE Patients.
Discussion
SLE is a worldwide chronic autoimmune disease which may affect every organ and tissue. 2 Complex pathogenesis of SLE involves multiple cellular components of the innate and immune systems: presence of autoantibodies and immunocomplexes, engagement of the complement system, dysregulation of several cytokines including type I interferons and disruption of the clearance of nucleic acids after cell death. 10 Early detection and treatment is necessary in LN patients because delayed diagnosis significantly increases the risk of morbidity, end-stage renal disease and death in SLE patients. 11
The age range, predominance of female patients and duration of disease illness in our study was similar to studies by of Qin et al., 12 Yang et al., 13 Ayna et al., 14 Wu et al., 15 Yu et al., 16 Suszek et al., 17 Safak et al., 18 Li W et al. 19 and Soliman et al. 20
Median duration of illness in SLE patients was 3 years with IQR of 1–7 years in current study and similar duration was also expressed in studies by Yolbas et al. 21 and Soliman et al. 20 with mean of 2.6 years and 3.1 years, respectively.
In the present study, arthritis and fever were the most common clinical manifestations of SLE similar to previous studies by Rana et al. 22 and Pattanaik et al. 23 Oral ulcer was also a very common manifestation in 41% SLE patients of this study as opposed to study by Saigal et al. 24 The incidence of alopecia (26%) was lower in present study as compared to study by Saigal et al. 24 More than half, that is, 73 (66%) SLE patients in present study had a primary diagnosis (biopsy proven) of LN which was similar to studies by Qin et al. 12 , Ayna et al., 14 Wu et al., 15 Soliman et al. 20 and Suszek 17 et al. The patients with severe disease activity, that is, with active urinary sediments at the time of scoring, were more in present study as compared to studies by Yu et al. 16 and Sheriff et al. 25
ESR (mean: 63 mm/hr) values of SLE patients were high in present study at the time of inclusion, as compared to previous studies by Qin et al. 12 and Yang et al. 13 As present study was conducted at tertiary care centre, more than half SLE patients had severe inflammation in form of high disease activity attributed due to renal involvement in different class of LN, with flares and fever.
CRP is the most widely used inflammation marker due to its kinetics and it usually gets elevated in various inflammatory conditions. Though our study also showed low CRP (mean: 2.21 g/l) levels in SLE patients, as compared to previous studies by Yu et al., 26 Yu et al. 16 and others.13,19,22,27–29 The probable reason behind low CRP values is that our cohort patients were at various stages of disease progression ranging from SLE without complications to end stage renal disease.
Complement levels, that is, C3 (mean: 73.03 mg/dl) and C4 (mean: 14.50 mg/dl) were in the normal range in this study and results are found to be similar to studies by Qin et al. 12 and Yu et al. 26 while study by Xie et al. 30 reported low values of complements. SLE patients of this study were on immunosuppressive treatment which ranges from few weeks to several years and this lead to a sustained reduction in antibodies levels and increment in C3, C4 levels in initial weeks of treatment, which normalises after 4–6 weeks of corticosteroids therapy. 31
Neutrophil-derived CPD available in automated haematology analyser reflects inner cytoplasmic granularity of neutrophils and cellular nucleic acid (DNA/RNA) contents. These numerical parameters provide quantitative information concerning the morphological and functional characteristics of neutrophils. The change in these numerical values corresponds to the morphological and functional transformation of the leukocytes activated in response to infection and inflammatory processes. 32
Our study has explored the usefulness of neutrophil-derived parameters, reported by the XT Sysmex analysers. The differences found when comparing the median values for the patients with LN and without LN, the control group indicate that those differences reflect changes in structure and morphology of leucocytes in the event of renal involvement.
Similar to studies by Luo et al. 33 and Ngyun et al. 34 , who reported high values of leucocyte-derived parameters and total leucocyte count in sepsis and cardiac complications respectively, our study also showed increased Neut-X, Neut-Y and Neut-Z values in SLE patients with high disease activity related to renal involvement. This diversity in neutrophil parameters is probably due to release of inflammatory cytokines, which lead to increase in intracytoplasmic and intranuclear granularity, ultimately leading to increase in synthesis of cytokines and reactive oxygen species. 35
Neutrophil-derived parameters showed a high area under curve (AUC) for Neut-X (0.710) and Neut-Z (0.707) for discriminating SLE patients with LN from without LN in our study. The large volume of neutrophils and their marked variations in patients with nephritis, than in without nephritis patients and healthy subjects gave the best results in the ROC analysis, with a high sensitivity for the detection of active inflammatory conditions, similar to studies by Park et al. 36 and Cevlik et al. 37
An important information that arises from this study is that there is a compelling association between neutrophil-derived parameters and SLE disease activity, which discloses a promising and noteworthy application for prognosticating renal involvement in SLE patients. A study by Buoro S et al. 38 on liver dysfunction in sepsis patients would apparently reflect a clinical worsening similar to our study.
It is imperative to emphasise that the diagnostic effectiveness of these parameters seems to be partly associated with the LN patients. Therefore, their utilisation should always be accompanied by careful assessment of the presence or absence of renal dysfunction.
Though renal biopsy is definitive for assessment of renal involvement in SLE patients, it is an invasive and time-taking method, while CPD parameters constitute a non-invasive, considerably faster and more easily accessible biomarker of the prediction of LN. CPD parameters are automatically and routinely generated along with the CBC results on various automated haematology analysers, so measurement of these parameters would provide rapid and cost-effective information to the clinicians regarding disease activity and to assess prognosis of LN patients.
Due to complexity of SLE disease and variability of disease, inaccurate conclusions might be generated. So for SLE, a large-scale study should be implemented in future to validate our study results through multicentre and prospective studies.
Conclusion
To the best of our knowledge, the relationship between neutrophil-derived parameters and renal involvement in SLE patients has not been elucidated previously. Therefore, we explored the effectiveness of Neut-X, Neut-Y and Neut-Z in SLE patients, and explored their association with inflammatory markers in LN patients. Our study shows that neutrophil-derived parameters have potential to be used as novel, cost-effective inflammatory, disease activity as well as non-invasive biomarkers for predicting renal involvement in SLE patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.