
Abstract
Lupus erythematosus is an autoimmune disease characterised by the formation of various autoantibodies, leading to the involvement of numerous organ systems like the nervous system, renal system, and cutaneous involvement. Cutaneous involvement is the second most common manifestation after musculoskeletal involvement and can range from minor involvement to severe disabling sequelae. The type of skin manifestation can sometimes predict the underlying systemic involvement, as most patients of acute lupus erythematosus have concomitant systemic involvement in contrast to limited chronic cutaneous LE, which has a low incidence of systemic involvement. The cutaneous manifestations have been included in the Systemic Lupus International Collaborating Clinics (SLICC) and American College of Rheumatology criteria for ease in diagnosing lupus erythematosus patients. Herein, we present a review of various cutaneous manifestations seen in association with systemic lupus erythematosus (SLE) patients and their specific management, which can ease the early diagnosis of the patients and triage the patients that will need close follow-up for systemic involvement.
Keywords
Introduction
Lupus erythematosus is a distinct group of autoimmune diseases characterised by varied autoantibody formation involving several organ systems. The disease spans a spectrum of minor organ involvement (cutaneous) to disabling and life-threatening organ involvement (renal, central nervous system). 1
Cutaneous LE can manifest isolated or be accompanied by other major organ involvement. The musculoskeletal system ranks highest in terms of frequency of involvement, followed by skin. Nearly 80% of patients with systemic lupus erythematosus (SLE) manifest symptomatic skin and mucous membrane lesions at least once in their disease course. The skin lesions can sometimes be disabling, leading to permanent disfigurement owing to the secondary scarring associated with chronic lesions.
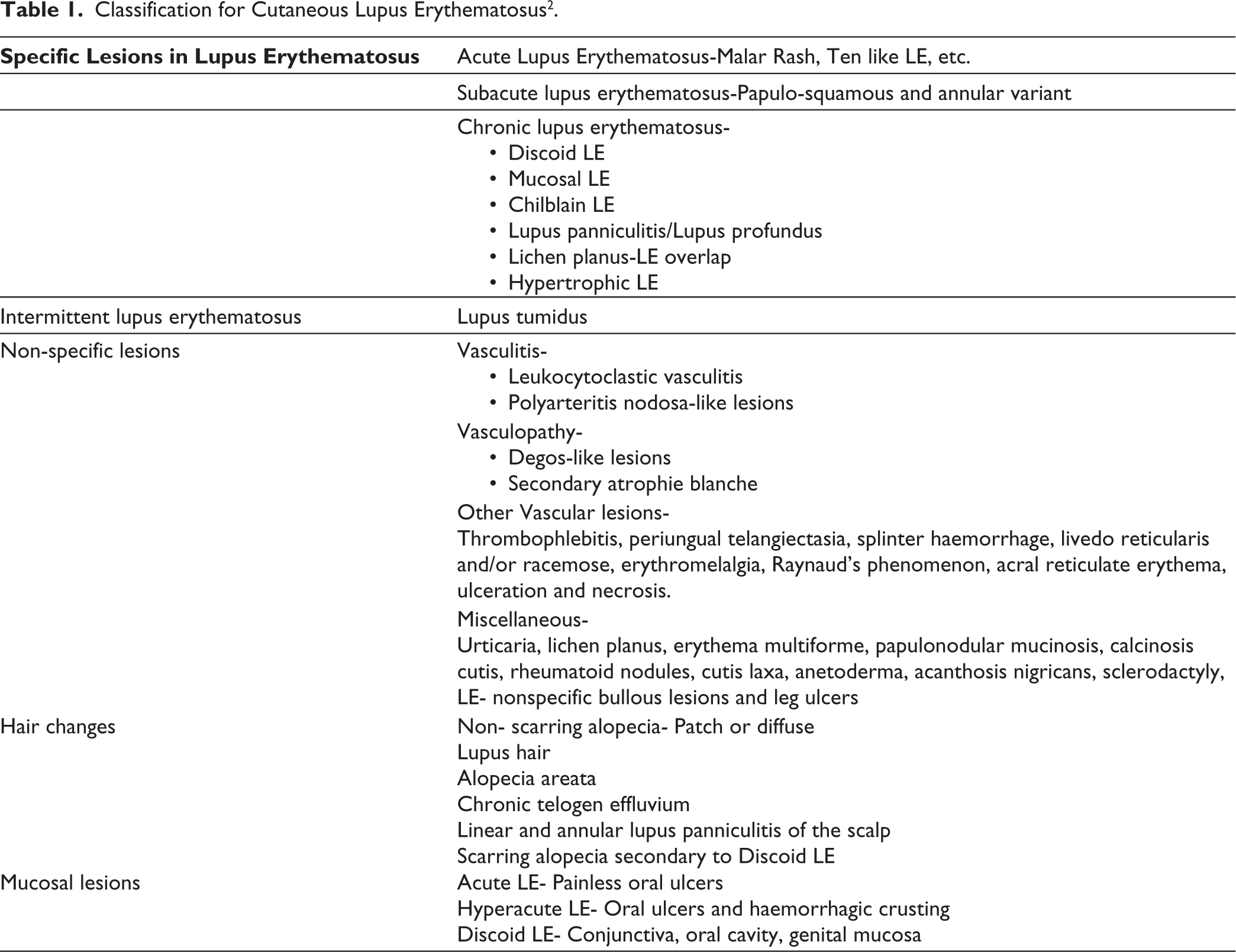
The most widely accepted classification for cutaneous LE is given by Gilliam et al., which classifies cutaneous LE into two major subtypes: LE-specific lesions and LE non-specific lesions based on the presence of interface dermatitis on histopathology. LE-specific lesions are further subclassified into acute, subacute and chronic cutaneous LE (Table 1). 2
Classification for Cutaneous Lupus Erythematosus 2 .
Acute LE
Malar rash is popularly known as butterfly rash due to its bilateral symmetrical distribution over the central face. It typically presents over the nose, cheeks, malar areas, and chins with sparing of nasolabial folds. Morphologically characterised by fixed discrete small erythematous macules or papules and coalescing to form more widespread confluent patches and plaques over the areas as mentioned above (Figure 1). 3 Erichetti et al. have delineated dermoscopic findings of malar rash. The key findings included folliculocentric salmon/reddish-coloured dots surrounded by white halos in an inverse strawberry pattern in 53.9% of the cohort. This pattern was significantly typical in SLE malar rash and revealed a specificity of 86.7%. 4
Malar rash is one of the pivotal manifestations and has been included in all the classification criteria for diagnosing SLE, that is, American College of Rheumatology (ACR) criteria and Systemic Lupus International Collaborating Clinics (SLICC) criteria.5, 6
Erythematous Plaques with Mild Scaling Present Over the Cheeks, Nose and Eyebrows Suggestive of Malar Rash in a Patient with Acute Lupus Erythematosus.

Acute LE can be extensive at times and involve other body parts like extremities and the trunk. Rarely, there has been a description of a hyperacute variant in which the epidermis is detached from the dermis at the level of the dermo-epidermal junction and mimics toxic epidermolysis necrolysis (Figure 2). It can be differentiated from the TEN by the presence of photo exacerbation of the lesions, minimal mucosal involvement, and characteristic histopathological findings of LE. 7
Toxic Epidermal Necrolysis like Lupus Erythematosus with Flaccid Vesicles and Bullae over an Erythematous Background.

Most patients having acute LE have concomitant systemic involvement and high titres of anti-nuclear antibodies. These lesions heal with or without residual pigmentary changes (Figure 3).
Hyperpigmentation Over the Face in a Patient as a Sequelae to Acute Lupus Erythematosus.

Subacute LE
Classically, two morphological variants have been described in the literature: papulosquamous and annular. These lesions are distributed in photosensitive areas over the face, trunk, and upper extremities. The primary morphology of these lesions is a circumscribed erythematous plaque mostly arranged in an annular configuration (Figure 4). They sometimes present with vesiculation, crusting, and/or desquamation. A considerable number of patients show positivity for anti-Ro/La antibodies, and up to 50% will have underlying systemic involvement. A meticulous drug history (terbinafine, calcium channel blockers, angiotensin-converting enzyme inhibitors, antiepileptics) must be elucidated, as up to a third of patients have drug-induced subacute LE. With appropriate treatment, these lesions resolve with subtle pigmentary alterations and rarely with atrophy.
Erythematous Scaly Plaques of Subacute Cutaneous Lupus Erythematosus Over the Upper Back.

Chronic LE
Chronic LE encompasses numerous morphological variants, with localised cutaneous LE ranking highest in frequency of involvement.
Chronic Cutaneous LE
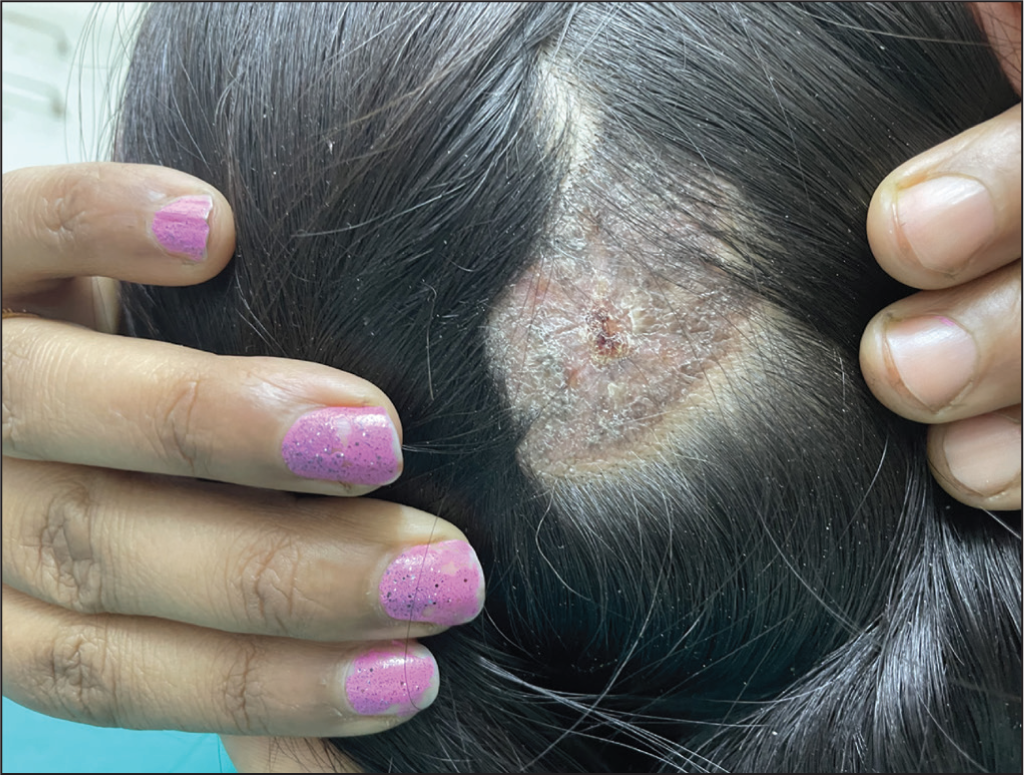
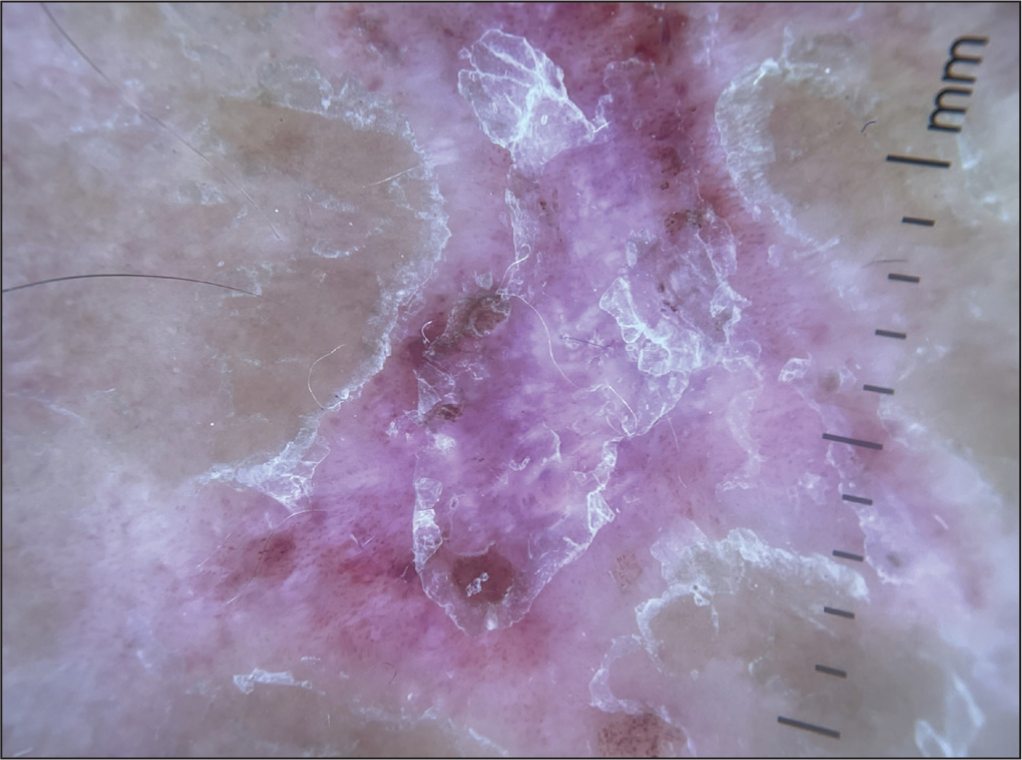
CCLE is presents as well-circumscribed erythematous plaques with adherent scales with atrophy, scarring, and pigmentary changes as sequelae (Figure 5). Dermoscopy (Figure 6) of these lesions reveals follicular plugging, perifollicular scaling, absent follicular opening later on, white structureless areas, pink to white background, brownish pigmentation, and arborising vessels. 8 The localised variant involves the scalp, head, and neck area. The other variant described is the disseminated chronic cutaneous LE, which involves areas below the neck, most commonly the hands. The risk of systemic involvement is low, with the exception of the disseminated variant, where it can reach up to 30%. Additional factors that increase the risk of SLE are anti-nuclear antibody positivity, periungual involvement, joint pain, anaemia, and low white blood cell counts. 9 Rarely, sequelae of these lesions can be non-melanoma skin cancer, which needs to be differentiated from hypertrophic cutaneous LE as the former carries a poor prognosis. 10
Well-Circumscribed Erythematous Scaly Plaques of Discoid Lupus Erythematosus Over the Scalp Leading to Scarring Alopecia.
Dermoscopy of Discoid Lupus Erythematosus Revealing White Structureless Areas, White and Pink Background, Whitish Scales and Multiple Blood Vessels.
Lupus Panniculitis/Lupus Profundus
Lupus panniculitis characteristically presents as erythematous painful indurated nodules predominantly involving upper body fat-rich areas. Sometimes, these nodules have overlying plaques of discoid LE, making them lupus profundus. Delay in diagnosis is relatively common, leading to lipoatrophy and calcinosis with profound disfigurement. 11
Hypertrophic LE
It is one of the rare variants of LE, which involves extensors of the upper limb and upper trunk. 12 Clinically, it presents as verrucous indurated plaques (Figure 7), which sometimes can be mistaken as squamous cell carcinoma. 10
Hypertrophic Lupus Erythematosus at the Angle of Mouth.

Chilblain LE
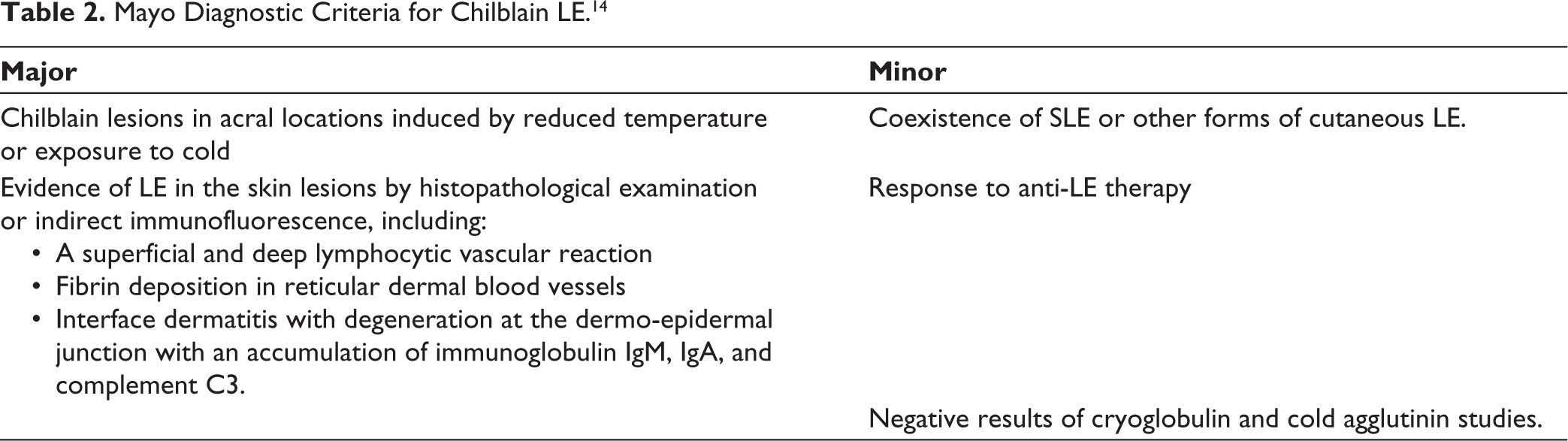
Chilblain LE has been described in two forms—familial and sporadic. Familial form is seen in childhood, secondary to heterozygous mutations in gene TREX1. 13 Sporadic form is proposed to result from microvascular injury due to immunological damage to the vessel wall. It manifests as erythematous to violaceous pruritic or painful plaques distributed symmetrically predominantly over the dorsal aspects of hands and feet. Like chilblains, it is precipitated by cold and damp weather but can persist in hot conditions. Mayo diagnostic criteria proposed for diagnosing chilblain LE, encompasses two major and three minor criteria (Table 2). 14 Definitive diagnosis is made when both major and at least one minor criterion are fulfilled. 14 Once diagnosis is established, cold protection and topical steroids remain the mainstay treatment. The risk of developing systemic LE is up to 20% in patients with chilblain LE; hence, it should be carefully followed up. 15
Mayo Diagnostic Criteria for Chilblain LE. 14
Lichen Planus-lupus Erythematosus Overlap
To date, less than 50 cases have been reported in the literature. This syndrome is characterised by a chronic disease process that exhibits overlapping features of both the diseases clinically and histologically. Jicha et al. defined a set of clinical, histopathological, serological, and direct immunofluorescence features comprising diagnostic criteria. 16
Lupus Tumidus
It is clinically characterised by photosensitive erythematous urticarial non-scaly plaques with excellent response to anti-malarials and resolves without dyspigmentation and atrophy. 17
According to Gilliam and SLICC 2012, it has been classified as one of the types of chronic cutaneous LE. Its classification has been under debate recently due to its clinical and immunological features. It has a relapsing and remitting course, mostly lacking underlying systemic involvement and a predominantly negative autoantibody profile. 18 Histologically, it is different from other specific lesions of LE by the presence of abundant mucinous deposition in the dermis and minimal epidermal alterations. 19 It is thus sometimes considered a form of intermittent LE rather than chronic cutaneous LE. 20
Non-specific Lesions
Numerous other dermatological manifestations occur in patients with systemic LE. These are non-specific, as these can be seen with other disorders as well. Vascular involvement can be both cutaneous and visceral, sometimes life-threatening.
Vascular events occur either due to the inflammation leading to vasculitis or secondary to thrombosis indicating vasculopathy. When signs indicate vasculopathy, antiphospholipid antibodies should be looked for. Even if these antibodies are absent, patients should be observed as having high vascular risk. 21
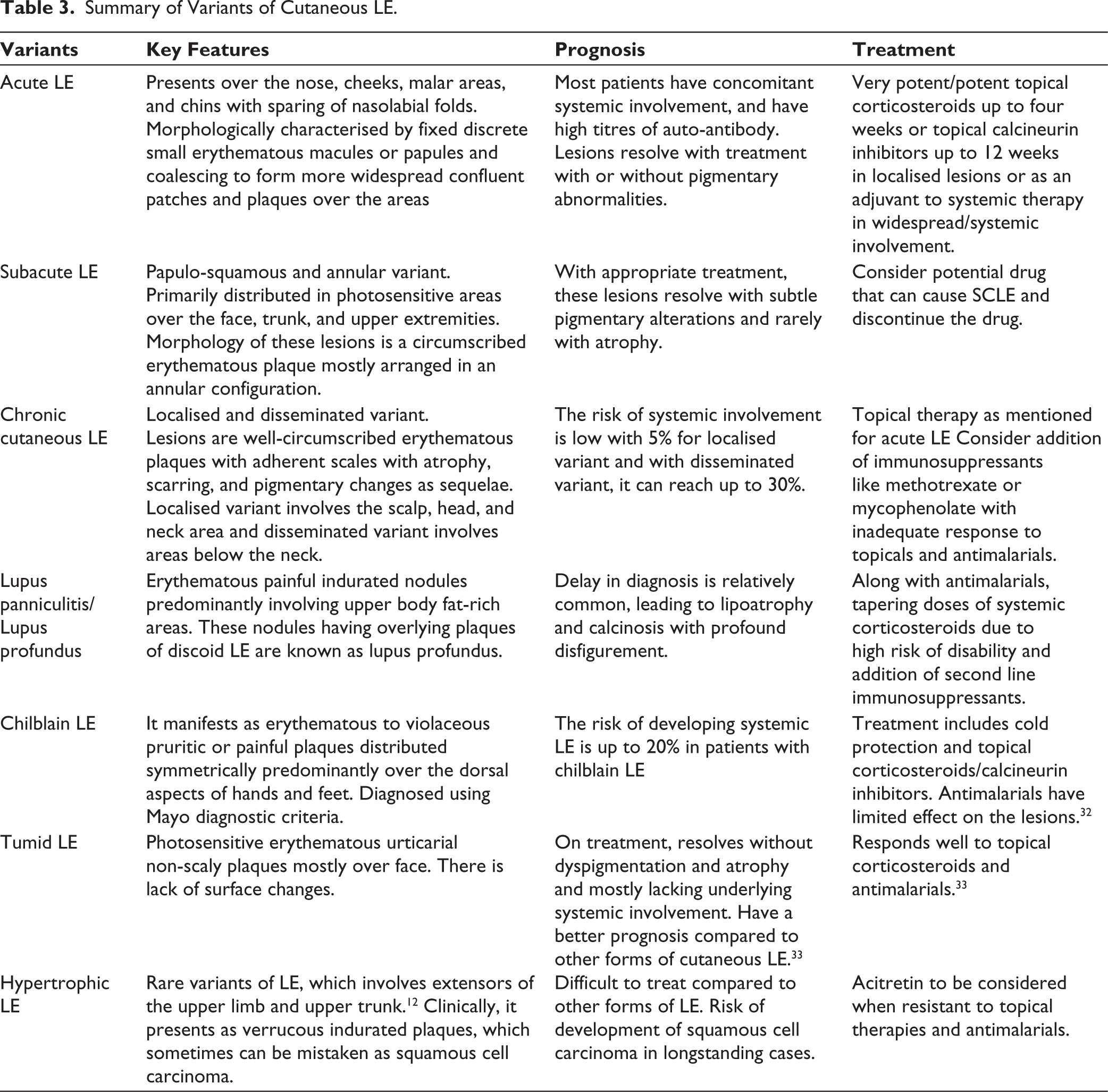
Summary of Variants of Cutaneous LE.
Typical manifestations of vasculopathy are degos-like lesions and secondary atrophie blanche (Figure 8). Vasculitis can present as leukocytoclastic vasculitis- urticarial vasculitis and palpable purpura or polyarteritis nodosa-like cutaneous features. Other vascular lesions that can be seen are thrombophlebitis, periungual telangiectasia, splinter haemorrhage, livedo reticularis and/or racemose, erythromelalgia, Raynaud’s phenomenon, acral reticulate erythema, ulceration, and necrosis.2, 22
White Atrophic Scar with Surrounding Erythema and Hyperpigmentation in a Reticulate Pattern Over the Dorsum of Feet Suggestive of Atrophie Blanche.

Other dermatological manifestations that present in association with LE and are included in Gilliam’s classification are non-scarring hair loss, urticaria, lichen planus, erythema multiforme, papulonodular mucinosis, calcinosis cutis, rheumatoid nodules, cutis laxa, anetoderma, acanthosis nigricans, sclerodactyly, LE- non-specific bullous lesions and leg ulcers (Table 1). 2
Hair Involvement in LE
Hair loss in SLE is a well-recognised entity and, thus, has always been incorporated into different classification criteria for SLE. 5 SLICC 2012 has incorporated four mucocutaneous manifestations in their classification criteria, one of which is non-scarring alopecia. It has been defined as diffuse thinning or fragility of hair with noticeably broken hairs without other causes, such as androgenetic alopecia, iron deficiency, drugs, and alopecia areata. 5
Non-scarring alopecia can sometimes cause patchy involvement in which the pathogenesis is similar to diffuse non-scarring alopecia but confined to an area. These patches show subtle erythema and scaling with hair thinning and are associated with the initial presentation of SLE or during the flare-up of the disease. The main differential diagnosis of this pattern of hair loss is alopecia areata, which itself has been reported to occur in higher frequency in patients with SLE. Whether the patchy, non-scarring alopecia is a distinct entity from the alopecia areata or is an overlapping entity needs to be elucidated in further studies. 23
Lupus hair is a type of non-scarring alopecia characteristically seen in patients with chronic active systemic LE. It is detected in the frontal hairline and is defined by the presence of short, lustreless, and brittle hair (Figure 9). Occasionally, slight erythema can be seen in the background. Other parts of the scalp may be involved but are usually less conspicuous. The treatment is aimed at controlling the lupus flare. 24
Short Lusterless Hair Over the Frontal Hairline.

A rarely reported entity is linear and annular lupus panniculitis of the scalp. This presents as a non-scarring alopecia, presumably along the lines of Blaschko of the scalp in a linear, arciform, or annular shape. The pathology is located in the subcutaneous tissue much below the hair stem cells; hence, scarring is not observed. The development of SLE is the least with this type of hair loss. It has been successfully treated with oral antimalarials with intralesional and/or oral corticosteroids. 25
Scarring alopecia is seen when the discoid LE plaques involve the scalp area, as mentioned above in the heading of chronic cutaneous LE.
Mucosal Involvement in LE
Mucosal involvement is not uncommon in LE, occurring in up to 45% of individuals. Oral lesions in systemically ill LE patients can manifest in various morphologies vis oral erosions or ulcerations, palatal or diffuse erythema, purpuric macules, and circumscribed red areas. These can involve the oral cavity symmetrically and sometimes be present without cutaneous involvement. The so-called hyperacute LE can have severe involvement of oral mucosa and presents with erosions and haemorrhagic crusting.
Chronic LE can involve oral, conjunctival, and genital mucosa in the form of discoid LE. It manifests as well-demarcated plaques with central atrophy or ulceration and peripheral radiating white streaks and telangiectasia (Figure 10). It is mainly distributed asymmetrically over hard palate (Figure 11), buccal mucosa, and lips. Rarely, squamous cell carcinoma may arise in chronic lesions. 26
Erythematous Plaques in the Buccal Mucosa with White Radiating Striae.

Erythematous Plaque of Lupus Erythematosus Over the Hard Palate.

Nail Involvement in LE
Although many nail abnormalities have been reported in the SLE, none is characteristic of the disease. Nearly 25% of SLE patients show nail involvement. It can present as onycholysis, onychomadesis, subungual hyperkeratosis, leukonychia, nail pitting, and longitudinal ridging. 27
Management
Since lupus erythematosus is a disease that involves multiple systems, patients presenting with cutaneous LE should be screened for underlying systemic involvement, although the risk varies with the type of cutaneous presentation. Essential blood and urine investigations for haematological and renal abnormalities and anti-nuclear antibodies are to be done for the screening. A multi-disciplinary approach is needed for the systemic involvement, and depending on the severity, treatment is instituted. For cutaneous involvement, the treatment is directed according to the type of lesions. 28 General recommendations for all forms of LE remain photoprotection using daily preventive (chemical and physical) sunscreens and avoidance of unprotected UV exposure. Vitamin D supplementation is recommended with all forms of cutaneous LE. Topical corticosteroids (very potent/potent) are recommended for the localised lesions for up to four weeks or topical calcineurin inhibitors are recommended for up to 12 weeks. With the disseminated lesions or systemic involvement or risk of scarring, antimalarials are added in addition to the topical therapies. Antimalarials (hydroxychloroquine up to 5 mg/kg body weight or chloroquine 2.3 mg/kg body weight) is recommended in severe or widespread or high-risk of systemic involvement. In addition to antimalarials, systemic corticosteroids therapy is recommended for severe or widespread involvement but long-term use is not recommended in isolated cutaneous involvement.14, 29 Second-line immunosuppressants methotrexate or mycophenolate are to be used on a case-to-case basis. Third-line therapy in refractory cutaneous LE cases include thalidomide/lenalidomide, intravenous immunoglobulin, clofazimine or biologics like belimumab. 29 Azathioprine, cyclosporine or cyclophosphamide is not recommended for cutaneous LE without systemic involvement. 30 Treatment options are to be tailored according to the types of LE like dapsone for bullous lesions of LE and intralesional corticosteroids/acitretin for hypertrophic LE. 31 Since, lupus panniculitis/profundus leads to severe disfigurement and is resistant to first-line antimalarials; immunosuppressants are added early, whereas localised chronic cutaneous LE is managed with topical immunomodulators. 11 Vascular involvement treatment depends on the underlying pathology, ranging from cold protection for Raynaud’s phenomenon to anticoagulants/antiplatelets for thrombotic vasculopathy, and immunosuppressives for vasculitis. Prognosis largely depends on the vascular involvement of the central nervous or renal system. 22
As it is well known that skin can be a window of diagnosis of many underlying systemic disorders, the knowledge regarding various cutaneous manifestations is vital as many times leads to early diagnosis or helps monitor exacerbations of underlying systemic disorders. This write-up portends to exemplify the fact that at each stage in LE there are distinct cutaneous manifestations which is of at most importance for the treating physician for, for example, a case of LE presenting as TEN which can be mistaken for drug-induced thus causing a significant delay in diagnosis of LE and leading to mortality. Similarly, various typical and non-typical cutaneous manifestations of SLE have been highlighted which can be present much earlier before the patient develops the systemic manifestations of SLE. In LE, depending on the type of cutaneous manifestations, the probability of developing systemic LE changes and helps in prognosticating the patient. Hence, the cutaneous examination and ideas regarding various cutaneous lesions in LE are pertinent for physicians.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Statement
The patients in this manuscript have given written informed consent to publication of their case details and photographs.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.