
Abstract
Background:
Paediatric systemic lupus erythematosus (pSLE) is a heterogeneous, chronic autoimmune disease characterised by multi-system inflammation and the production of antibodies-directed self-antigens. Anti-C1q has been associated with SLE as well as other connective tissue diseases. They have been considered as a marker for disease activity and the presence of nephritis.
Objectives:
To determine the prevalence of anti-C1q antibodies in the paediatric SLE and to determine clinical associations of elevated anti-C1q antibody levels, especially with lupus nephritis.
Methods:
All consecutive children with SLE on treatment with immunosuppressive drugs attending our clinic were recruited. After obtaining informed consent, blood samples were tested for anti-C1q antibodies by a commercially available ELISA kit. The prevalence of anti-C1q and its association with lupus nephritis were determined.
Results:
Out of a total 150 children with SLE, anti-C1q positivity was present in 95 children (64%), at a cut-off value of 20 U/mL. Children with proteinuria, low C3, low C4 and anti-dsDNA positivity had significantly more anti-C1q antibody positivity. Children with lupus nephritis were significantly more likely to have anti-C1q antibody positivity than children without renal involvement (74% vs. 51%, p = .02). Among the children with lupus nephritis, children with active renal disease were more likely to have anti-C1q positivity than in children with quiescent disease (88% vs. 53%, p = .002). Anti-C1q antibodies had a sensitivity of 74% and specificity of 54% at a cut-off value of 22 U/L for renal disease in pSLE.
Conclusion:
In our study, children with lupus nephritis were significantly associated with elevated anti-C1q antibodies, and children with active renal disease had higher anti-C1q positivity than those with quiescent disease. Anti-C1q levels showed significant associations with low C3, low C4 and anti-dsDNA positivity. Anti-C1q levels did not show significant associations with clinical features of SLE like malar rash, arthritis and CNS involvement. Anti-C1q antibody titres were found to have a positive correlation with renal disease and hence could be used as an adjunctive biomarker in monitoring the disease activity in children with lupus nephritis.
Introduction
Systemic lupus erythematosus (SLE) is a chronic, autoimmune disease characterised by multi-system inflammation and the production of autoantibodies directed against self-antigens. Children with SLE have a more severe disease process and greater organ involvement than adults. Renal disease has been found to be more common in paediatric SLE than in adults. 1 Deficiency of early complement components is genetically associated with the development of SLE. 2 Individuals with a deficiency of C1q, the first component of the classical complement pathway, have the highest prevalence of SLE and the most severe disease manifestations. The strongest association is seen in patients with homozygous C1q deficiency, of whom 88% developed SLE and 30% developed glomerulonephritis. 3 Acquired antibodies against the collagen-like region of C1q were present in the glomerular basement membrane of patients with proliferative lupus nephritis, at a much higher concentration than in the serum, suggesting a role for this antibody in the pathogenesis of lupus nephritis. 4 C1q were aggregated within immunoglobulin G in renal sub-endothelial deposits in active proliferative lupus nephritis, as seen on electron microscopy, further supporting a pathogenic role of anti-C1q. 5 The presence of anti-C1q at the time of renal biopsy was associated with worse renal outcomes by the ACR renal response criteria. 5 Patients with active lupus nephritis had a higher prevalence of anti-C1q than those without lupus nephritis, 74% versus 32% (p < .0001). 6 Anti-C1q increased almost six months prior to renal involvement in 50% of patients with SLE 7 and was associated with proliferative forms of lupus nephritis. 8 Anti-C1q concentration correlated with activity on modified SELENA Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and the SLICC renal activity score. 9 There is no published trial evaluating the role of anti-C1q in Indian children with SLE. Hence this study is being undertaken to evaluate and understand the role of this antibody as a marker for lupus nephritis in paediatric SLE and to elucidate its association with other clinical manifestations of SLE.
Materials and Methods
This observational study was conducted in the Pediatric Rheumatology unit of Christian Medical College, Vellore, over a period of two years. All children aged 6–18 years of age diagnosed with SLE according to the ACR criteria were included after obtaining parental consent. 5 Convenience sampling technique was used. All children with SLE on immunosuppressive drugs presented to our paediatric rheumatology OPD irrespective of disease status were recruited after consent. Children with congenital complement deficiencies were excluded.
Clinical and laboratory data were collected from children fulfilling the inclusion criteria and entered into a proforma. Clinical and laboratory test details were retrieved from the electronic medical records of our hospital. After obtaining parental consent, blood samples were sent to anti-C1q antibodies. The disease activity of SLE was assessed using the SLEDAI. Anti-C1q antibody assay was done by a commercially available ELISA kit (IMTEC-anti-C1q-antibodies 9ITC590330, Germany). A reference level of 20 IU/mL was taken as the cut-off as recommended by the manufacturers. A level of assay of more than 20 IU/mL was taken as positive. Anti-C1q levels were compared to clinical and laboratory parameters.
As per the ACR criteria, lupus nephritis is defined as persistent proteinuria (>0.5 g/day, or spot UP/UC > 0.5 or >3+ by dipstick) and/or—casts (cellular, RBC, granular or mixed casts).
Active lupus nephritis was defined as the presence of urinary casts, haematuria (>5 RBC/HPF) or proteinuria (urine protein/creatinine ratio of >0.2, whereas inactive renal disease was taken as the absence of the above-mentioned.
Statistical Methods
Demographic and clinical characteristics are reported as median and range or n (%), as appropriate. Continuous variables are presented as mean with standard deviation or median with interquartile range based on the distribution of data. The association of anti-C1q with various clinical manifestations was obtained by calculating odd’s ratio, adjusted for confounders by performing logistic regression analysis. The sensitivity and specificity with a 95% confidence interval for anti-C1q antibodies in renal lupus were obtained. p Values <.05 were considered to be statistically significant. All statistical analysis was done using SPSS software analyses.
Results
During our study period, a total of 150 children with SLE on immunosuppressive drugs who fulfilled ACR criteria were recruited. Their baseline characteristics are summarised in Table 1.
Baseline Characteristic Features of Children with SLE.
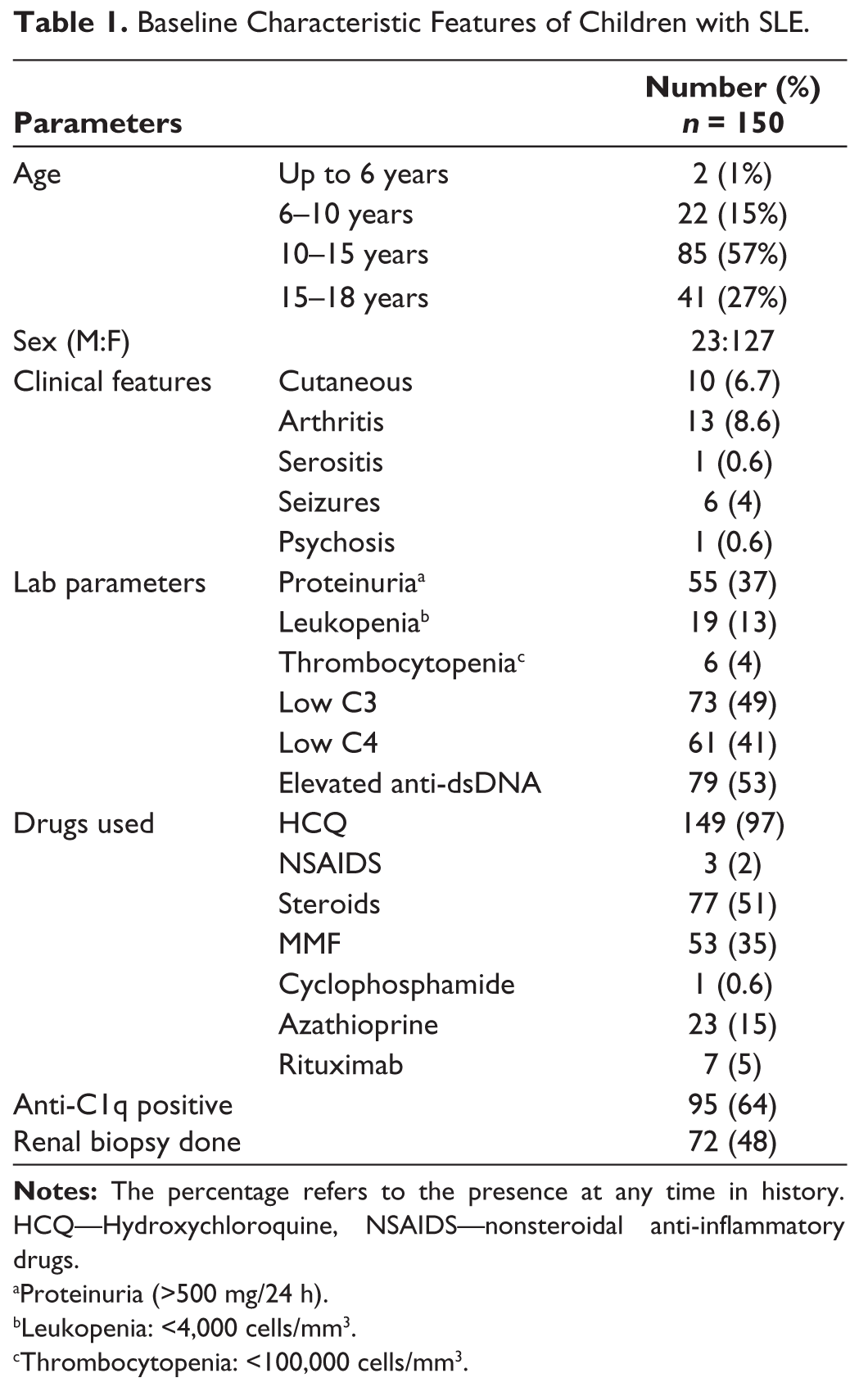
aProteinuria (>500 mg/24 h).
bLeukopenia: <4,000 cells/mm3.
cThrombocytopenia: <100,000 cells/mm3.
Among the 150 children enrolled, the majority (84%) were females, and 57% were in the 10–15 year age group. Rash (6.7) and arthritis (8.6%) were the most common clinical manifestations. Anti-dsDNA levels were elevated in 53% of children, followed by low C3 in 49% of children and proteinuria in 37%. Overall, 97% of children enrolled were on HCQ, 51% on steroids and 35% on MMF.
Out of 150 children with paediatric SLE (pSLE), 72 underwent renal biopsy because of lupus nephritis. A total of 7 (10%) had Class II lupus nephritis, 21 (28%) had Class III, 40 (54%) had Class IV and 4 (6%) had Class V lupus nephritis. Anti-C1q was positive in 59 (82%) of children who had undergone renal biopsy.
Clinical and Laboratory Associations of Anti-C1q
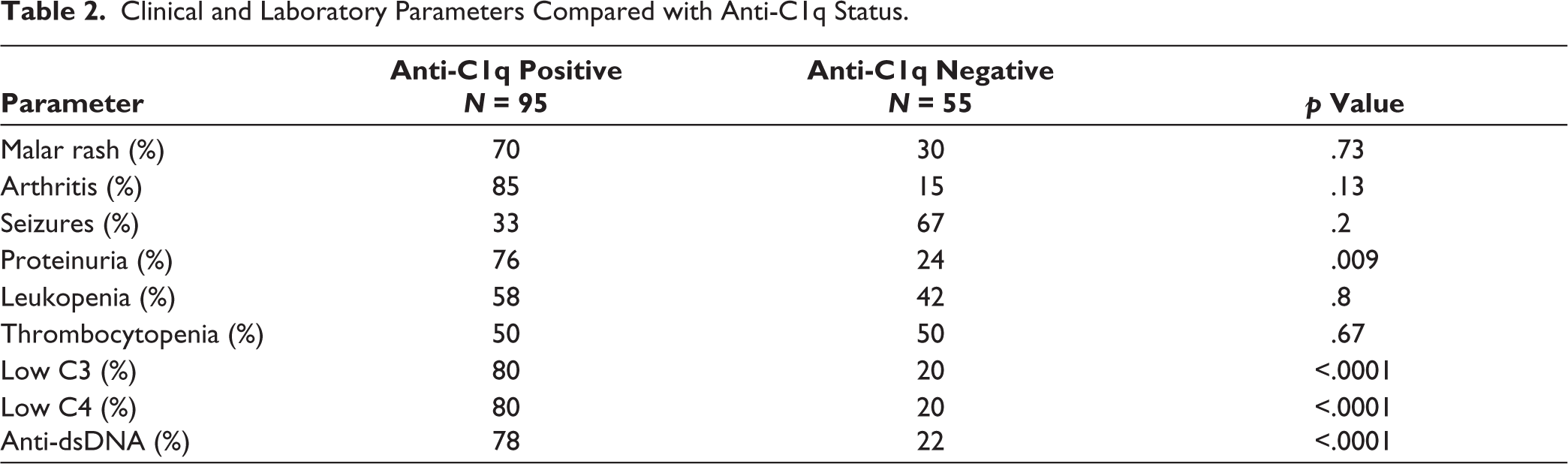
Associations of anti-C1q with various clinical features are listed in Table 2.
Anti-C1q levels did not show significant associations with clinical features of SLE like malar rash, arthritis, CNS involvement or blood involvement. However, anti-C1q levels showed significant associations with other serological parameters like low C3, low C4 and anti-dsDNA positivity.
Relation Between Positive SLEDAI and Anti-C1q Antibody Titres
The relation between positive SLEDAI and anti-C1q antibody titres was shown in Table 3.
Clinical and Laboratory Parameters Compared with Anti-C1q Status.
Correlation Between Positive SLEDAI and Anti-C1q Antibody Titres.

SLEDAI > 8 is taken as an active disease and <8 as an inactive disease. The mean anti-C1q level was high with children with high SLEDAI (p = .08).
There was no significant correlation between average c1q antibody titres and SLEDAI positivity (r = 0.172) by Pearson correlation.
Anti-C1q in Patients with Renal Involvement
Anti-C1q titres in patients with SLE with and without renal involvement are shown in Figure 1.
Anti-C1q Status in pSLE with or Without Renal Involvement.
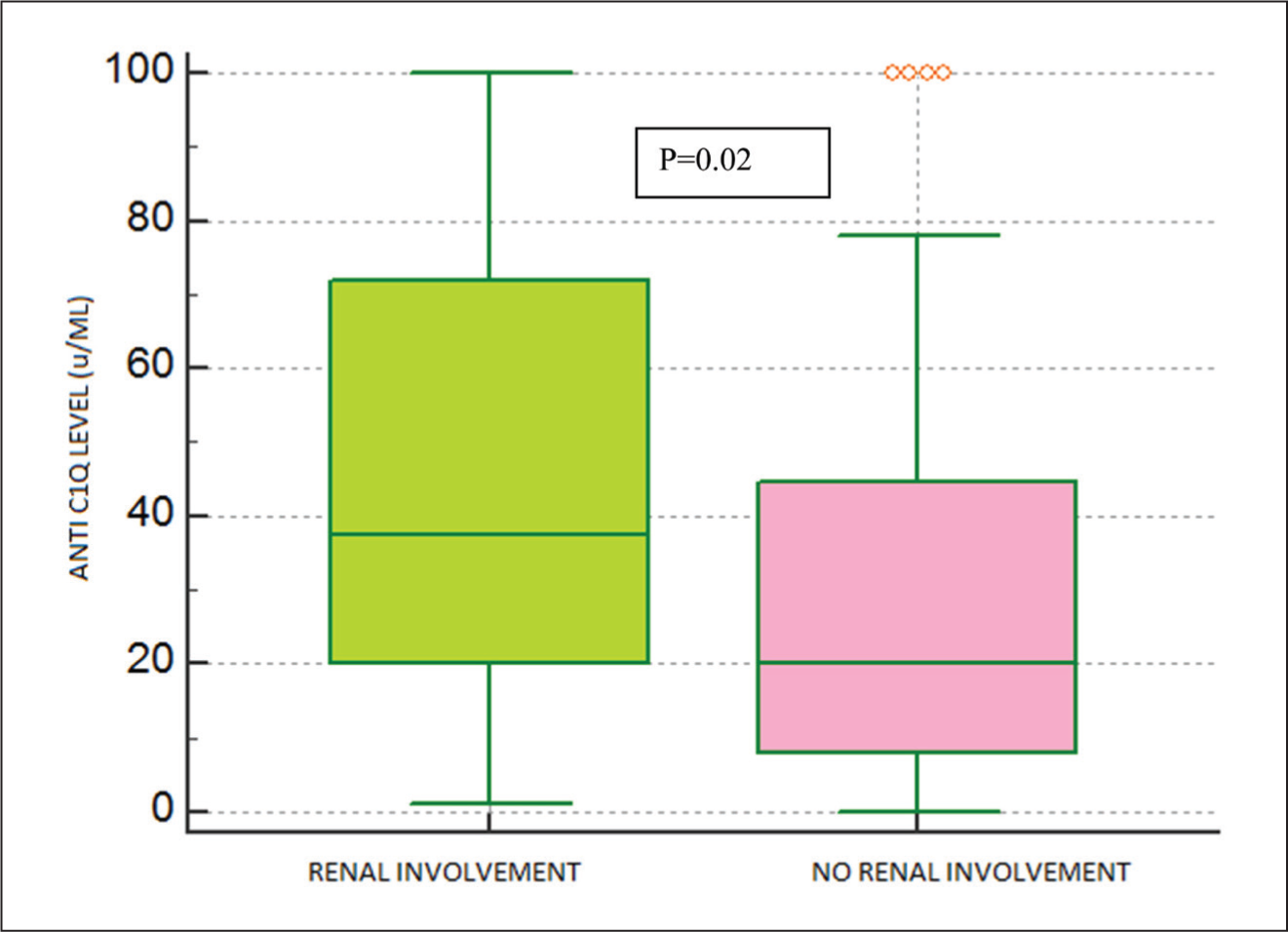
Lupus nephritis was significantly associated with elevated anti-C1q antibodies (p = .001, RR 1.7, 95% CI 1.2–2.6).
Lupus nephritis was significantly associated with elevated anti-C1q antibodies (p = .001, RR 1.7, 95% CI 1.2–2.6).
Anti-C1q in Children with Active Lupus Nephritis
Anti-C1q titres in patients with SLE with active and inactive lupus nephritis are shown in Figure 2.
Anti-C1q Status in pSLE with Active or Inactive Renal Disease.
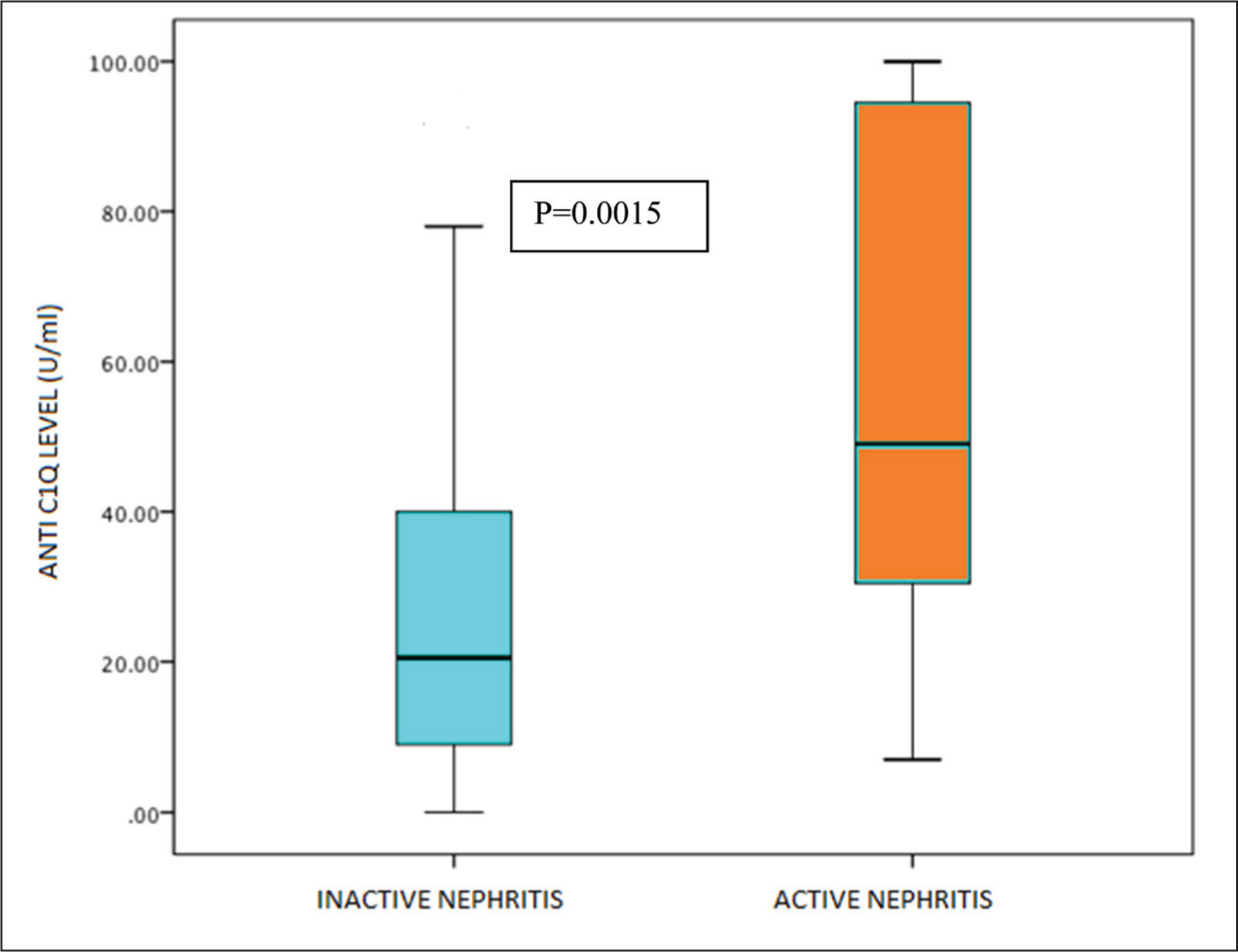
Among the children with lupus nephritis, children with active renal disease had more significant anti-C1q positivity than children with quiescent disease (88% vs. 53%, p = .002). Levels of anti-C1q in children with active lupus nephritis were higher than in children with inactive disease.
Sensitivity and Specificity for Anti-C1q
Sensitivity and specificity for anti-C1q levels were derived from the ROC curve as shown in Figure 3.
ROC Curve for Sensitivity and Specificity for Anti-C1q Levels.
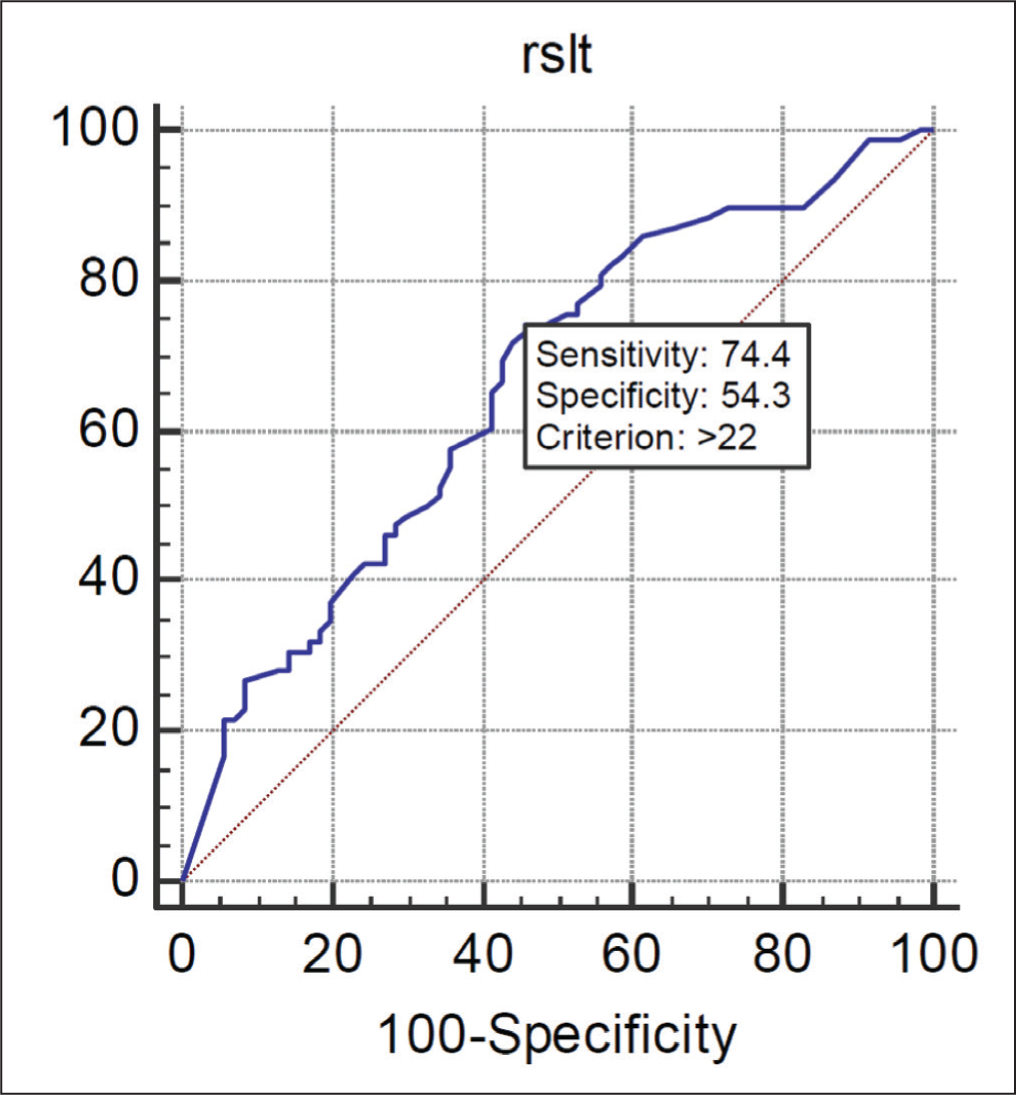
AUC analysis (area under the curve) for positive anti-C1q titres for renal disease was 0.659, with a sensitivity of 74% and specificity of 54% at anti-C1q cut-off of 22 U/L.
Discussion
This observational study was performed to evaluate the diagnostic utility of anti-C1q in the pSLE concerning disease activity and lupus nephritis. Renal involvement was the most common clinical feature with 55 children having active proteinuria at the time of recruitment to the study and 78 children (52%) with established lupus nephritis. This is similar to reports published by Hiraki et al. from Toronto, who described a lupus nephritis incidence of 55% in their SLE population. 10
In our cohort, the malar rash was seen only in 10 children (7%) and none had a discoid rash. In comparison with the study from Toronto, 10 cutaneous manifestations were the most common, with malar rash being seen in 66% of the study population. In the study from West India, the incidence of malar rash was reported at 44%. 11 Arthritis in our study was seen in 13 children (9%), which is again less than that reported previously in the literature. Levy et al. reported that the incidence of arthritis was 80% in paediatric SLE while Hiraki et al. reported arthritis in about 67% of children.10, 12 Patwardhan et al. also reported an arthritis incidence of 60% in West India, as did studies from South India.11, 13 CNS manifestations are one of the most dreaded complications of paediatric SLE. In our study, there were six children with seizures and one child with psychosis. Hence CNS manifestations were present in 5% of the study population. In a study from South India on adult SLE, Robert et al. and colleagues reported a seizure incidence of 20% and psychosis incidence of 16%. 14
A total of 72 out of the 150 children with lupus nephritis underwent renal biopsy. Class IV lupus nephritis (diffuse proliferative lupus nephritis) was the most common, followed by Class III (focal proliferative lupus nephritis). In the study by Hiraki et al., Class III and IV nephritis constituted about 80% of the renal biopsy samples. 10 Mean anti-C1q values were found to be higher in Class III and IV lupus nephritis, reflecting a more severe disease course. There was, however, no statistically significant difference between Class III and IV nephritis concerning anti-C1q values.
Antibodies to initial complement factors are increased in patients with SLE. Most of these studies have been undertaken in adults or mixed populations. In our study, 95 of 150 children (64%) had positive anti-C1q titres (>20 U/mL).
Children with lupus nephritis were significantly more likely to have anti-C1q positivity compared with children without renal involvement (74.4% vs. 48.6%, p = .0001, OR 1.77, 95% CI 1.2–2.6). The mean anti-C1q value was also higher in the lupus nephritis group as compared to children without lupus nephritis (46.29 vs. 29.77 U/L) and the difference was statistically significant (p = .011). This is consistent with the study published by Marto and Bertolaccini, where children with lupus nephritis were found to have higher anti-C1q values as compared to children without lupus nephritis. 6
Lupus nephritis was significantly associated with elevated anti-C1q antibodies (p = .001, RR 1.7, 95% CI 1.2–2.6). A total of 59 out of 72 (82%) children with the lupus nephritis group had positive anti-C1q values. Published studies have found anti-C1q positivity in 50%–74%. Mean titres were also significantly increased in the lupus nephritis group as compared to those without renal involvement. This is again consistent with the available literature. AUC analysis (area under the curve) for positive anti-C1q titres for renal disease was 0.659, with a sensitivity of 74% and specificity of 54% at an anti-C1q cut-off of 22 U/L. The positive and negative predictive value of anti-C1q titres in renal disease was both around 65%. In the retrospective study done by Picard et al., anti-C1q titres were positive in 84% of pSLE with active disease and had better specificity than anti-dsDNA in distinguishing patients with lupus nephritis (73% vs. 19%). 15 Proteinuria was present in 55 children, 44 of whom had positive antibody titres. Of the 95 children without proteinuria also, 51 had positive levels of anti-C1q antibody. However, the difference between the groups was statistically significant (p = .0006, RR =1.5, 95% CI 1.19–1.87), though the average antibody titre was not significantly different between the groups in our study.
In our study, we had 10 children with malar rash and there was no significant difference between those with cutaneous disease and those without cutaneous disease concerning antibody positivity. The mean level of anti-C1q titres was also not significantly different between the two groups (42.59 vs. 38.14, p = .89).
SLEDAI > 8 is taken as an active disease and <8 as an inactive disease. The mean anti-C1q level was high with children with high SLEDAI (p = .08).
There was no significant correlation between average c1q antibody titres and SLEDAI positivity (r = 0.172) by Pearson correlation.
Low complement levels are used to assess disease flares in SLE. About half of our study population had low C3 or C4. There were 73 children with low C3 of whom 58 had an elevated anti-C1q value. C1q positivity was found to be significantly higher in children with low C3 as compared to normal C3 (p < .0001, RR—1.8, 95% CI—1.36–2.37). The mean C1q antibody level was also higher in the group with low C3 as compared to the group with normal C3 (54 vs. 24, p = .001). Similarly, there were 61 children with low C4, of which 50 children had positive antibody titres, and the difference was statistically significant (p = .0002, RR 1.6, 95% CI 1.25–2.01). However, the average antibody titre between the groups was not significantly different (54 vs. 28, p = .14).
Children with active lupus nephritis were more likely to have low C3 levels as compared to children with inactive lupus nephritis (p = .0028, OR 2.25). Similarly, the active lupus nephritis group had a significantly higher number of children with low C4, as compared to the inactive nephritis group (p = .0012, OR 5.48). In a recent report, Song et al. found that plasma levels of C3 were lower in patients with active lupus 76 nephritis than in those in remission (0.62 ± 0.37 vs. 1.09 ± 0.18 μg/mL, p < .001). 16 In a retrospective cohort study patients were persistently low complement levels were significantly more likely to have lupus nephritis than patients with normal complement levels. 17
Strengths and Limitations
This is the first prospective study to include 150 children with SLE to evaluate the prevalence and clinical associations of anti-C1q antibodies in pSLE in Indian Children. The relatively small number of patients, in particular when comparing subgroups of patients, does not allow for drawing definite conclusions.
Our study characteristics did not sufficiently allow the calculation of the sensitivity and specificity of anti-C1q for the determination of a specific nature and severity of flares in comparison to other laboratory markers of disease.
Conclusion
Our data support the usefulness of anti-C1q in SLE, especially in lupus nephritis. Our study results revealed that anti-C1q antibody titres were found to have a positive correlation with renal disease in pSLE. Anti-C1q can be used as a follow-up marker in SLE patients, in particular in SLE patients with renal involvement. Hence use of anti-C1q determinations becomes important for clinical care and disease prognosis, anti-C1q can be reconsidered for inclusion in classification criteria and the clinical management of SLE. Further studies have to be performed using well-defined large cohorts of patients with close as well as long follow-ups to determine the diagnostic value of anti-C1q in SLE patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Our Institutional Review Board approved this study (IRB Min No: 10305).
Funding
The authors received no financial support for the, authorship and/or publication of this article.