
Abstract
Objectives:
To assess causes of vaccine hesitancy to COVID-19 vaccines in patients with autoimmune rheumatic diseases (AIRD).
Methods:
Study design: We conducted a cross-sectional observational survey-based study of patients attending Rheumatology OPD regarding the reason for vaccine hesitancy, counselled by treating rheumatologists and responses regarding willingness recorded after counselling. Convenience sampling was done by including all adults (>18 years) with AIRD attending rheumatology OPD. Those vaccinated, recently infected (within six weeks), and non-AIRD patients were excluded. The questionnaire included details about patients’ demography, medication and reason for vaccine hesitancy. Statistical analysis was performed using measures of central tendency for quantitative variables and using counts and percentages for qualitative variables.
Results:
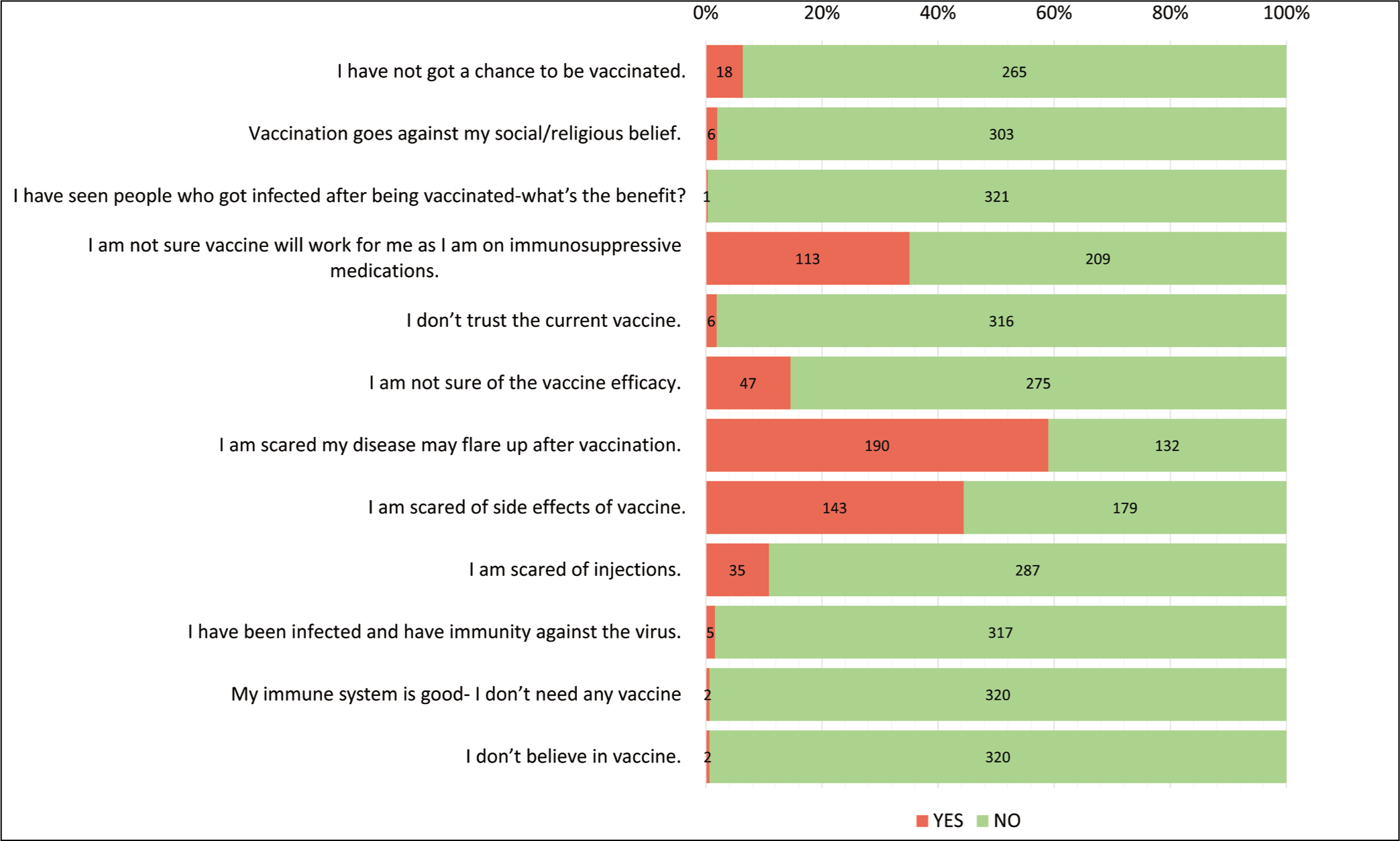
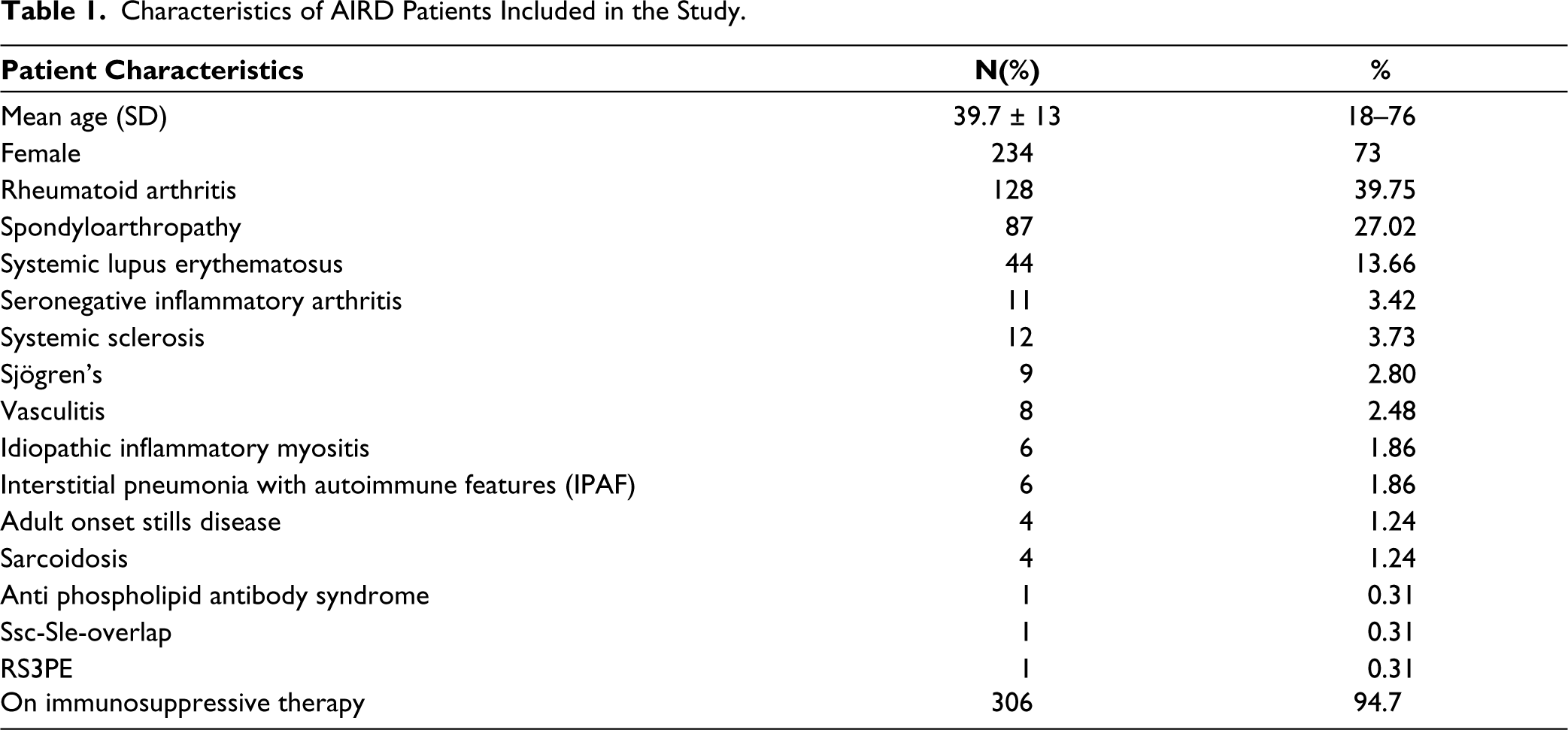
A total of 322 patients participated in the study with a mean age of 40 years (18–76), with 73% (234) females and 27% (88) males. Most patients had RA (40%) followed by SpA (27%), SLE (13%) and were on immunosuppressive medications (95%). A significant proportion of patients (60%) had more than one reason for vaccine hesitancy. Almost 60% of the respondents feared disease flare post-vaccination, while almost half (44.4%) feared vaccine side effects and more than one-third (35%) doubted vaccine efficacy while on immunosuppressive medications. Other causes were the inability to get vaccinated (18%), doubts about vaccine efficacy (15%), and fear of injections (10%). Most patients (91%) expressed vaccine acceptance after specialist counselling.
Conclusions:
Vaccine hesitancy is multifactorial. Addressing reasons for vaccine hesitancy in patients with AIRD like fear of flare of disease post-vaccination, fear of vaccine side effects and doubts over vaccine efficacy while taking immunosuppressive medications are necessary. Most patients were willing to take vaccine after counselling by a rheumatologist.
Layman Summary
COVID-19 has posed several global challenges and vaccination has helped human race tide over a lot of them. But the most vulnerable group are patients on pills that lower immunity. Most of the patients with autoimmune diseases are on such pills and have fears regarding vaccination against COVID-19. If fears regarding vaccination are left unattended, a patient with an autoimmune disease can stay unvaccinated and prone to COVID-19-related complications. The collective responsibility to allay fears regarding vaccination is on both the treating physician and the society. This study is to discuss reasons why patients with autoimmune diseases reject/fear vaccination and to address them. Most patients in our study feared that their disease might worsen after vaccination. Some patients cited vaccine-related side effects and others feared that vaccine might not work on them as they are on pills that lower immunity. We counselled patients accordingly based on reasons and noticed that most patients expressed willingness after counselling. We advocate counselling by a rheumatologist for patients with autoimmune diseases who are hesitant to vaccinate. This is because we believe that discussing complex facets of the disease and vaccination from treating rheumatologists will help them to vaccinate without fear.
Introduction
Vaccination is amongst the most significant public health achievements in modern history; however, its success has been marred to some extent by vaccine hesitancy. The Strategic Advisory Group of Experts (SAGE) on Immunisation in 2012 constituted a working group which defined vaccine hesitancy as ‘A behaviour, influenced by a number of factors including issues of confidence (do not trust vaccine or provider), complacency (do not perceive a need for a vaccine, do not value the vaccine), and convenience (access)’. 1 India’s cumulative COVID vaccination coverage has reached 2,20,64,22,209 doses as of 05/03/2023 due to an efficient vaccine public distribution system and regular awareness campaigns. 2 Vaccine hesitancy in patients with autoimmune rheumatic diseases (AIRD) and specially those on immunosuppressive medications can be disastrous from a public health perspective as they are more likely to have severe infections, transmit it to their household contacts and shed the virus for longer periods and at a higher risk of generating mutant strains compared to healthy individuals. 3 A meta-analysis of seven case-controlled studies conducted by Akiyama S et al. showed that the risk of COVID-19 in patients with AIRD was significantly higher than in control patients (OR: 2.19, 95%CI: 1.05–4.58, p = .038). 4 A single-centre study was conducted which aims to understand the possible reasons for vaccine hesitancy in patients with AIRD and the effectiveness of Specialist counselling on vaccine-hesitant patients to take the vaccine.
Method
Study Design
We conducted an observational qualitative face-to-face structured questionnaire-based cross-sectional study in which patients attending the OPD of a tertiary care hospital were asked about their vaccination status. The study was conducted during period of October 2021 to March 2022. The questionnaire initially consisted of 40 questions and was circulated among four clinician rheumatologists from the same tertiary centre. Questions that patients and clinicians found relevant and pertinent to Sage working group 2014 of ‘Model of determinants of vaccine hesitancy’ were included. The 12 questions were shortlisted by the physicians after a pilot testing involving 20 patients not from the study sample. The questionnaire was physician-administered and had closed-ended questions. The perceptions were assessed and counselled in the patients’ own language. The unvaccinated patients were asked the reason for vaccine hesitancy, and the hesitants were counselled by the treating rheumatologist. The vaccine-hesitant patients were asked at the end of counselling regarding their willingness to take the vaccine and their responses were recorded.
Sample
Convenience sampling was used, so the sample size was not calculated.
Inclusion and Exclusion Criteria
All adults (>18 years) with AIRD coming to the rheumatology OPD. Those vaccinated, recently infected (within six weeks), and non-AIRD patients were excluded.
Data Collection
The questionnaire included patients’ demographic details, diagnosis, medication details, and response to the reason for vaccine hesitancy (based on 12 questions) after obtaining consent from patients.
Statistical Analysis
Descriptive statistics were performed by calculating measures of central tendency for quantitative variables and using counts and percentages for qualitative and nominal variables. Quantitative data were expressed as proportions and qualitative data were expressed as frequencies using SPSSv23.
Results
The study included 322 patients with a mean age of 40 years (ranging from 18 to 76) and a majority of female respondents (73%). Most patients had Rheumatoid Arthritis (40%), followed by Spondyloarthritis (27%), Systemic Lupus Erythematous (13%), and other diagnoses. Almost all patients (95%) were on immunosuppressive/immunomodulatory medications. The most common reasons for vaccine hesitancy were the fear of disease flare post-vaccination (60%), fear of vaccine side effects (44.4%), and concerns about vaccine efficacy while on immunosuppressive medications (35%). Other reasons included difficulty in getting vaccinated (18%), doubts about vaccine efficacy (15%), and fear of injections (10%) (Figure 1). The majority of patients (91%) were willing to take the vaccine after specialist counselling, while only a small percentage (9%) remained hesitant even after counselling. Among the 28 patients who continued to deny the vaccine after counselling, the most common reason cited was religious or social beliefs. A breakdown of patient diagnoses is provided in Table 1.
Reasons Cited Towards COVID Vaccine Hesitancy by the Patient Population.
Characteristics of AIRD Patients Included in the Study.
Discussion
Our study found that the most common reasons for COVID vaccine hesitancy among our patient population were fear of disease flare after vaccination and doubts about vaccine efficacy. Almost all patients had multiple concerns contributing to their hesitancy, which is consistent with findings from previous studies on patients with AIRDs. For example, Shukla et al. reported poor vaccine acceptance among AIRD patients in Gujarat, India, with only 12% expressing concern about disease flare after vaccination, compared to 60% in our study. 5 The VAXICOV study similarly found that vaccine hesitancy was higher among AIRD patients than among healthcare workers, but that a large proportion (32%) of AIRD patients were uncertain about whether to get vaccinated, suggesting that collective measures could increase vaccine willingness. 6
The increased vaccine hesitancy related to disease flare may be due in part to misinformation and case reports/series of disease flare and immune adverse effects following vaccination. However, studies such as the EULAR-COVAX registry have found that although the risk of disease flare post-vaccination is up to 4%, only 1% of patients with AIRDs required intervention, and the risk of post-vaccination side effects was similar to that of the general population.7, 8 Similarly, a systematic review of 198 studies on the impact of COVID-19 in SLE patients found that vaccine-induced flares were mild and intermittent, and less than 5% required a change in medications. 9
A systematic review conducted to determine the immunogenicity of COVID-19 vaccines in immunocompromised populations showed that in patients with AIRD, the use of B cell depleting agents, methotrexate and glucocorticoids negatively impacted the immune response. 10 A study from India determined that humoral responses and attainment of neutralising activity after the BBV152 vaccine is inferior to that of the AZD1222 (ChAdOx1) vaccine in immunosuppressed patients. 11 But we are still in need of trials to ascertain ways to avoid poor immunogenicity in patients on immunosuppressants. There needs to be more clarity if additional boosters can be safe as well as efficacious in providing cell-mediated and humoral protection with regards to healthy controls. With ample data, doubts regarding vaccine effectiveness in patients on immunosuppression can be easily tackled and explained.
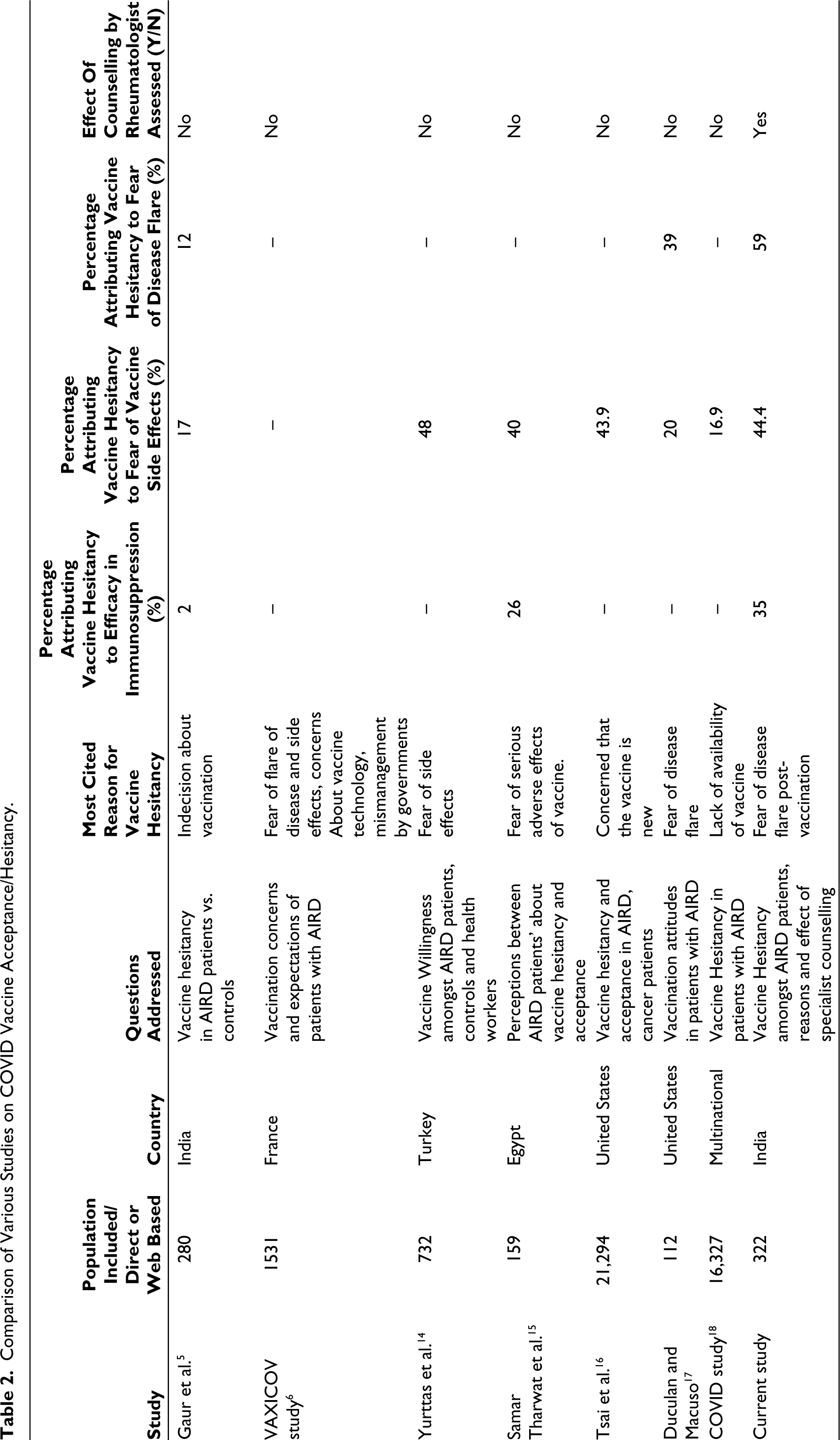
Fear related to COVID vaccine adverse effects constituted 17%–50% in various studies whereas our study showed almost half (44.4%) of patients had fear of vaccine adverse effects (Table 2). Many studies have affirmed that COVID vaccines, especially mRNA vaccines are safe in patients with AIRD.7, 12, 13 Studies which assessed vaccine acceptance and hesitancy in various sample populations have been compared in Table 2. Yurttas et al. reported that COVID vaccine acceptance could be increased if recommended by a specialist physician which was further affirmed by our study results that noticed a shift in perception after counselling by the treating physician. 14 VAXICOV STUDY categorically stated that the most trusted healthcare professional who can change COVID vaccine hesitancy is the specialist (rheumatologist) followed by the general practitioner. The fact that most patients (91%) in our study agreed to get vaccinated with just single unstructured counselling with a rheumatologist speaks volumes about the important role of specialist can play in ensuring patients with AIRD near-total vaccination coverage. Also, it demonstrated that the proportion of acceptance to COVID-19 vaccines was higher in patients who had received Influenza and Pneumococcal vaccination. A study designed to assess COVID-19 vaccine acceptance in the United States showed that patients who took influenza vaccination in the past are more likely to exhibit COVID-19 vaccine acceptance. 19 Other factors like lack of trust, religious and social barriers, and inability to get access to vaccines occupied lesser proportions. Social, religious leaders and media at large might have a role in allaying these beliefs as vaccine hesitancy was high as 9% even after physician counselling in our study, attributing the cause to religious and social beliefs.
Comparison of Various Studies on COVID Vaccine Acceptance/Hesitancy.
While the questionnaire used in the study is not a fully validated version, it is based on the SAGE working group 2014 ‘Model of determinants of vaccine hesitancy’.20 Although the study is not fully powered to assess attitude changes towards vaccination, the fact that a significant proportion (91%) of patients accepted the physician’s recommendation and expressed willingness to get vaccinated can be considered a measure of the impact of counselling by a rheumatologist. However, the study has limitations, including its cross-sectional design which makes it difficult to confirm whether patients were actually vaccinated or not, and the use of convenient sampling instead of calculating the sample size.
Conclusions
COVID vaccine hesitancy is multifactorial. Addressing reasons for vaccine hesitancy in patients with AIRD like fear of flare of disease post-vaccination, fear of vaccine side effects and doubts over vaccine efficacy while taking immunosuppressive medications are necessary. Most patients were willing to take the COVID vaccine after counselling by a rheumatologist.
Footnotes
Contribution of Authors
Conceptualisation: KC. Data curation: All authors. Formal analysis: KC; Funding acquisition: N/A. Investigation: KC, KK, PD, JD, DE, AKV. Methodology: KC; Visualisation: KC, UD. Writing-original draft: AKV, KC. Writing, Review and editing: All authors.
Data Availability Statement
Data are available upon reasonable request by any qualified researchers who engage in rigorous, independent scientific research, and will be provided following review and approval of a research proposal and Statistical Analysis Plan (SAP) and execution of a Data Sharing Agreement (DSA). All data relevant to the study are included in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval/Patient Consent
Ethical approval from institutional ethics committee was taken and informed written consent was taken from every patient prior to enrollment in the study. This study was approved by institutional ethics committee of King George's Medical University (Ref No ‑1513/Ethics/2021, dated 27‑10 2021).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Key message
COVID vaccine hesitancy is multifactorial in most. Patients fear of vaccination may affect their disease adversely, fear vaccine side effects, and doubt vaccine effectiveness while on immunosuppression. Specialist counselling improves COVID vaccination acceptance.