
Abstract
Aim:
The present study is intended to evaluate the factors influencing the diagnostic and rheumatology care referral delay in patients with spondyloarthropathy (SpA) and psoriatic arthritis (PsA) in India.
Materials and methods:
The independent prospective, multicentre, observational study collected data from 8 centres across India through the database created by the Indian Rheumatology Association (IRA). Modified Prasad scale was used for socio-economic classification based on the patient’s income. The data of PsA and SpA were analysed separately, and the causes were compared using t-test for continuous variables and chi-square and Fisher’s exact tests for categorical variables.
Results:
The mean referral delay noted for PsA and SpA subjects were 16.3±34.35 and 17.48±33.59 (IQR 24 and 34) months, respectively. Majority of the PsA patients and about 65% of SpA subjects reported a lack of awareness of the rheumatology specialty as the major reason for the delay. Another major reason was management by other specialists instead of rheumatologists (65% and 74% respectively). Approximately 8% of patients in both disease groups had no faith in modern care due to perceived elevated risk of adverse effects. SpA patients with improved socio-economic status had a higher proportion of subjects seeking specialty care. A direct association was noted between professional skill and early access to specialty care for both PsA and SpA patients.
Conclusion:
The lack of awareness of rheumatology as a specialty and patients being managed by other specialties are the two major reasons for delayed referral of SpA and PsA. Additionally, a patient’s economic and skill level can influence their ability to access specialty care.
Introduction
The disease burden of both spondyloarthropathy (SpA) and psoriatic arthritis (PsA) is substantial and extends beyond physical symptoms to include reduced mobility, impaired mental health, and overall quality of life. Spondyloarthropathy (SpA) is a commonly prevalent inflammatory rheumatic disease in India, following rheumatoid arthritis. The prevalence of HLA-B27 subtypes in the country is estimated to be approximately 6%. 1 A one-year study by Kumar et al. reported the prevalence of PsA as 8.7%. The researchers also observed differences in prevalence rates, which can be attributed to geographical and ethnic distinctions, differences in the clinical characteristics of the patients with psoriasis, and the specific diagnostic criteria employed. 2
The early diagnosis and treatment of PsA are critical for preventing irreversible joint damage and improving quality of life. 3 However, majority of the subjects experience diagnostic delays, which can lead to a delay in treatment and worsening of symptoms. PsA poses a significant challenge for diagnosis and management. Early diagnosis is critical for optimal management and prevention of associated comorbidities and long-term functional disability. 4 A delay of 6 months from the symptom onset to rheumatology care can result in peripheral joint erosions and impaired long-term physical function. 5
Defining a specific time frame for delay in diagnosing and referring patients to rheumatology care, can be challenging. Some studies have used the period between the first recognisable symptom attributable to the disease and confirmation of diagnosis by a healthcare provider as the benchmark, while others have proposed it as the time taken to reach the relevant specialty care.6,7 In some instances, patients who achieve timely diagnoses may not receive the appropriate specialty care, which can affect their health outcomes. The suggested golden window of opportunity for early arthritis is 12 weeks, with the ideal recommendation being 6 weeks.8,9 Both the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) recommendations, considering the real-world factors such as availability and referral delays, have extended the optimal time to consider it as a delay to 6 months.10,11 While ACR guidelines focus on RA alone, EULAR recommends a six-month or longer delay in other early arthritis types. Based on these facts, the present study had arbitrarily chosen 6 months as the cut-off to consider it as a delay in accessing specialty care.
Gradual increase in awareness regarding the rheumatology field has led to a rise in the number of training centres in India.
12
Apart from accessibility and availability of specialty care, there are other factors influencing the number of patients approaching specialty care. They can be broadly categorised as follows:
Patient-related factors (belief, self-care, education, socio-economic status, demographic characteristics, disease knowledge, and affordability), Primary care or referring physician-related factors (knowledge about specialty and diagnosis), and Disease-related factors (clinical presentations). The study analysed the delay in diagnosis and referral of SpA and PsA under these three broad headings. The present study findings may help in stratifying the interventions to improve early diagnosis and access to specialty care.
Material and Methods
Registry/Database Design and Study Population
The observational study was conducted across 8 centres in India by gathering the data through database created by the Indian Rheumatology Association (IRA). The centres were selected based on their geographic location and the presence of patients with 6 different autoimmune diseases, namely rheumatoid arthritis, SpA, PsA, systemic lupus erythematosus (SLE), scleroderma, and primary Sjögren’s syndrome (pSS). The current study considered data of adult patients with PsA, and SpA who met the respective classification criteria. ClASsification criteria for Psoriatic ARthritis (CASPAR criteria) were used for PsA, while Assessment of Spondylarthritis (ASAS) International Society classification criteria were used for SpA.13,14 The database was launched in April 2020 and included both newly diagnosed patients and those undergoing follow-up at the centres. Data were collected using two separate structured proformas, with the first one gathering information on common demographic and socio-economic profiles, obstetrics, functional impairment, and health-related parameters, while the second collected information on disease-specific parameters. The questions for data collection were formulated by the experts, who were part of the database deployment and had undergone a trial before being finalised. The answers were filled in by the clinical research associates (CRAs) based on the responses received from the patients. To standardise the process across all the centres, both the principal investigators (PI) and the CRAs underwent online training organised by the nodal centre. Any related queries during data collection were addressed by the PI at the nodal centre. All participating centres had obtained clearance from their institutional ethical committees (the list of which is included in the appendix), and written informed consent was obtained from all selected patients in accordance with institutional recommendations.
Sample Size Calculation for Registry
The study aimed to evaluate the clinical and laboratory profile of the AIRDS under consideration with reference to patients referred to tertiary care for Musculoskeletal symptoms. Based on the reported prevalence of the individual diseases, a minimum of 6,500 patients were estimated to be recruited for analysis. Since the study was of a cross-sectional design and patients were selected from those visiting rheumatology care, the estimated prevalence of all AIRDS in patients with musculoskeletal symptoms combined was approximated at 10%. 15 The calculated P value was .01. For a 99% confidence interval, the corresponding Z-score was 2.59, and the estimated precision (d) was 0.01. Based on these calculations, the estimated population size required for the study was 6,037. To account for potential dropouts and missing values, a buffer was added, resulting in a final estimated sample size of 6,500. 16
Data Collection and Definitions Specific to Delay
The study considered the time taken to access tertiary care from the point of first attributable symptom or sign related to the primary diagnosis to understand the factors associated with delay. A Six-months delay was considered as the cut-off for the delay in referral or reaching the tertiary centre. A tertiary rheumatology centre is defined as a specialised healthcare facility that provides highly specialised care for patients with rheumatic diseases. In cases where a patient had previously consulted a rheumatologist in a private clinic before reaching a tertiary centre, their initial visit to the rheumatologist was taken into consideration for estimating the referral delay. The patients’ first enrolment to specialty care was considered rather than the diagnostic conclusion prior to referral or in the rheumatology department.
The research team interviewed and assessed each patient to gain further insight into the factors associated with the delay. The patient-related factors considered were their belief in modern medical care, lack of knowledge regarding rheumatology specialty, socio-economic reasons (treatment affordability and considerable distance to specialty centre), and the notion that modern medical care poses higher risk for adverse events. The major referral factors considered based on the patient’s briefing are summarised below: The primary care provider either refrained from referring them to a rheumatologist or hesitated to do so. Despite the correct diagnosis, the patients were directed to various other specialties such as dermatology, nephrology and orthopaedics. The lack of awareness about the rheumatology specialty by the primary care physician, and the absence of documentation or patient awareness of the primary diagnosis were among the factors considered. Despite considering all these factors, for patients who were unable to ascertain or subject the reason, it was recorded as ‘not ascertainable’. Modified Prasad scale was used for socio-economic classification, which uses the patient’s income, education status, and profession. 17 Clinical presentation and system involvement were also considered for the analysis.
Statistical Analysis
Descriptive analysis was performed using Microsoft Excel. The data of PsA and SpA were analysed separately, and the causes were compared using t-test for continuous variables, and the chi-square test and Fisher’s exact test for categorical variables. Missing data, especially those with no discernible reasons, were excluded from the analysis presuming them to be unrelated to the anticipated cause. Subjects belonging to each disease group were divided into patients referred to rheumatology specialty within 6 months and those referred to >6 months. The analyses were carried out using VassarStats and Statistical Package for the Social Sciences (SPSS, IBM, version 29.0.0). 18
Results
Five hundred and eight PsA patients were recruited, and one was excluded due to data incomplete data. Additionally, 1,163 SpA patients were recruited and 8 were excluded because of incomplete data. Based on the inclusion and exclusion criteria, the number of study subjects considered for PsA and SpA were 507 and 1,155 respectively. Mean age of the population, gender distribution, and mean duration to avail specialty care noted for the disease groups are depicted in Table 1. The mean referral delay noted in PsA and SpA subjects were 16.3±34.35 months and 17.48± 33.59 (IQR 24 and 34) months respectively. Nearly 50% of the PsA subjects availed specialty care within 6 months. Whereas it was only 35% among SpA patients. Nearly 29% and 38% of the subjects belonging to the PsA and SpA respectively reported a delay in referral of >24 months. Majority of the PsA patients and around 65% of SpA subjects reported lack of awareness regarding rheumatology specialty as the major reason for the delay. Around 8% of the patients in both the disease groups had no faith in modern care due to the notion of elevated risk for adverse effects. Management by other specialists, instead of rheumatologists, was another major reason for the delay (65% and 74% respectively). In addition, >25% of primary care clinicians were unaware of the rheumatology specialty and nearly 47% of the PsA subjects were not correctly diagnosed by the primary care physician (Table 1).
The Demographic Distribution of PsA and Seronegative SpA and Comparison of the Causes of Delay.
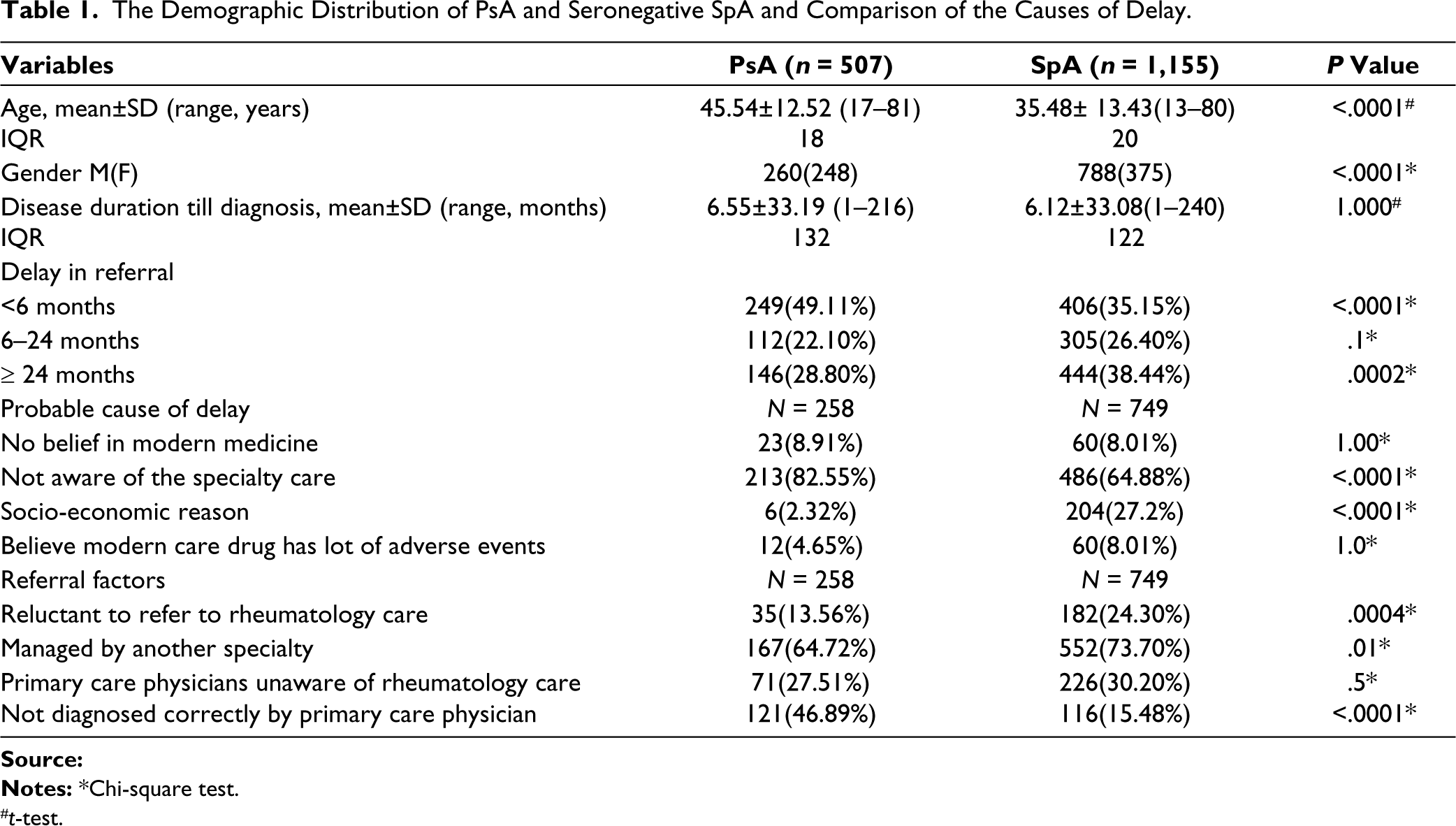
#t-test.
The comparison of causes for diagnostic delay due to clinical features showed no significant difference (details provided as supplementary file). Nearly 39% of the female SpA patients were referred to rheumatology care early as opposed to 33% of the male counterparts. Whereas no gender difference was noted for PsA. The proportion of subjects seeking specialty care was higher for SpA patients with improved socio-economic status. However, no such association was noted for PsA. In addition, a direct association was noted between professional skill and early access to specialty care for PsA and SpA patients (details provided as supplementary file).
Discussion
The current study has noted that only 35% of the SpA subjects availed specialty care within 6 months, whereas it was around 50% for PsA. Majority of the PsA patients and around 65% of SpA subjects reported lack of awareness regarding rheumatology specialty as the major reason for the delay. A 2022 UK-based literature survey conducted across two national health service (NHS) rheumatology services has found an average delay of 8.7 years between the onset of symptoms and a formal diagnosis. The study found that lack of awareness and recognition of axial SpA among healthcare professionals is one of the contributing factors to this diagnostic delay. 19 An international collaboration study by Ono et al. has reported that the lack of collaboration between specialists like gastroenterologists is the primary reason for delay in diagnosis noted in SpA patients with inflammatory bowel disease. 20
As per the 2014 update of the Canadian treatment recommendations for the management of SpA, subjects with elevated risk of peripheral SpA, including patients with PsA, should be examined by a rheumatologist within 6 weeks of referral. 21 A 2022 study by Park et al. noted that the primary reason for the delay in such patients was the limited availability of appointments in the PsA clinic. The researchers noted that improving access to rheumatologists can play a crucial role in providing timely and effective care to patients with PsA. 22
A cross-sectional, hospital-based study by Karoli et al. highlighted the importance of early and accurate diagnosis of ankylosing spondylitis to prevent irreversible structural damage and deterioration of quality of life. The researchers noted that majority of the patients exhibited advanced disease, probably due to delay in diagnosis. 23 Haroon et al. reported one year as the median duration between disease onset and the first rheumatologic assessment. The experts also observed that even 6 months delay from the onset of symptoms to the first visit to a rheumatologist can contribute to the development of peripheral joint erosions, sacroiliitis, and impaired long-term physical function. 5
Several factors including patients’ perceptions and concerns influence treatment adherence. The ALIGN study, which explored the association of patient factors with adherence to medications in a population with immune-mediated inflammatory diseases, including rheumatoid arthritis, PsA, and ankylosing spondylitis, showed a strong correlation between treatment beliefs and adherence to systemic medications. TNF inhibitors, as mono or combination therapy, had the highest adherence rates among the treatment options explored. 24
The study has noted a direct association between the proportion of subjects with SpA seeking specialty care and improved socio-economic status. Moreover, the study has noted a direct association between professional skills and early access to specialty care for both study groups. A qualitative study by Arpey et al. has noted that there is substantial literature evidence to validate that socio-economic status influences an individual’s health outcomes and the healthcare they receive. Subjects with low socio-economic status tend to have worse health outcomes, reduced life expectancy, and increased risk for chronic conditions. Moreover, they have limited access to diagnostic tests and medications due to increased cost and accessibility constraints. 25 Contrary to the current study finding, a nested case-control study by Joud et al. concluded that there is no association between socio-economic status and the risk of being diagnosed with SpA. 26
Studies have reported the existence of gender differences in the diagnosis and management of SpA. Chimenti et al. have observed longer diagnostic delays among female patients with axial SpA as opposed to male subjects and suggested distinct clinical presentations as the probable reason for this difference across genders. 27 In contrast, the current study has noted that a higher percentage of female SpA patients were referred to rheumatology care at an early stage compared to male SpA patients.
The current study has notable strengths such as the collection of data from multiple centres, larger sample size, and the inclusion of participants from diverse academic and private settings, thus providing representation for individuals from various socio-economic backgrounds. However, limitations of the study are apparent, including the non-uniformity in the number of patients recruited from different centres, the study cohort not being representative of the general population of India, and the limited generalisability of the study findings. Furthermore, potential bias may have arisen due to researchers’ discretion in gathering information on reasons for referral delays through the recall method. This bias has been reduced by providing sufficient training on data collection techniques.
Increasing the awareness of both the general public and primary care providers about the latest developments in the specialty care of PsA and SpA is crucial to improve early referral rates. The awareness should also focus on strategies for effective management, the benefits of early identification, and the advantages of early intervention. Additionally, it is important to address any misconceptions that patients may have about these conditions to promote early diagnosis and intervention.
Conclusion
The two major reasons for delayed referral of SpA and PsA are the lack of awareness of rheumatology as a specialty and the patients being managed by other specialties. Additionally, a patient’s economic and skill level can influence their ability to access specialty care. Appropriate interventions, at the professionals and the public front, are recommended to improve early referrals and to reduce the overall disease burden.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Author Contributions
All the authors have contributed equally to the conceptualisation, data capturing and development of the content.
Acknowledgements
Dr Debashish Dhanda and Dr Aman Sharma for their participation in administrative roles in the IRA database. The authors acknowledge the help of Research Assist (
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable
Funding
Educational and research grants from Novartis India.