
Abstract
This project aimed to explore the perspectives of entertainment industry and health communication practitioners in the United States on creating health storylines in entertainment programming. These dual perspectives are usually not studied in tandem but together offer insights into the creation of impactful health-related narratives. In-depth interviews were conducted with entertainment industry and health professionals (N = 6) who are experienced in creating health storylines. Questions aimed to illuminate how practitioners define ‘success’ of a health storyline, what they perceive as key elements for impactful health storylines, how key story elements are created and the nature of collaboration between the entertainment industry and public health. Grounded theory analysis identified three core themes for the successful combination of narrative entertainment and health: choosing teams with complementary strengths (e.g., leveraging professional collaboration and trust), knowing your audience (e.g., conducting formative research to understand who the story is intended for and why) and integrating health content in authentic ways (e.g., telling dramatic stories with universal themes, without creating from the intent of relaying health information). Best-practice guidelines for narrative entertainment to communicate about health, informed by the core themes and persuasion theory, are offered for narrative development, pre-production, content creation and dissemination.
Keywords
Introduction
The potential for narrative entertainment to educate and influence viewers presents health communicators with opportunity and challenge. Academic research on health-related narrative communication (e.g., De Graaf et al., 2016; Green & Fitzgerald, 2017; Kreuter et al., 2007) and entertainment-education (EE; e.g., Igartua & Casanova, 2016; Moyer-Gusé, 2008; Quintero Johnson et al., 2013; Singhal et al., 2006) have identified attributes and mechanisms of narratives that may lead to health-supporting outcomes. Although these academic perspectives are valuable, the perspective of entertainment industry and health-communication practitioners on creating such narratives has yet to be fully explored. For example, it remains unclear how practitioners define a successful health storyline, and what they perceive to be its key elements and how best to create those elements. A lack of clarity about how health communication, entertainment and public health professionals may, or may not, align in their approaches, emphases and even perhaps terminology around storytelling in health contexts impedes the establishment of best practices for narrative entertainment to communicate about health. On the other hand, integrating practitioner expertise with relevant theory would benefit and inform the process of health narrative creation, facilitate the establishment of best practices and enable more effective collaborations among health communication, public health, entertainment and production stakeholders.
To help fill these gaps, this project turned to the entertainment industry and its collaborators as a resource for health-pertaining story expertise. Writers, producers and public health professionals involved in the creation of health-related narratives were interviewed for guidance on how to create successful narratives that integrate health and storylines. The goal of this project was to illuminate these practices and to show how they connect with theory-based models of narrative effects. Thus, for health communication practitioners, public health practitioners, researchers and other professionals working with narrative entertainment to communicate about health, this project provides guidance that is informed by both theory and practice.
Literature Review
Entertainment-Education
Entertainment-education (EE) has largely been defined as the purposeful combination of entertainment and education to increase knowledge, influence attitudes and change behaviour along the prosocial spectrum (Singhal & Rogers, 2012). A classic example is Sesame Street, which began airing in 1969 with the goal to help preschool children become ready for school. The television show is associated with increased literacy, numeracy and health knowledge among children around the world (Kwauk et al., 2016). Although this example illustrates a program created specifically for education, researchers have also studied the impact of entertainment programming that is not specifically created to educate but may nonetheless have an educational impact. EE is predominantly this type in the United States, with existing entertainment programs embedded with educational messages rather than a program created for that educational purpose (Sood et al., 2017). For example, the primetime drama series Desperate Housewives included a cancer storyline, and the storyline changed viewer attitudes, knowledge and behaviour regarding lymphoma (Murphy et al., 2011). Both types of efforts—creating entertainment programs with the primary purpose to educate and embedding educational information into existing entertainment programs—are included in this project’s definition of EE. However, in this study, we focus primarily on the latter type and other products created by the entertainment industry in the United States, particularly the industry based in Hollywood.
Effective EE of this type requires skilled managers, producers, directors and writers to create and convey health content in an entertaining manner. No single process exists for getting health narratives into a script and onto the screen. Health storylines come from a variety of sources, including producers or screenwriters who have a personal interest or connection; staff or expert consultants who review scripts and may suggest ideas for more realistic stories or characters; and special interest groups or health agencies that engage in outreach efforts, perhaps via Hollywood-based advocacy organisations that liaise with the entertainment community (The Henry J. Kaiser Family Foundation, 2004).
In collaborations between the Hollywood-based entertainment industry and public health agencies, the public-health focus has been on assisting with portrayals that are accurate and that do not perpetuate health myths. These efforts are supported by organisations such as Hollywood, Health & Society (n.d.; HH&S) at the University of Southern California’s Annenberg Norman Lear Center, which aims to help entertainment professionals to include accurate storylines regarding health issues. For example, HH&S worked with the creators of Desperate Housewives to ensure the accuracy of the cancer storyline mentioned above. However, although ensuring accuracy is an important dimension of a health-related narrative, it is only one aspect of the narrative. More broadly construed, narratives are compelling because they elicit emotion and create transporting experiences, as will be explained below. Further, narratives may provide contextual cues that may frame health issues in certain lights, such as the extent to which health conditions are stigmatised. Thus, for those who are interested in the process of creating health narratives, a key question is the extent to which these other dimensions of narratives are informed by public health and entertainment perspectives, and ideally how to ensure both commercial and public health ‘success’.
Existing guidance on these issues is limited. EE gained its traction as a public health tool in developing countries, and Writing and Producing for Television and Film: Communication for Behavior Change (De Fossard & Riber, 2005) is a guide for implementing EE programs of this kind. As explained in this book, the program manager and filmmaker ideally collaborate to bridge the entertainment team (writer, actor and director) and the educational message design team. Together, they focus on the message, intended audience, plot, characters and visual representation. The aim is for impactful messages to be delivered in an engaging way that is appropriate for the audience. The guide encourages using the smallest message dose possible to promote behaviour change and using characters who feel like real people rather than mouthpieces for the message to increase behaviour adoption. However, given EE’s diversity in focus, content, form, funding and path to production (Walton-Wetzel, 2018), the extent to which the guidance is generalisable to other kinds of EE programs or other media remains unclear.
In addition to this guide, resources are available that support the accuracy of health depiction within a narrative. As examples, the US Centers for Disease Control and Prevention (2020) offers a resource webpage for entertainment writers and producers that includes tip sheets by health topic. Moreover, as already mentioned, programs such as HH&S provide free consultations, briefings and other resources such as tip sheets for entertainment industry professionals to promote the accurate depiction of public health and climate change topics in film and television shows. These health topic resources, while valuable, do not offer practical guidance on the creation of the narrative itself.
Whereas the previous resources originate from the public health perspective, there is also guidance on the crafting of effective stories from the entertainment perspective. For example, Story: Substance, Structure, Style, and the Principles of Screenwriting (McKee, 1997) is an instructional book that is widely used by writers in the entertainment industry. Featured concepts include realism (balancing between pure fact and pure imagination to convey truth), structure (creating a story out of the choices or actions that characters make under pressure) and character identification (sympathy and empathy when a character is revealed or changed by how they choose to act under pressure). Specifically, writers should convey what a character desires and why, and stories should demonstrate ideas about life. Screenwriters are often called upon to craft health storylines, as suggested by research showing that more than half of the top-rated, primetime, English-speaking, scripted shows had health storylines (Rosenthal et al., 2014). However, although McKee’s (1997) guide provides insight into the writing process and how to start writing stories for the screen, its scope does not include health storylines and the unique challenges involved.
Few studies have looked at the on-the-ground process of collaborating between those creating narratives for commercial success and those who are interested in advocating for health. Some studies have focused on the different emphases brought to the table by health communication professionals and media production professionals when collaborating on EE. For example, health communicators think of ‘target groups’, ‘behaviour change’, ‘story-telling for social change’ and a message-centred approach of health education, whereas media production professionals think more about ‘viewers’, ‘viewers’ satisfaction’ and audience-centred entertainment; reciprocal working relationships can be developed that overcome some of the differences in habitus between these professionals (Bouman, 2002; McKee, 2017; Walton-Wetzel, 2018). The current study further explores collaborations from the distinct perspective of health communication, public health, entertainment and production stakeholders in the United States.
Narrative Persuasion
Researchers have argued that human brains are hard-wired to think in terms of stories (Fisher, 1987; Schank & Abelson, 1995). Narrative communication, harnessing this phenomenon, is ‘a representation of connected events and characters that has an identifiable structure, is bounded in space and time and contains implicit or explicit messages about the topic being addressed’ (Kreuter et al., 2007, p. 222). Despite lacking a universal definition in the literature (Hinyard & Kreuter, 2007), ‘narrative’ is often synonymous with ‘story’ (Green & Fitzgerald, 2017; Kreuter et al., 2007). Herein, we use the terms interchangeably. Narrative persuasion, of which EE is an example, is ‘any influence on beliefs, attitudes or actions brought about by a narrative message through processes associated with narrative comprehension or engagement’ (Bilandzic & Busselle, 2012, p. 201). It capitalises on the likelihood that one will accept information as truth unless motivated to look critically, a human tendency that research shows is pervasive (Gilbert, 1991).
Exposure to narratives is positively associated with story-consistent beliefs, attitudes, intentions and behaviours across narrative mediums (Braddock & Dillard, 2016); influences health beliefs and behaviours on various topics, including organ donation, cancer screening and unplanned teen pregnancy (Morgan et al., 2009; Moyer-Gusé & Nabi, 2010; Murphy et al., 2011); and provides ‘stimulus and context’ for discussing sensitive, stigmatised health topics (Papa & Singhal, 2009). A story’s formulation may also lead, however, to unintended consequences, such as when persuasive subtext in stories with explicit agenda backfires and creates a negative evaluation of the attempt (Asbeek Brusse et al., 2015) or when health information not well integrated with the storyline is poorly recalled (Quintero Johnson et al., 2013). Embedding potentially resistance-generating health message in a compelling story may overcome viewer resistance, and Green (2013) urges cooperation of creators of entertainment media to embed health persuasion content without reducing narrative quality.
Modelling How EE Works
The entertainment overcoming resistance model (EORM; Moyer-Gusé, 2008) conceptually explains narrative influence; integrates contributions from transportation theory (Green & Brock, 2000), narrative engagement model (Busselle & Bilandzic, 2008), extended elaboration likelihood model (E-ELM; Slater & Rouner, 2002) and social cognitive theory (Bandura, 2002), among others; and suggests eight features leading to story-consistent attitudes and beliefs: transportation, identification, parasocial interaction, liking, perceived similarity, the perceived similarity with an efficacious character, narrative structure and enjoyment. Transportation (sometimes referred to as engagement or absorption) and identification are distinct processes (Tal-Or & Cohen, 2010) that have been identified via meta-analysis (Tukachinsky & Tokunaga, 2013) as most central to narrative persuasion; we further focus on them and other character-relevant constructs.
Transportation
In transportation theory, transportation reflects a holistic state of being in the narrative world with ‘an integrative melding of attention, imagery, and feelings’ (Green & Brock, 2000, p. 701). Associated persuasive mechanisms include reduced counterarguing, heightened connections with characters, heightened perceptions of realism, more emotional engagement and more story-relevant mental imagery. Counterarguing, also emphasised in E-ELM and EORM, involves generating rebuttals to presented information via critical thought that transportation disrupts. The idea is that viewers who are highly transported will be less likely to generate arguments against an embedded persuasive message. Similarly, high levels of emotional engagement with characters may encourage audience members to be less critical of characters’ actions, which can be helpful if viewers are initially resistant or dismissive towards actions modelled by the character. Overall, higher transportation supports positive evaluations of story protagonists, more story-consistent beliefs even with fictional stories, and effect on story-related beliefs (Green, 2004; Green & Brock, 2000); predicts increased knowledge and behavioural intent, as demonstrated for cervical cancer screening (Murphy et al., 2013); is connected to media enjoyment, perceived realism or story plausibility; and if disrupted, may weaken persuasion and narrative experience (Green et al., 2004).
Identification
Cohen (2001) defines identification as ‘a process that consists of increasing loss of self-awareness and its temporary replacement with heightened emotional and cognitive connections with a character’ (p. 251). Cohen (2006) further conceptualises identification as including both affective and cognitive components, wherein empathy for the character, understanding their goals and motives and taking their perspective differ from aspects that appraise the character in terms of liking or similarity. Identification is described as emotional reactions or connections with characters in transportation theory and as vicarious involvement or perceived connection in E-ELM. Emotional engagement (feeling emotions in relation to characters) highly correlates with attitude and identification in the narrative engagement model (Busselle & Bilandzic, 2009). Busselle and Bilandzic (2008) conceptualise identification as perspective-taking and purport that functional overlap exists with transportation.
Other Character-relevant Constructs
Differing from character perspective-taking, the constructs of liking and perceived similarity, or homophily, occur from the viewer’s perspective. Liking a character may lead to a parasocial relationship, or seeing the character as a friend. Perceived similarity involves cognitively noting one’s commonalities with a character, and people often like characters perceived as similar (Moyer-Gusé, 2008). Thus, a viewer can feel emotions like sympathy for a character while not sharing the character’s emotions (Busselle & Bilandzic, 2009).
Per social cognitive theory (Bandura, 2002), behaviours are learned by observing and imitating the behaviour of role models. Such social modelling may involve aspects of identification and character liking. Through vicariously experiencing attitudes and behaviours of characters, plus observing the consequences of characters’ actions, viewers learn of possible positive and negative reinforcements that guide their own future behaviour (Bandura, 2001). Epilogues given by favourable characters to summarise health messages—a staple of traditional EE—influence attitudes without producing counterarguing (Moyer-Gusé et al., 2012).
Research Questions
Despite the presented theory, research and existing guides for narratives, the perspectives of practitioners who have created successful health-related narratives—entertainment industry professionals and their collaborators—have not yet been fully explored. This expertise has the potential to illuminate the process of health narrative creation and help inform best practices of effective storytelling in health contexts. Understanding these perspectives should also enhance collaboration with public health professionals.
Thus, this project reached out to the entertainment industry and public health professionals. We posed several research questions to address:
How do practitioners define ‘success’ of a health storyline? What do they perceive as key elements for impactful health storylines? How are those key elements created? How do these findings relate to theory and existing resource texts?
To explore these areas, in-depth interviews were conducted, with discussions guided by the questions above. The results were analysed using grounded theory analysis (Glaser & Strauss, 1967), which would allow a ‘story’ to emerge that is based in data and which may or may not move beyond the parameters of the questions asked.
Methods
Participants
Participants (n = 6) were made up of the entertainment industry and public health professionals with experience in creating successful health-related storylines (see Table 1). Recruitment attempts within Hollywood included emails to entertainment industry organisations and snowball sampling. Recruitment efforts also included colleague referral and locating emails via the contact page of relevant organisations’ websites. We recognise the need for an adequate sample size to achieve saturation (i.e., the point at which the addition of more participants would not yield additional conclusions), per Glaser and Strauss (1967) and others. At the same time, there were many challenges to recruiting this hard-to-reach population (addressed in the limitations section). While the sample size may be small by some standards, it falls within the range of 5–25 participants as recommended by Creswell (1998) for qualitative inquiry. Further, a study of data saturation in field interviews by Guest et al. (2006) showed that saturation occurred within 12 interviews, with meta-themes present within six. In the present study, the sample of six yielded substantive themes that we offer as a starting point for further research.
Study Participants
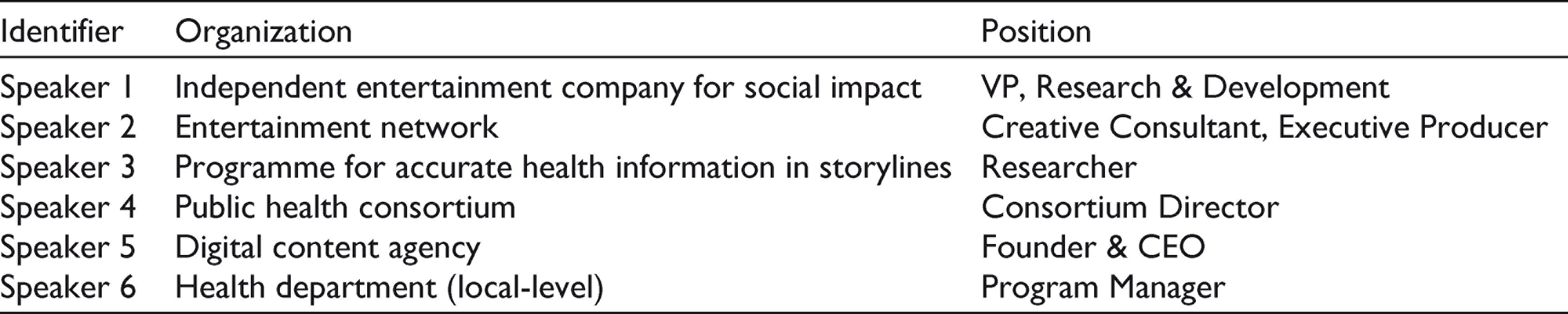
In this sample, positions varied but all participants worked within collaborative teams to develop health-related storylines for the screen. These audio-visual stories include a Hulu TV show, primetime drama episodes, mockumentary web series and web series with paired public service announcements (PSAs). Some of these works have earned awards in the health sector, as well as Emmy nominations. To protect the confidentiality, the names of specific shows and other potentially identifying information are not reported.
Data Collection
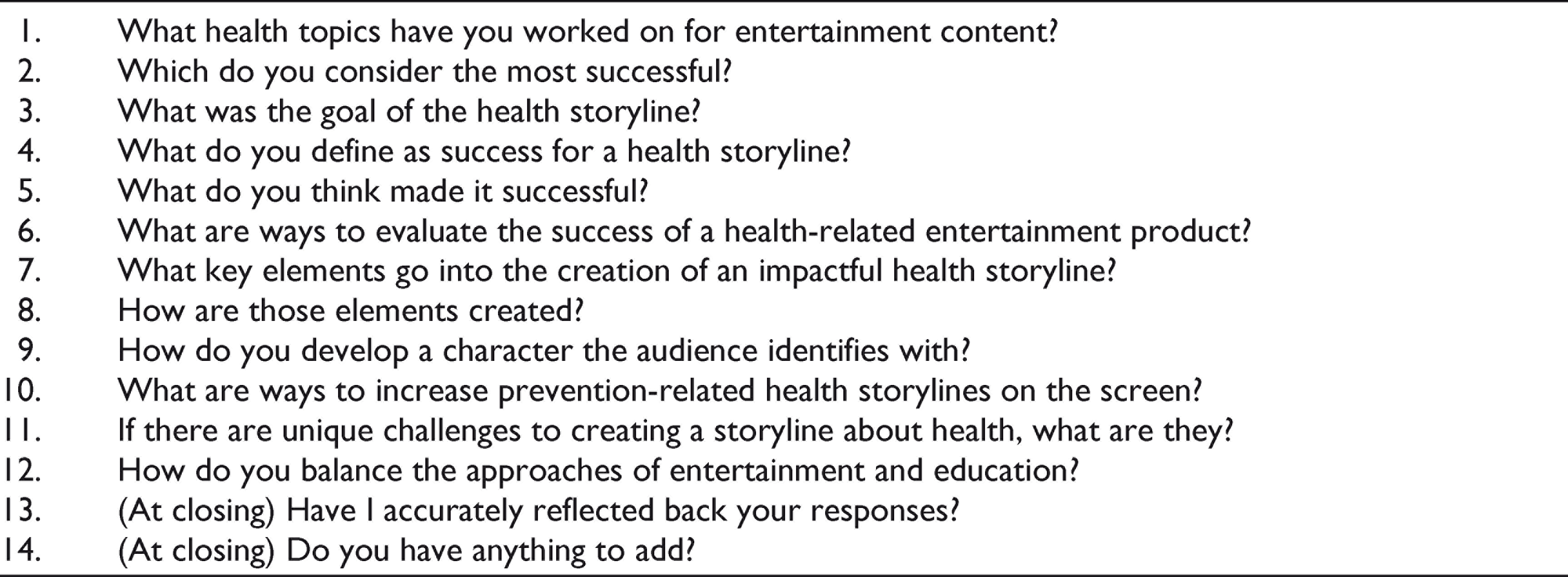
Semi-structured in-depth telephone interviews were conducted by the first author over February and March of 2019. The interviews were audio-recorded with participant permission. The average duration of a call was 40 min, with a range from 30 to 53 min. Participants were asked open-ended questions about the experience, approach and process for creating successful narratives that integrate health messages and storylines. Informed by both narrative persuasion theory and practical considerations of multidisciplinary collaboration, the questions were designed to solicit and explore responses regarding the goals, success and key elements of health storylines the participants had created (see Table 2). The Institutional Review Board at the university with which the authors are affiliated reviewed study procedures and determined the project to be exempt from further review. As a key feature of semi-structured qualitative interviews, follow-up questions were asked based on the responses of participants (Harrell & Bradley, 2009). There was evidence of response saturation emerging, in that later interviews yielded perspectives similar to those given in previous interviews, supporting meta-themes (Guest et al., 2006). Written notes were taken during the interviews and then the audio recordings were transcribed.
Per-protocol, Open-ended Interview Questions
Analysis
Grounded theory (Glaser & Strauss, 1967) was used to analyse interview transcripts. Grounded theory analysis is based on the constant comparative method and consists of a line-by-line review of content, with the categorisation of content into open, axial and selective codes. These codes illuminate concepts and themes, providing the basis of the data’s meaning. In open coding, initial concepts were identified that directly and descriptively captured the content of the data. Then in axial coding, concepts were grouped into categories. The nuances among concepts within a category were captured using subcategories. This deeper analysis revealed relationships among open codes, creating a fuller picture of the phenomenon. Finally, selective coding determined a core category to encompass the axial codes. The emergent theory was validated by the relationships among core category axial codes related to strategy and process.
The first author conducted all interviews and analysis. To comply with the grounded theory approach, assumptions were deconstructed and discussed with an additional researcher to prevent such biases.
Results
We report the following three axial themes that emerged from grounded theory analysis, as well as the overarching theme encompassing them.
Choosing Teams with Complementary Strengths
Two sub-themes composed this category: the importance of collaboration and trust.
Each participant strongly emphasised the importance of collaboration in creating a quality narrative involving health. Telling a story about health requires information about health, but it also involves writing a story, producing it and depicting people impacted by the health topic. Speaker 1 summarised the needed types of team members:
I think that it definitely involves a partnership with people who are really good at telling stories, producing stories, making the stories look good and all of that, in conjunction with the people who really understand the issues and are close to the issues, in conjunction with people whose voices you are wishing to uplift and making sure that they’re at the table as well, and having them as part of the process.
Collaboration likewise encompassed health expert consulting for writers and producers to include information that is accurate in the existing entertainment series (Speaker 3). As well, topic-relevant health organisations and patient advocacy groups may have existing materials or initiatives to combine efforts and increase reach (Speaker 2).
In combining teams representing these different perspectives, it becomes important to acknowledge the limitations of one’s expertise and to trust the perspectives of teammates. For example, responses suggest that health professionals are able to identify successful storytelling, but possess a different professional skillset and perspective from storytellers. Whereas public health professionals are experts in public health, storytellers are experts in storytelling who ‘work from a more artistic sort of approach’ (Speaker 3). Therefore, it is important to have both on a team. However, in order to have teams with complementary strengths, members on both sides have to learn to defer to others to build up trust among the different modalities. This may be easier for some groups than others. For example, from Speaker 4’s perspective, it may be harder for public health professionals to defer regarding storytelling than for content creators to defer regarding public health issues.
You’ve got to trust that the directors and the writers know how to tell really good stories, and they do. And they’ve got to, on the other hand, obviously they’re gonna … they defer very easily on the health content.
Knowing Your Audience
A major theme that emerged was the need to gather information to inform content, especially regarding who the story is intended for and why. To make informed decisions regarding these areas, there are many resources that participants reported utilising. These include team discussions, ‘needs assessments that have been done from preeminent organizations’ (Speaker 5), and focus groups with the target audience. First, the target audience needs to be identified. Audiences range from broad to niche, with varying levels of specificity in between that best serves the project’s goal. Speaker 2 addressed why the decision can be deceptively simple:
You know, the easy answer is the broadest group of people possible, but then as you carve a story into characters then you have to make sure you have characters who will speak to each of those different potential factions of the audience in some way so people can connect to it.
The full answer to the question of identifying the ‘who’ is beyond just a determination of demographic, and also requires a thorough profile to understand the culture, current situation and needs related to health topics and beyond. Such a profile, with its associated research and inquiry, might consider, for example, societal, community or personal attitudes and beliefs regarding existing or needed health services; sensitivities, roadblocks or stigma associated with a health topic; or temporal urgency of a health concern. As Speaker 6 put it, ‘We wanted to, as much as we can, meet them where they are’.
In line with knowing the audience, the majority of speakers explained that there are format options that may better serve the target audience, such as ‘episodic’ or ‘serialised’ (Speaker 5). Episodic provides a complete story arc in one episode of viewing, whereas serialised expands the arc to cover multiple episodes. The context in which the audience will view the content needs to be considered to inform a usable narrative structure that coincides with the audience’s needs. Speaker 5 elaborated:
People watch these in their homes, but we also get a lot of feedback that people are watching them in clinics. ‘Cause clinic days, you can be sitting around for hours. From doctor to doctor and it is easier to chunk off eight minutes at a time than it is to ride a 60-minute wave across a number of episodes.
Integrating Health Content in an Authentic Way
A key insight that emerged is that consideration of the story merely as a means to relay health information detracts from the effectiveness of the story itself. Participants agreed that creating from this intention does not produce an authentic or engaging story because the audience picks up on the agenda and is turned off. As Speaker 4 states, ‘Tell stories, don’t give opinions… have a dramatic arc that makes you want to go from minute one to minute 30’.
Participants emphasised the necessity of conflict and drama within a story to capture the audience’s interest. An example of conflict is a character facing adversity, and the viewer watches to see how that character will overcome it. A key point, however, is that although the audience should have a clear understanding of what outcome they want to happen, the journey should not be straightforward. As Speakers 1 and 2 respectively said, ‘show both sides and let people come to their own reactions about it’, because a unidimensional storyline seems preachy and ‘people will disengage and say it’s not feeling honest’.
Variants of representing ‘real’ and ‘experience’ were featured strongly throughout the interviews, with the story’s plot pulling from real-life experience. This, however, does not mean ‘documentary’. Speaker 5 clarified:
We’re constantly getting people’s actual stories. So those heavily inform the way that we craft. But we also don’t stay beholden to ‘it must have been reported as having happened or else we can’t do it’, which I think can be a false sense of authenticity. You’re allowed to use your creative imagination… so long as we don’t stray outside the realms of what is possible.
Telling a dramatic story involves sharing the different layers of context in addition to the viewpoints. Stories portray not just an individual, but wider society. Providing contextual depth to a character’s situation makes both the story more holistic and the character fleshed out. It also may help the audience better understand and empathise with the character, ideally contributing to the influence of social norms and a decrease in stigma (Speakers 1 and 4). Speaker 1 further explained:
So many times, people go in with the individual lens of an issue and how it affects that person, but when you are able to show that it goes deeper than that, that there are systemic reasons behind these issues, or how it affects the people around them, or their communities, it’s much more impactful.
Another important element the participants discussed was employing universal themes. In this way, writers ‘let the specific tell the universal’ (Speaker 4). Universal themes were described as allowing the audience to personally relate to the onscreen situations, regardless of the plot intricacies. Speaker 1 again explained, ‘We can all identify with a feeling of loss, or love, or family, or feeling like the underdog and having to overcome that’.
Whereas the previous points relate to integrating health information within a narrative, participants also offered suggestions for providing specific health information in ways that are outside the bounds of the typical storyline. For example, Speaker 2 encouraged placing resources for the ‘conclusive facts and statements’ at the end of the story, via a phone number or website. Another suggestion was to supplement the story with PSAs (Speaker 4). As participants acknowledged, public health professionals find it difficult to resist the urge to include large amounts of information in the story because their go-to intention is to inform. However, entertainment professionals provide necessary, and ultimately appreciated, push-back to balance what the story should contain to remain informatively useful without taking the audience out of the storyline. As Speaker 4 described:
We were able to use those PSAs as really the primary vehicle where all the really heavy information gets out there and then the dramatic series brings out the issues but doesn’t load them with information.
Overarching Theme: Transporting Audiences to Better Health
Emerging from grounded theory analysis, the phenomenon at the core of interview responses is the successful combination of narrative entertainment and health, which spurs audiences on a process of seeking better health. This phenomenon begins with ‘holistically telling authentic and accurate stories’ (Speaker 3), which represents both the entertainment and public health perspectives and involves mutual deference to teammates’ greater expertise in given areas. Successfully combined stories then bring the audience on a journey, with resulting outcomes of audiences talking or posting about, being aware of, understanding, and/or seeking additional information on the health topic. The narrative may also serve as a ‘springboard’ (Speaker 5) for guided discussions and skill-building activities. These outcomes, especially reactions on social media and interaction with resources for additional information, provide useful feedback to support or reassess decisions and content for future efforts.
Discussion
We began with the aim of illuminating the perspectives of entertainment industry and health communication practitioners involved in the creation of health narratives. Given that narratives are a powerful way to educate about health, it is important to understand how successful ones are created so that the process may be followed by others. Although there are organisations, such as HH&S, which serve as health information consultants for entertainment programs in the United States, the primary purpose of those organisations is simply to ensure the inclusion of accurate information. And although there is extensive academic research on narrative persuasion and EE, the practical expertise and perspective of successful storytellers for health had been underutilised. Thus, the current project interviewed entertainment industry and public health professionals with experience creating health-related storylines for the screen to bring those under-examined perspectives to light: in particular, to understand from their perspectives what success looked like, the key elements necessary for it and how to create those elements. Responses were analysed using grounded theory, which led to a framework for impactful health-related narratives.
A key finding is that practitioners define ‘success’ of a health storyline as organically, holistically integrating health content to tell authentic and accurate stories. This success is evident through audience response, such as discussions in person and online, increased awareness, understanding and motivation to learn more about the health topic. The parameters of this success are also dependent on the initial goal. The key elements for impactful health storylines fall within two areas: knowing your audience and integrating health content. To know your audience requires formative research with and about the target audience. Integration is achieved via elements of (a) conflict among various viewpoints, (b) social contexts around the health topic, (c) universal themes, (d) limiting health information only to that organic to the storyline and (e) supplementing with additional health information through resources and/or materials linked to the narrative. Finally, in order to accomplish these tasks, the skills and expertise of both storytellers (writers, producers, directors, cinematographers) and health professionals (subject matter experts, health organisations) are required, with the team decisions informed by ongoing input, feedback from the intended audience and formative public health research and current initiatives.
Given that the main findings of this study were about process, it is worthwhile to consider them in light of the EE guide reviewed earlier (Writing and Producing for Television and Film: Communication for Behavior Change; De Fossard & Riber, 2005). Our findings are similar to those offered by De Fossard and Riber in that both sets emphasise collaborating, knowing your audience through formative and process evaluation, and integrating health information in ways that will maintain the authenticity of the story. However, the vocabulary for discussing EE is different. In the De Fossard and Riber (2005) guide, as well as in other academic works, EE is described using words like ‘embedded’, ‘health message’ and ‘change behaviour’. From the perspective of our participants, this language and in turn the implied agenda behind such words would not be viable in practice as indicated by the fact that none of the respondents referred to their work as EE or spoke about persuading the viewer. This finding is consistent with the colloquial preference for ‘social impact’, reported by Walton-Wetzel (2018). According to participants in the current study, health information is in the storyline to raise awareness and educate as opposed to persuade. Approaching content with a holistic perspective necessarily refocuses emphasis to be on the narrative as a whole rather than two independent agendas of entertainment and health. The general consensus is that this approach would create stories of more interest and impact on viewers. The approach is also consistent with the phenomenon of psychological reactance (Brehm & Brehm, 1981), wherein people resist being told what to do and dislike having their autonomy taken away when they are aware of being persuaded.
Respondents described audiences going on a journey and relating to characters and their stories. Reflecting back on existing narrative and EE theory, these intentions for the audience seem analogous to the academic constructs of identification and transportation. Responses focused on the front-end creation from the entertainment industry and public health professional perspective more so than that of the audience. The EORM (Moyer-Gusé, 2008) presented eight features that facilitate impact on viewers: transportation, identification, parasocial interaction, liking, perceived similarity, the perceived similarity with an efficacious character, narrative structure and enjoyment. In addition to identification and transportation, respondents addressed narrative structure and enjoyment, though dimensions of character-audience response related to identification were not consistently extrapolated beyond character. With some overlap to the EORM, attributes of quality narrative such as sequence, character, structure, bounded in space/time and production values (Kreuter et al., 2007) were likewise identified as necessary elements by interviewees.
Because this research focused primarily on the process of creating EE, it was not the aim to contribute directly to narrative persuasion theory. However, theory undergirded the interview questions, which aimed to explore key elements for effective (‘successful’) storytelling, as perceived by practitioners. The study results thus both support the application of narrative theory and illuminate key mechanisms and constructs that were elicited. While practitioners place a high priority on authenticity and accuracy, they perceive that narratives are most compelling when they elicit emotion and create transporting experiences. As discussed above, practitioners prioritise taking the audience on a journey and engaging them in a relationship with the characters and their stories. Hence, the key constructs of transportation and identification, which have been identified within the theoretical framework as most central to narrative persuasion (Tukachinsky & Tokunaga, 2013), are valued and executed in practice.
Although social media was not addressed by participants beyond its use as a gage of audience reception, it is important to consider how social media may influence the reach and impact of health narratives. People in North America use social media for about two hours each day, in part motivated by entertainment (Bayindir & Kavanagh, 2018). Among adults in the United States, 69% are on Facebook and 75% of young people are on Instagram (Perrin & Anderson, 2019). We posit that social media would help creators of health-related narratives to connect with audiences (‘meet them where they are’; Speaker 5) and would lend itself particularly well for participatory approaches in EE (e.g., serve as further discussion ‘springboard’; Speaker 5). Riley et al. (2017) assert that such audience participation can be used in formative research to determine norms and potential solutions, and as a form of social listening to evaluate the impact of programs.
In addition to enhancing evaluation, social media could also extend the influence of EE programs by engaging audiences as co-creators of content or even ‘ambassadors’ of a show. For example, research has shown that television viewers interact with content posted about television shows on social media as well as communicate about the shows to other viewers (Min et al., 2015). Being a participatory method, social media could empower respondents, promote collaboration among stakeholders and facilitate the development of culturally sensitive EE interventions (Riley et al., 2017). Engagement with the audience through conversation, then, might serve as the key to promotional efforts by entertainment program producers (Lu et al., 2019). Oh et al. (2017) recommend that social media strategies for fostering consumer engagement should be cohesive across different platforms. Another possible avenue may be to connect with the social media presence of health advocacy groups or other topic-relevant online communities. Thus, researchers have many opportunities to explore how health-related entertainment programming can utilise social media content to support viewership and health communication.
Practical Implications
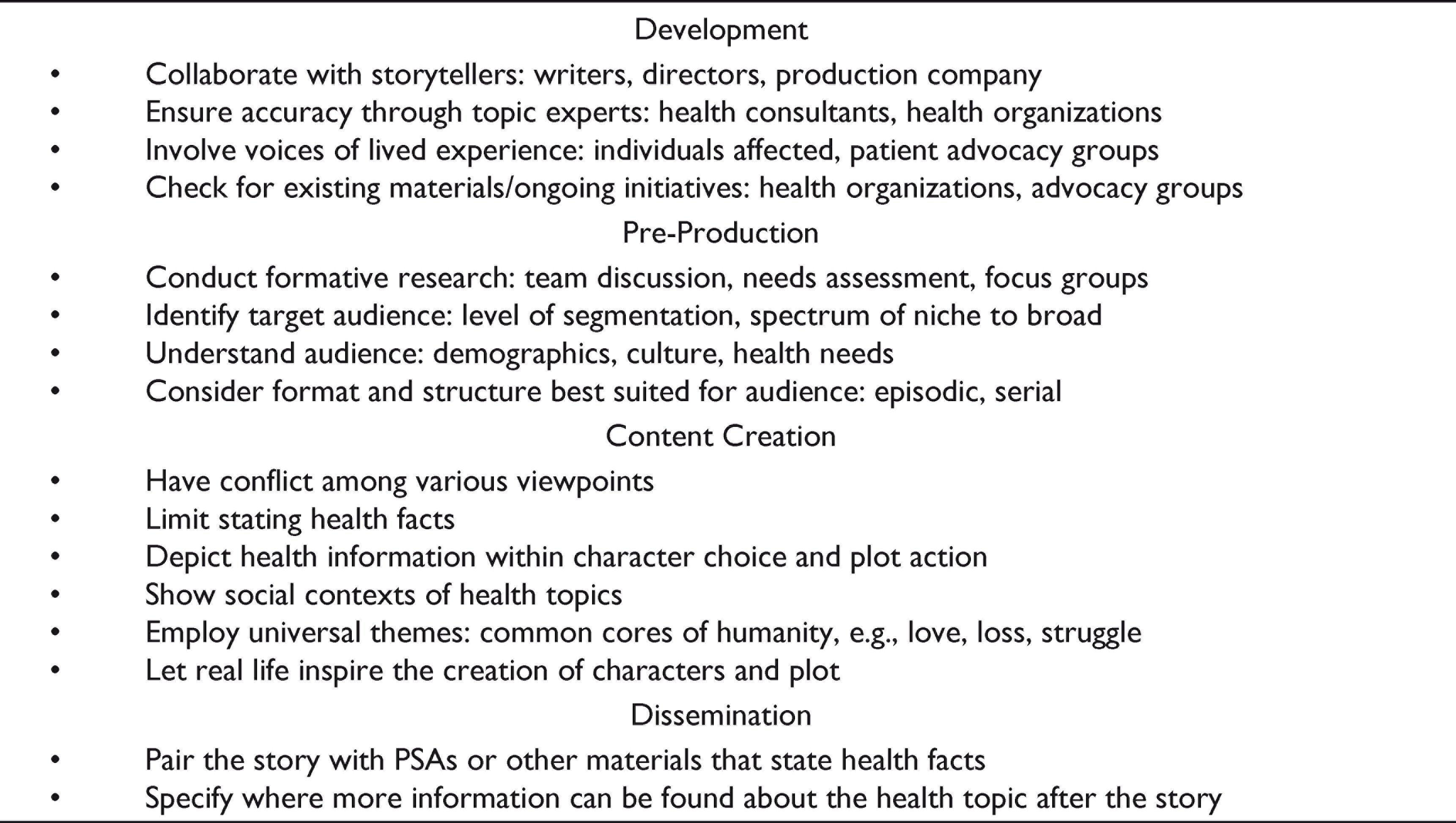
Table 3 presents guidelines for the creation of narrative entertainment to communicate about health, through successfully combining narrative entertainment and health information. The guidelines represent the core findings from grounded theory analysis, which in general supported academic theory and existing resource texts, and are grouped by the narrative process stages of development, pre-production, content creation and dissemination. There is no prioritising within or across groupings—all items are important. In brief, guidance is offered to (a) ensure the right team and right information are leveraged (for development); (b) identify and know the target audience and structure (for pre-production); (c) captivate the audience and emphasise authenticity (for content creation) and (d) supplement health information and provide resources (for dissemination).
Guidelines: Narrative Entertainment to Communicate About Health
Limitations
The narrative medium discussed was constrained to audio-visual content; the process of creating narratives in other genres would be worthy of further study. It was ‘pilot season’ during the period of recruitment and data collection, meaning entertainment industry professionals were at their busiest time of year and recruitment was difficult; more participants would have yielded a richer data set. The current study was also limited to an emphasis on development, pre-production and content creation processes more so than post-production. This aspect should be explored in future research, especially in light of observations that the film experience is increasingly social and is migrating online (Governo et al., 2017). Future studies could therefore explore strategies for generating social media discussion, increased audience reception and sharing within social networks. Ideally, this research would involve potential consumers as partners in the process (Riley et al., 2017). Finally, the study focused on the entertainment industry and health communication practices based in the United States. Other countries, India for example (Anand & Batra, 2016), certainly have flourishing entertainment industries and also utilise EE. This study is meant to complement works written from other cultural perspectives.
Conclusions
This project set out to deepen understanding of the process of creating health narratives meant for widespread dissemination in the United States. We focused on the perspectives of key stakeholders in that process—entertainment industry and health communication practitioners. The guidelines emerging from this project provide direction to health communication practitioners in creating their own content and collaborating with other creative content producers. However, what also became clear was that the question of how to create a story is a difficult one to answer—similar to asking an artist how to make art. Rather than seeking a formula, it may be more realistic to ask about their process. Though there is an art to storytelling, key elements of the creation process (such as choosing teams with complementary strengths, knowing your audience and integrating health content in an authentic way) help clarify and name practical tools for pairing narrative entertainment and health communication.
Footnotes
Acknowledgements
The authors thank Dr Joseph M. Cabosky at the Hussman School of Journalism and Media at University of North Carolina, Chapel Hill, and Dr Parul Jain at the EW Scripps School of Journalism at Ohio University, Athens, for their helpful critique of the study design and results.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.