
Abstract
Objective
Changes to parental presence and engagement in neonatal intensive care units (NICUs) during the COVID-19 pandemic were associated with marked reductions in direct breastfeeding among premature infants. Whether these rates have recovered following the removal of pandemic-related restrictions remains unclear. This study examined direct breastfeeding rates 1 year after the pandemic among premature infants admitted to a NICU.
Methods
A retrospective cohort study was conducted in a level II-III NICU. Sixty-four infants born at ≤34 weeks’ gestation whose mothers intended to breastfeed were included. Infants were grouped as pre-pandemic (n = 28), in-pandemic (n = 12), or post-pandemic (n = 24). The occurrence of direct breastfeeding at the first oral feeding attempt and at hospital discharge was evaluated.
Results
There was a statistically significant difference in the proportion of infants receiving direct breastfeeds at hospital discharge across the three groups: 20/28 (71%) pre-pandemic, 1/14 (8%) in-pandemic, and 2/24 (8%) post-pandemic (p = .001).
Conclusion
Direct breastfeeding rates among premature infants have not returned to pre-pandemic levels despite the removal of visitation restrictions. These findings underscore the continued need for targeted parental engagement and lactation support strategies within NICUs.
Introduction
Breast milk is recognized as the optimal source of nutrition for infants and plays a crucial role in the health of premature infants. 1 Breast milk has been shown to reduce the occurrence of common medical complications associated with preterm birth, such as late-onset sepsis and necrotizing enterocolitis (NEC).1–3 These benefits are further amplified when infants feed directly from the breast, as opposed to receiving expressed breast milk from a bottle, which carries the risks of contamination and degradation of its immunologic and nutritional components during freezing and storage.4, 5
The process of establishing direct breastfeeding in premature infants is multifaceted and shaped by biological, environmental, and social influences.4–7 Infants born before 34 weeks’ gestation typically lack the neurological maturity required to coordinate sucking, swallowing, and breathing, necessitating prolonged reliance on tube feeding and expressed milk. 6 During this period, mothers must maintain milk supply through pumping, often for extended durations prior to the initiation of oral feeding. 7 In addition to these physiological challenges, broader social and contextual factors play a critical role in breastfeeding success.
Parental presence and engagement in the neonatal intensive care unit (NICU) are essential components of breastfeeding establishment. 6 Opportunities for skin-to-skin contact and frequent direct breastfeeding interactions support milk production and infant feeding skills. 6 However, direct breastfeeding outcomes are influenced by broader social determinants of health, including race and socio-economic status (SES). Racial and ethnic disparities are well-documented, with Black and Indigenous mothers facing systemic barriers.6–8 Similarly, lower SES is associated with limited access to breast pumps, lactation consultants, and workplace accommodations for pumping, all of which reduce opportunities for establishing and maintaining direct breastfeeding.
Advances in parental engagement practices over the past three decades have shown that these approaches can significantly improve direct breastfeeding rates in premature infants. 9 Various parental engagement models, such as the Family Integrated Care Model or Creating Opportunities for Personal Empowerment (COPE), have been developed internationally with the primary goal of enhancing the health of infants born preterm.9, 10 Generally, these models promote 24-h parental presence, involvement in daily medical rounds, and participation in parenting activities such as bathing and feeding.9, 11–13 They also encourage early parental interventions like skin-to-skin contact, nonnutritive sucking (NNS), and sensorimotor stimulation. 9 The literature highlights numerous benefits of parental engagement for both parents and infants.9, 11, 12, 14 Infants whose parents engage in these programs show improved weight gain, higher rates of breastfeeding at discharge, and shorter hospital stays. Parents who participate in such programs tend to be more sensitive to their infant’s behavioral cues, feel more confident in their parenting abilities, and experience lower stress levels compared to those who do not participate in any parental engagement initiatives.9, 11, 12, 14
The coronavirus disease 2019 (COVID-19) pandemic has had a tremendous impact on the establishment of direct breastfeeding in premature infants in the NICU, as these parental engagement practices were no longer or minimally practiced.15–21 To reduce contagion, hospitals around the world implemented varying degrees of limitations within their NICUs, including restricting parent visitation hours and the use of personal protective equipment such as gowns, gloves, and masks. As a result, opportunities for direct breastfeeding and parent engagement activities, such as skin-to-skin contact, were greatly limited. A number of studies, including our previous work, observed a significant decrease in lactation support provided as well as the number of infants who received direct breastfeeds or expressed “mother’s own milk” breastfeeds while in hospital during the COVID-9 pandemic.15–20 Lack of breastfeeding support is associated with lower direct breastfeeding rates in premature infants. 22
Although the pandemic is now behind us, its enduring effects may continue to influence parental engagement and, in turn, direct breastfeeding practices. Staff shortages in healthcare, which remain unresolved in our center, may limit lactation support to families. Ongoing parental anxiety about infection transmission, coupled with limited understanding of how viruses spread, may also affect parents’ engagement in the NICU and their comfort with direct breastfeeding. 23 While early pandemic studies showed declines, it is unclear whether direct breastfeeding rates have recovered post-pandemic, which this study aims to evaluate.
Methods
Study Design and Setting
An observational, retrospective cohort study was conducted in the NICU at the Kingston Health Sciences Centre. The NICU is a level II-III unit with a maximum capacity of 26 beds and cares for approximately 400 infants per year. The NICU provides care centered on the Family-integrated Care (FiCare) model. The FiCare model allows for 24-h parental visits, supports parental involvement in medical rounds, and encourages parents to provide bathing and feeding, and to administer certain interventions, such as skin-to-skin contact and NNS on an emptied breast. From March 16, 2020, to July 2020, during the first wave of the pandemic, the NICU restricted parental visitation to only one parent at a time for a maximum of 3 h per day, and parents were required to wear personal protective equipment, including face guards, masks, and gowns. Throughout the pandemic, in July 2020, this was changed to a maximum of 6 h per day, with only one parent visiting at a time, and parents were required to wear masks. In August 2023, the NICU returned to practicing the parental engagement practices from prior to the first wave of the COVID-19 pandemic.
Participants
To be included in the study, mothers had to: (a) intend to breastfeed at admission; (b) be recognized as decision-makers according to hospital policy; (c) have an infant(s) born at ≤34 weeks’ gestation because they most often receive tube feedings due to their inability to coordinate sucking, swallowing, and breathing; and (d) the infant(s) does not have any heart or oral congenital anomalies, metabolic disorders, or genetic syndromes. These criteria were chosen to ensure that the participants had a uniform intent to direct breastfeed their infant and that mother-infants were separated for an extended period. Mothers and their infants who were part of other breastfeeding studies on the unit were excluded due to the potential confounding, as were mothers and their infants who were “outborn,” meaning they transferred into the NICU from another regional hospital, due to the high likelihood that they may be transferred back to their original hospital prior to meeting the study outcomes.
The sample of participants consisted of three groups. The first group included infants who were born prior to the pandemic, between March 2017 and March 2018 (1 year, pre-pandemic, n = 28). The second group consisted of infants born during the first year of the pandemic, from March 2020 to March 2021 (1 year, in-pandemic, n = 12). The third group consisted of infants who were born after lifting the COVID-19 parental visitation restrictions, from August 2023 to June 2024 (approximately 1 year, post-pandemic, n = 24).
Outcomes
The outcomes from this study were twofold: occurrence of direct breastfeeding at the first feed by mouth regardless of corrected gestational age (proportion, %), and occurrence of at least one direct breastfeeding at hospital discharge (proportion, %). The occurrence of direct breastfeeding at hospital discharge was defined as at least one oral feed directly from the breast within 24 h prior to discharge home to reduce any biases in this outcome because of the 3-h visitation restriction policy during the in-pandemic period. These data were extracted from electronic medical records.
As maternal factors can have potential effects on direct breastfeeding, the following maternal characteristics/factors were monitored: maternal age, prenatal care, being a first-time mother, and participation in skin-to-skin contact with their infant. Infant factors that have been found to influence oral feeding skills in premature infants were also recorded. These include birth weight, gestational age, gender, twin, and the existence of any sustained neonatal morbidities, such as intraventricular hemorrhage (IVH) III or IV, sepsis, NEC, or bronchopulmonary dysplasia (BPD).
Procedure
Three researchers were trained in data abstraction and blinded to the study objectives.
Each researcher was responsible for abstracting data pre-pandemic, in-pandemic, or post-pandemic. The following procedure was followed to ensure ethical conformity and eligibility: (a) The researcher first reviewed electronic medical records from the study period to determine eligibility for inclusion in the study. (b) Following this, the researcher verified that each participant had provided their consent for the use of their data from their electronic medical chart for research purposes. (c) Data for direct breastfeeding outcomes, maternal factors, and infant factors were abstracted from electronic medical records. (d) To ensure accuracy, all data collected were cross-referenced by another researcher. The study protocol was reviewed and approved by the university and affiliated hospitals’ Research Ethics Board. Participant ethical consent was not applicable because it was a retrospective study.
Statistical Analysis
The sample size for this study was determined using a non-probability convenience sampling technique. As such, the study was not a priori powered to detect specific effect sizes, and the findings are interpreted as descriptive and exploratory. Due to the limitations of the sampling method, generalizability and statistical power are limited. Statistical analyses were limited to Chi-square and Fisher’s exact tests to assess the occurrence of direct breastfeeding at the first oral feed attempt and at hospital discharge across three time periods: pre-pandemic, in-pandemic, and post-pandemic. There were no missing data regarding the occurrence of direct breastfeeding at the first oral feeding attempt and at hospital discharge, as these variables are mandatory for nurses to document in the medical record. Effect sizes, using Cramér’s V, are reported for Chi-square analyses to provide additional context for the magnitude of observed associations. For baseline maternal and infant characteristics, Chi-square tests were used to compare categorical variables, while one-way analysis of variance (ANOVA) was used for continuous variables. A significance level of p < .05 was used throughout, and analyses were conducted using SPSS version 29.0.
Results
The total sample size for this study was 64 participants, comprised 28 infants born pre-pandemic, 12 infants born in-pandemic when parental restrictions were in place, and 24 infants born post-pandemic following removal of all parental visitation restrictions. As illustrated in Table 1, all three groups had similar maternal and infant baseline characteristics, except for sex (p = .001) and twin (p = .043).
Baseline Characteristics.
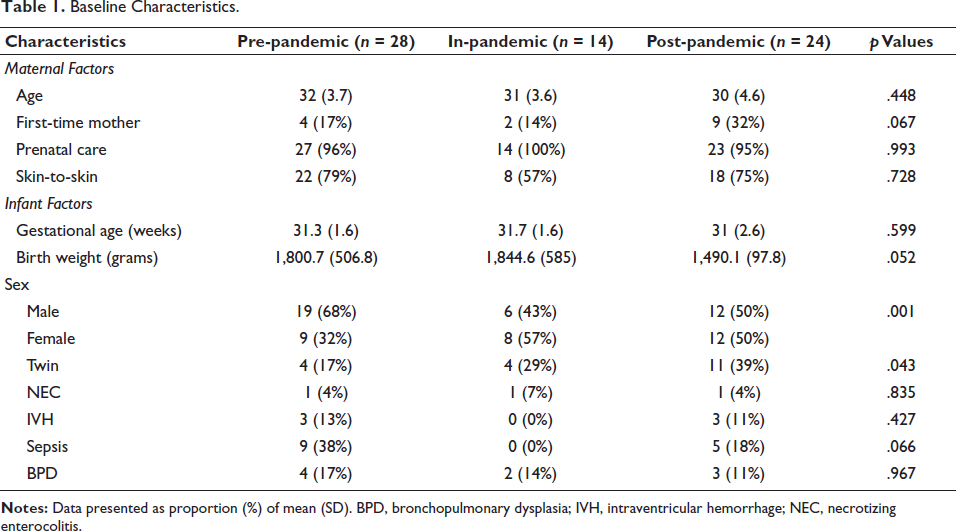
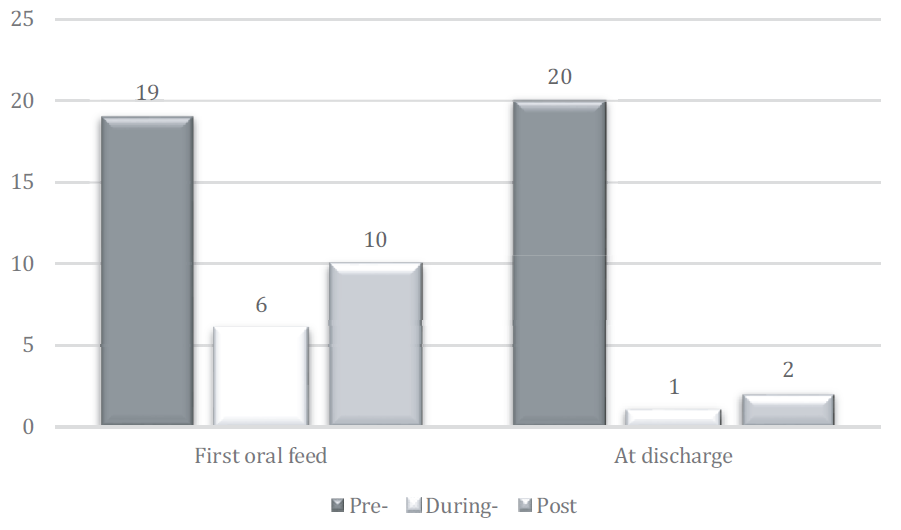
Figure 1 illustrates the results for direct breastfeeding occurrence at the first oral feeding and at discharge. There was no statistically significant difference between the three groups with regard to the occurrence of direct breastfeeding when infants started to feed by mouth (first oral feed attempt), χ² (1, N = 64, r = 2.053, p = .109), and the associated was strong Cramer’s V = 0.652. However, there was a statistically significant difference in infants who received direct breastfeeding at hospital discharge χ² (1, N = 64, r = 27.235, p = .001), and the association (effect size) was strong Cramer’s V = 0.652. Furthermore, when performing post-hoc group comparisons, there was a significant difference between the pre-pandemic group versus the in-pandemic group (20/28 (71%) vs. 1/12 (8%), p = .00025), and the pre-pandemic group versus the post-pandemic group (20/28 (71 %) vs. 2/24 (8 %), p = .01). There was no significant difference between the in-pandemic and post-pandemic group (1/12 (8 %) vs. 2/24 (8 %), p = 1.0).
Discussion
The aim of this study was to assess the rate of direct breastfeeding, post-pandemic, among premature infants in a level II-III NICU. The results suggest that the pandemic in this single-center study may have changed parent engagement approaches in the NICU in ways that have enduringly and negatively impacted direct breastfeeding outcomes in premature infants.
When all three groups were compared, the pre-pandemic group, the in-pandemic group, and the post-pandemic group, the proportion of infants that started oral feeds directly from the breast was the same in all three groups. This is likely due to a unit guideline informed by our previous study, which demonstrated that the method (bottle or breast) of the first feed influences direct breastfeeding establishment at hospital discharge. 24 However, a significantly fewer number of infants received direct breastfeeds at hospital discharge in both the in-pandemic and post-pandemic groups when compared to the pre-pandemic group. Specifically, direct breastfeeding rates of premature infants significantly decreased in-pandemic when parent visitation restrictions were in place,16, 18, 20 and these rates remained significantly low post-pandemic when parental visitation restrictions were lifted. The continued low rates of direct breastfeeding post- pandemic that have been observed in this study can be attributed to several factors, including stricter enforcement of hospital policies for infection control, healthcare professional shortage, misinformation on the spread of viruses, and parent psychological distress. 17
At the peak of the pandemic, many hospitals, including our center, implemented strict visitor restrictions to reduce the spread of COVID-19, and although visitor restrictions have since been lifted, some policies remain in place that may hinder direct breastfeeding.17, 24, 25 For instance, the study was conducted at the Kingston Health Sciences Centre, parents continue to be encouraged not to visit their infant in the NICU if they demonstrate any signs or symptoms of any virus. This often limits or entirely prevents parents from visiting their infants in the NICU, thereby reducing opportunities for mothers to practice direct breastfeeding on a frequent basis, which is essential for stimulating milk production and for establishing a direct breastfeeding routine. 26 Another factor is healthcare professional shortages, and consequently, the reassignment of healthcare professionals to other roles and mandates by hospitals. 17 At our center, prior to the pandemic, lactation support services consisted of neonatal nurses specialized in lactation who provided education and support on an as-needed basis to all mothers whose intention was to breastfeed. During the pandemic, these nurses were redirected to other critical care areas, thus reducing the support available for breastfeeding mothers. However, we continue to experience shortages of healthcare professionals, and consequently, those lactation services have yet to be fully resumed. Hence, there are now fewer opportunities to provide education and support to mothers who would like to breastfeed than there were pre-pandemic.
The pandemic has significantly heightened public awareness of how viruses spread and the extent to which they can impact our health. However, there has been an abundance of misinformation associated with the spread of viruses that may persist or a lack of understanding about the safety of breastfeeding during a virus, which may continue to influence some mothers to be reluctant about direct breastfeeding or to avoid direct breastfeeding altogether post-pandemic. Furthermore, parents may have experienced extreme psychological stress as a result of the pandemic. 27 The concern about the health of their infant and their level of understanding of the risk of any virus transmission may contribute to mothers feeling overwhelmed and less secure about direct breastfeeding their infant.
Although our study results reveal that direct breastfeeding rates have not returned to pre-pandemic levels. There are several measures that can be taken to return direct breastfeeding rates back to pre-pandemic levels. Having or restoring consistent access to lactation consultants is one such measure, as there is a direct correlation between consultation with a lactation specialist and direct breastfeeding establishment among premature infants in the NICU. 28
Furthermore, having in place specific breastfeeding education in the NICU has also been found to increase the rate of direct breastfeeding. Lastly, offering parental engagement opportunities, such as continued promotion of skin-to-skin and NNS on an emptied breast, has also been found to increase rates of direct breastfeeding in the NICU.26, 29 In our unit, we are now offering more breastfeeding education programs as well as peer-parent support programs.
We anticipate that these measures would be beneficial in improving direct breastfeeding rates among premature infants in the NICU.
Limitations
This study has several limitations. The retrospective study design made it difficult to cross-reference any errors within the documentation. However, the data were collected by one researcher and verified by another researcher to ensure that the abstracted data was accurate. Furthermore, the retrospective study design entailed missing data and relying only on data included in the participants’ electronic medical charts. For instance, maternal factors, such as SES and having a social support network, can influence direct breastfeeding established. However, they were not considered because the data were not available in the electronic medical charts. Another limitation of the retrospective study is the lack of adherence to engagement practices in the unit as we cannot follow the fidelity to the FiCare practices and adherence to the COVID-19 policies. Due to the small sample size, single-center design and the use of a convenience sampling method, the study was underpowered for more complex analyses. As a result, only bivariate analyses (e.g., Chi-square tests) were conducted, and potential confounding variables such as infant sex and twin status were not adjusted for. These factors may influence direct breastfeeding outcomes; therefore, the results should be interpreted with caution and may affect the interpretation of associations.
Conclusion
The pandemic brought about significant challenges that continue to impact direct breastfeeding rates among premature infants in the NICU. The findings from this study suggest the need to focus on enhancing lactation supports for families, with the goal of increasing direct breastfeeding rates in premature infants to pre-pandemic levels.
Footnotes
Acknowledgment
The authors thank Ms. Wilma Hopson for her assistance with the statistical analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by Queen’s University Human Subject Research Ethics Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.