
Abstract
In this deeply personal narrative, I share my journey as both a primi mother and a pediatrician, offering a dual perspective on the intricate world of breastfeeding. This exploration intertwines my own lived experiences with the professional insights I’ve gained through years of medical practice.
Introduction
As a dedicated paediatrician and an advocate for exclusive breastfeeding, I have counselled numerous mothers about the benefits of proper positioning, attachment, and the importance of exclusive breastfeeding. However, my own journey as a primi mother taught me valuable lessons about the realities of breastfeeding that I had not fully appreciated before.
Section 1: The Personal Journey as a Primi Mother
When my baby was born at 37 weeks, weighing 2450 grams, and experienced Transient Tachypnea of the Newborn (TTNB), my breastfeeding journey began with unexpected challenges. The initial separation from my baby and the use of formula as his first feed in the nursery triggered fear and anxiety that I might face challenges in breastfeeding due to the non-practice of breastfeeding within the first hour and rooming in.
Despite my knowledge about breastfeeding, I encountered difficulties when trying to breastfeed my own child. I could not latch the baby to my breast in the first two to three days of the postpartum period without support, no matter how hard I tried. My lactation counsellor became my lifeline, providing the support and guidance I desperately needed. With her help, I could latch my baby comfortably, but every feeding session needed help with positioning and attachment during the first week. However, I was confident and comfortable that the issues would be resolved.
Nevertheless, the journey of struggle continued, and I faced latching issues that required consistent support during every feeding session. A new problem arose—persistent nipple pain with no visible injury and intermittent bouts of painful cramps in the breast. These issues happened prior to breastfeeding during letdown and also in between the feeds, giving me chills of pain, fear, anxiety, and depression. I reached a state of fearfulness towards the baby by the end of the first month.
When I struggled for help, my family and community tried a lot as per their knowledge with conflicting guidance, and I could not get any professional support from trained professionals in my small native district after my initial post-partum period. I finally had to call a healthcare professional experienced in breastfeeding, who found problems in my positioning and attachment techniques through video and advised small modifications based on mine and the baby’s technique. This helped to improve my breastfeeding process and exclusively breastfed my baby till six months.
Through three to six months, I could comfortably breastfeed with little support, and then I had to join back work. I could not take my baby with me and had to abruptly wean him off after a period of six months of exclusive breastfeeding. I have experienced the proper joy of successful breastfeeding, cherishing the unique bonding experience it offered even with all these challenges.
Section 2: The Professional Insights as a Paediatrician
As a paediatrician, my breastfeeding journey offers unique insights into the challenges that many mothers face despite having knowledge and motivation. The initial struggles with latching, the need for consistent support, and the emotional rollercoaster of fear, anxiety, and depression underscore the difficulties that can accompany breastfeeding, especially for first-time mothers.
Emphasizing the evidence-based advantages of breast milk, including immune system support, optimal nutrition, reduced risk of infections to baby, and advantages to mother as protecting from breast cancer, ovarian cancer, hypertension and Type 2 Diabetes has always been a core aspect of my professional role. However, my own experiences have deepened my understanding of the real challenges that mothers may encounter on their breastfeeding journeys. Personally feeling the pain during milk let-down, I demonstrated my determination to breastfeed by taking analgesics daily to ensure continued breast milk provision to my child, but this also highlights the crucial role of professional support needed in breastfeeding.
Reflecting on the emotional aspect of my journey, from the initial fear triggered by separation and formula use to the eventual joy of successful breastfeeding, sheds light on the emotional complexities that many mothers face during this period. The struggles encountered, both physical and emotional, are common including challenges of returning to work and the decision to wean. The emotional aspects of weaning, including feelings of guilt and pain, resonate with many mothers who grapple with the delicate balance between work and breastfeeding.
In essence, my experience offered me a paediatrician’s perspective on the highs and lows of the breastfeeding journey, emphasizing the importance of professional support, perseverance, and the unique bonding experience that breastfeeding brings. It served as a testament to the strength and resilience of mothers navigating the intricate complexities of motherhood. With patience, perseverance and support, many new mothers will be able to overcome any challenges they may face.
Section 3: Bridging the Gap: Challenges and Solutions
My experiences have led me to contemplate why exclusive breastfeeding rates are disappointingly low in India and beyond. Generational wisdom is not being passed on to modern moms due to weakening family ties. In traditional joint families, grandmothers or great-grandmothers naturally supported lactation. Still, in modern times, this support system has diminished. According to the National Family Health Survey (NFHS 5), the initiation of breastfeeding within the first hour of life is 44%, and the exclusive breastfeeding rate till six months is 55%. 1 Barriers to exclusive breastfeeding include a lack of prenatal education, lack of confidence, perception of insufficient milk, misinterpretation of normal infant crying, inadequate professional support, comfort and ease in formula-feeding maternal employment, and early introduction of solids. 2 A meta-analysis identified factors associated with breastfeeding initiation and continuation. High-impact factors included the mode of delivery, parity, dyad separation, maternal education, and professional support, including smoking. 3
Breastfeeding faces challenges in today’s market-driven world, necessitating reforms across various attributes. Demographic factors like age, education, family size, and socio-economic status are crucial, as are psychosocial elements such as maternal beliefs and a supportive social network. Counselling interventions, whether face-to-face or telephonic, delivered at least four times postnatally in the first month, were proven effective in promoting exclusive breastfeeding and reducing anxiety. 4 Community attributes, including local knowledge and action, create a breastfeeding-friendly environment. In low- to middle-income countries, community-based peer support increases exclusive breastfeeding rates at three months (RR 1.90, 95%CI: 1.62–2.22), and six months (RR 3.53, 95%CI: 2.49–5.0), while decreasing pre-lacteal feeds (RR 0.38, 95%CI: 0.33–0.45). 5 Peer counsellors with similar cultural routines provide valuable support. Social media groups offering community support are also appreciated, although challenges include reliability and a lack of regulation. 6
Healthcare attributes are vital considerations, involving well-established healthcare routines, consistent advice, collaboration between healthcare and peer support groups, and ensuring early discharge practices. Intervention effects of Baby-Friendly Hospital Initiatives (BFHI), including policies in maternity areas like rooming in, early maternal contact, are known to increase the rate of exclusive breastfeeding for six months (OR 5.21, 95%CI: 2.15–12.61), professional provider-led intervention (OR 2.76, 95%CI: 1.76–4.33), having a protocol available for the provider training program (OR 2.87, 95%CI: 1.89–4.37), and implementation during the prenatal and postnatal periods (OR 3.32, 95%CI: 1.83–6.0). 7
Regular postnatal visits, comprising three to six contacts of 20–30 minutes each, are crucial for continuous breastfeeding support. Home-based postnatal visits (HBPNC) by midwives on the 3rd, 7th, 14th, 21st, 28th, and 42nd days after birth have the potential to address breastfeeding issues. However, a challenge lies in the skills and attitudes of midwives. Breastfeeding training programs for midwives significantly improve outcomes, leading to longer exclusive breastfeeding durations, fewer challenges, higher satisfaction, and reduced use of breast milk substitutes. 8 Prioritizing training programs and incentives for midwives attending HBPNC visits is imperative. This involves providing skills for latch-on techniques, necessary equipment, and addressing common concerns, fears, and myths to ensure effective and supportive breastfeeding care for mothers. Additionally, dedicated lactational consultants and specialists play a vital role in increasing breastfeeding initiation and rates, especially in situations falling outside the scope of midwives. 9
Public policy also plays a pivotal role, encompassing official recommendations, maternity leave benefits, the training of healthcare staff, and the implementation of national plans like MAA (Mother’s Absolute Affection) to promote breastfeeding. In an Indian Institute of Human Settlements survey of 120 working mothers, it was found that only 27% of mothers could continue breastfeeding during working hours, 83% faced challenges, and 34% identified the biggest challenge as a lack of nursing facilities. 10 Mothers should feel comfortable nursing in public. Incorporating technology for breastfeeding support by remote interventions can also be effective for breastfeeding support and education. Virtual lactation support with remotely provided breastfeeding assistance is the solution to the problems with manpower, geographical constraints and health systems. In a meta-analysis conducted by including 26 studies, remotely provided breastfeeding support significantly reduced the risk of women stopping exclusive breastfeeding at three months by 25% (RR: 0.75, 95%CI: 0.63–0.90). 11 By addressing these multifaceted attributes, we can work towards creating an environment that facilitates and supports breastfeeding in the face of evolving challenges (Figures 1).
Critical Phases of breast feeding support.
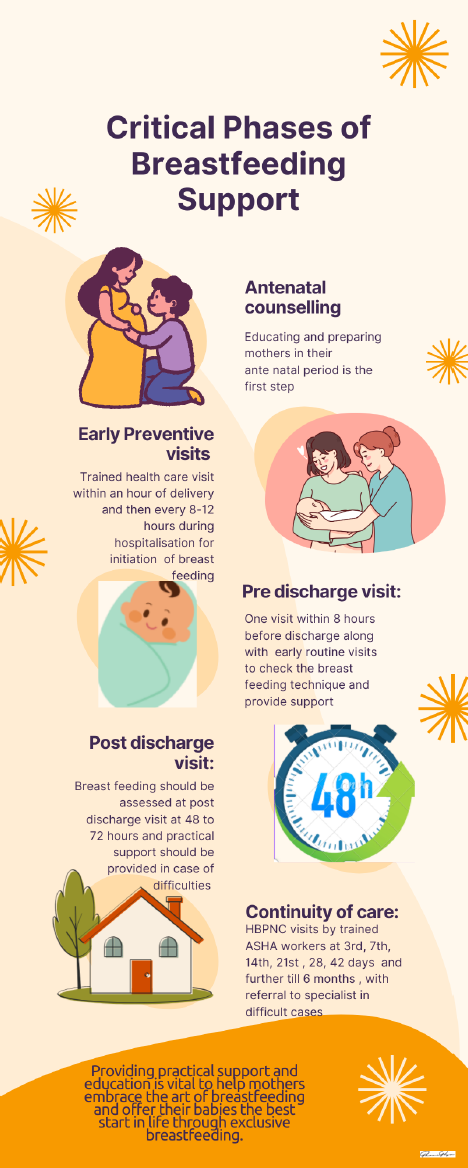
Verbal advice is often insufficient; what mothers truly need is hands-on, practical support to master proper positioning and attachment. Organizations like Breast Breastfeeding Promotion Network of India and international bodies must also prioritize training healthcare providers to offer comprehensive breastfeeding support. By equipping healthcare professionals with practical skills, we can empower mothers to overcome breastfeeding challenges and continue our culture of breastfeeding.
Conclusion
My journey as a primi mother and paediatrician has taught me that breastfeeding is not always easy, even for those well-versed in its benefits. Providing practical support and education is vital to help mothers embrace the art of breastfeeding and offer their babies the best start in life through exclusive breastfeeding.
Footnotes
Declaration of Conflict of Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Disclosures
There is ethical approval sought from institute as this is my own personal experience and I give my consent for sharing this.
Funding
The author received no financial support for the research, authorship and/or publication of this article.