
Abstract
Background
There is often a delay in the initiation of feeding in preterm babies and more dependence on PDHM milk due to the non-availability of the mother’s own milk. This study aimed to increase the percentage of very preterm neonates receiving expressed breast milk (EBM) within 24 hours of birth.
Methods
A quality improvement (QI) initiative study was conducted from May 2022 to August 2022 in a tertiary care (Level III-B) NICU. A QI support team was formed. The reasons for the delay in the initiation of expression of breastmilk were evaluated. We included preterm neonates (<32 weeks gestation) born within the study period. Antenatal and postnatal counseling regarding the expression of breast milk, using leaflets and video, frequent visits, telephonic reminders, and emphasizing Kangaroo Mother Care through various Plan-Do-Study-Act cycles were done.
Results
A total of 17 very preterm babies were studied over a period of 3 months. The percentage of preterm receiving EBM within 24 hours of birth, increased from 20% (observation phase) to 83.3% (initiation phase) and maintained to 90% in the continuation phase. The time of receiving the first EBM reduced from a median of 32.5 hours (1.35 days) in the retrospective phase to 17 hours (0.7 days) during the initiation phase and it was sustained later on. Mothers were able to express as early as within 4.5 hours.
Conclusion
A simple QI intervention showed early expression and sustenance of breast milk in mothers of preterm neonates.
Introduction
The benefits of a mother’s own milk (MOM) as a primary source of nutrition in preterm neonates are well-known. MOM plays an important role in reducing the risk of late-onset sepsis (LOS), necrotizing enterocolitis (NEC), 1 retinopathy of prematurity, and bronchopulmonary dysplasia and improves neurodevelopmental and cognitive outcomes. 2 Preterm babies are not able to feed directly from the mother’s breast due to prematurity and other related complications. Therefore mothers need to express their milk for feeding and ensure sufficient milk output, however, there is often a delay in the expression of breast milk. Studies show that mothers who start expressing milk within 1 hour, produce more milk compared to those who delay. 3 It is recommended to start expressing milk within 6 hours after delivery (8–10 times per day) including once in the night-time to establish feeding. 4 Early usage of colostrum to the buccal mucosa has additional immunologic benefits to the preterm, facilitates milk production in the mother, 5 and helps to reach enteral feeds earlier. According to the American Academy of Pediatrics, PDHM (Pasteurized donor milk) has been recommended as the next best choice of nutrition for very low-birth infants when mother milk is not available, but in order to make it usable, the donor milk has to go through pasteurization, thawing, and prolonged storage. In this process, it loses its bioactivity. PDHM can be considered as a “bridge” until mother’s milk is available, but lacks additional benefits like reduction in LOS, or neurodevelopment. 6
Retrospective data from our tertiary care (Level III-B) neonatal unit suggests various causes that led to the delayed initiation and maintenance of breastfeeding by mothers of preterm neonates. It was noted that mothers were not motivated enough to express milk within 24 hours of birth because of anxiety, stress, pain, lack of knowledge, and family support. Eventually, neonates were forced to be kept nil by mouth or be dependent on donor milk (PDHM) for nutrition. So keeping this in mind, we initiated a quality improvement (QI) program to improve the percentage of preterm infants receiving expressed breast milk (EBM) within 24 hours of birth. We took preterm infants (<32 weeks) for the study hoping that if we are able to see improvement in the attainment of “mother’s own milk” in these babies, then similar translational changes can also be brought in other neonates at higher gestational age.
Methods
The study was carried out over a period of 12 weeks (May 23, 2022, to August 15, 2022) at a tertiary care neonatal ICU (Level III-B). The institutional review board and scientific and ethics committee approved the QI project and informed consent was taken from the parents of the babies. In this study, we included all very preterm babies less than 32 weeks of gestation admitted to our NICU and excluded the ones who were sick, had congenital malformations, NEC (and other conditions that preclude early trophic feeding with MOM), or whose mothers were very sick.
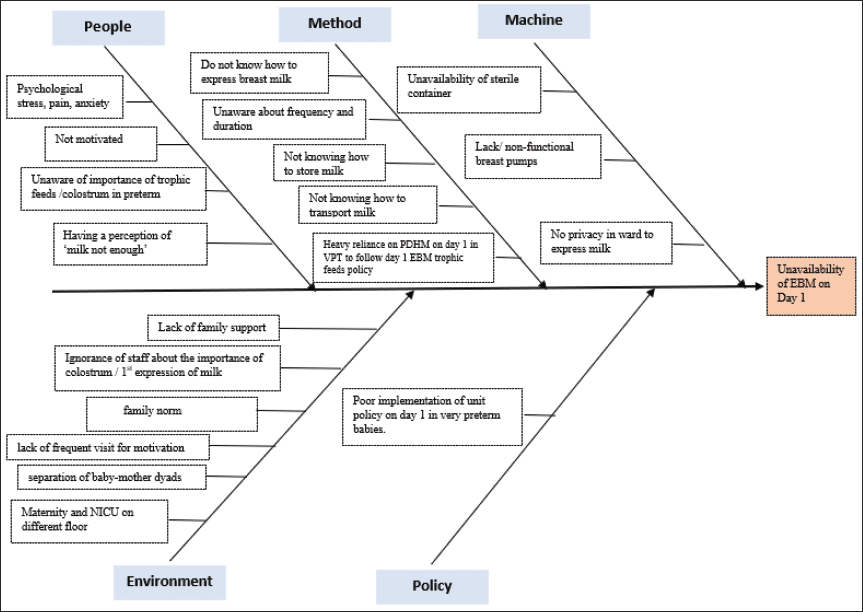
A QI support team including a neonatologist, NICU residents, a nurse in charge of NICU, ward, maternity, and a lactation counselor promoting “Mother’s only milk” was formed. Baseline data was collected retrospectively (observation phase) from 3 months prior to the study. Time and quantity of milk received for the first time by neonate from day 1 until day 7 were recorded. A fishbone analysis was done (Figure 1) to know the root cause of the delayed establishment of breast milk. Inputs from team members were also considered. Predominant barriers were lack of sensitization, knowledge, motivation, family support, and poor implementation of unit policy. Interventions were focused on improving the above-mentioned factors (Table 1).
Fish Bone Analysis Showing the Main Reasons for the Delay in Initiation of Milk Expression and Availability of EBM (VPT, Very Preterm).
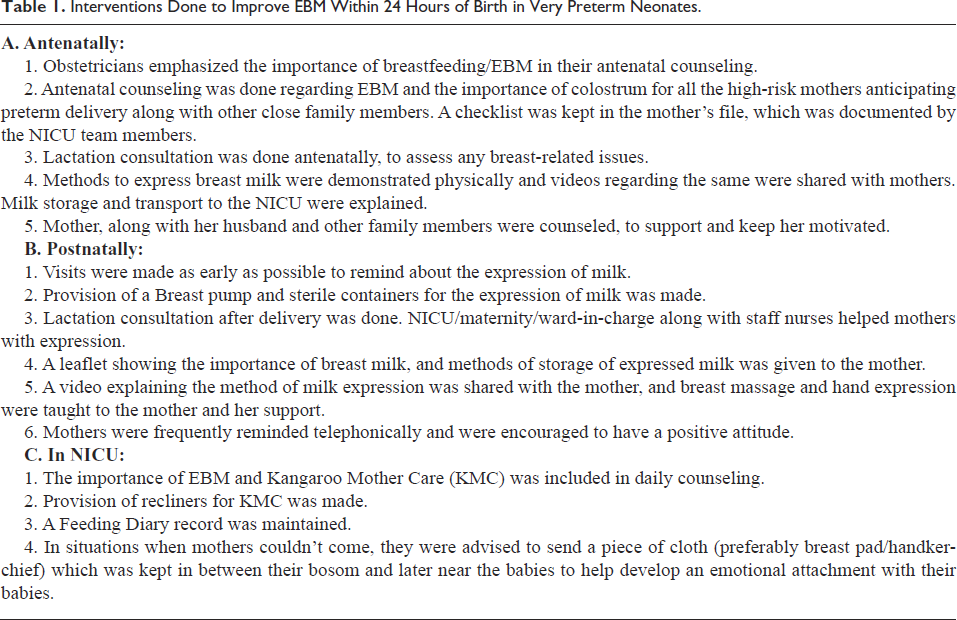
Interventions Done to Improve EBM Within 24 Hours of Birth in Very Preterm Neonates.
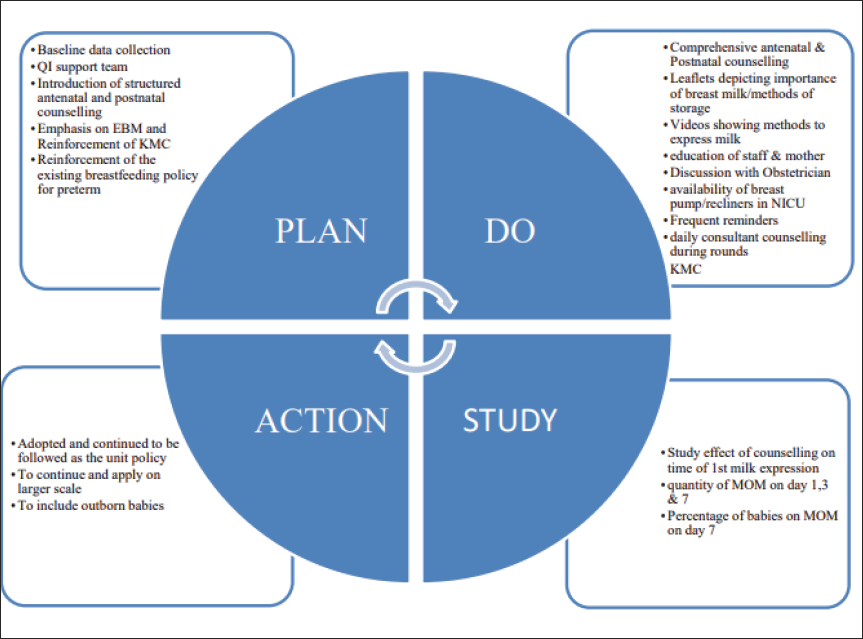
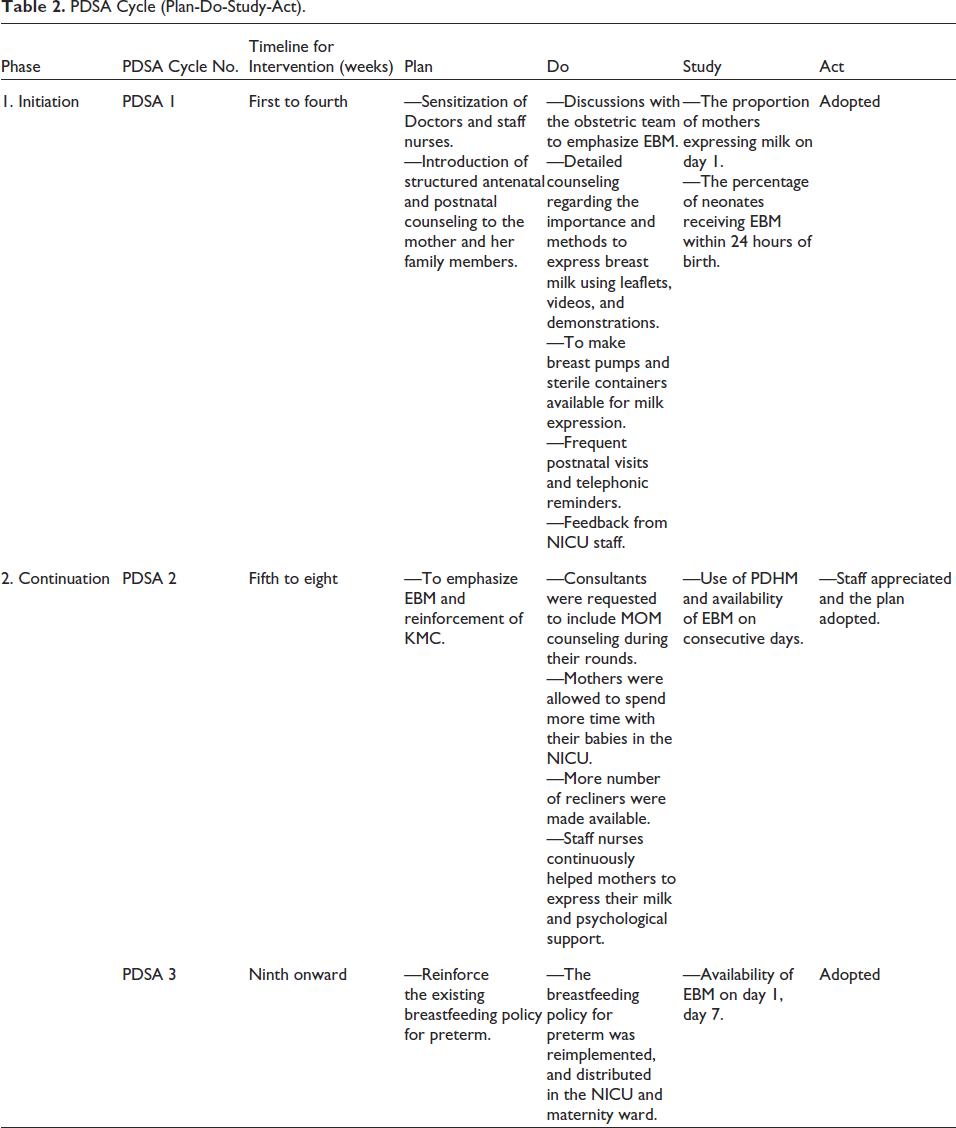
The intervention phase was carried out in two phases, the initiation phase and the continuation phase. The initiation phase was done over a period of 4 weeks in a Plan-Do-Study-Act (PDSA) cycle and the continuation phase was done from the 5th week onwards with various PDSA cycles with additional interventions along with structured counseling (explained in Figure 2 and Table 2).
PDSA Cycle (Plan-Do-Study-Act): Depicting a Continuous Feedback Loop, KMC, Kangaroo Mother Care, MOM, Mother’s Own Milk.
PDSA Cycle (Plan-Do-Study-Act).
A comparison of data from the initiation and continuation phases was done with baseline values. Data were described in medians and interquartile ranges. The study measured the percentage of preterm babies who received EBM within 24 hours of birth, the time of receiving their first EBM, amount of breast milk received on day 1, day 3, and day 7 of life.
Results
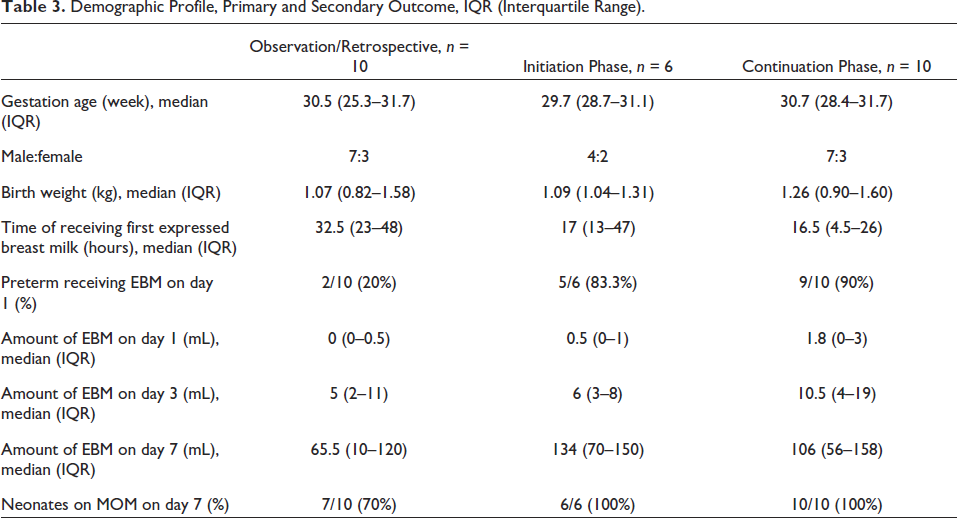
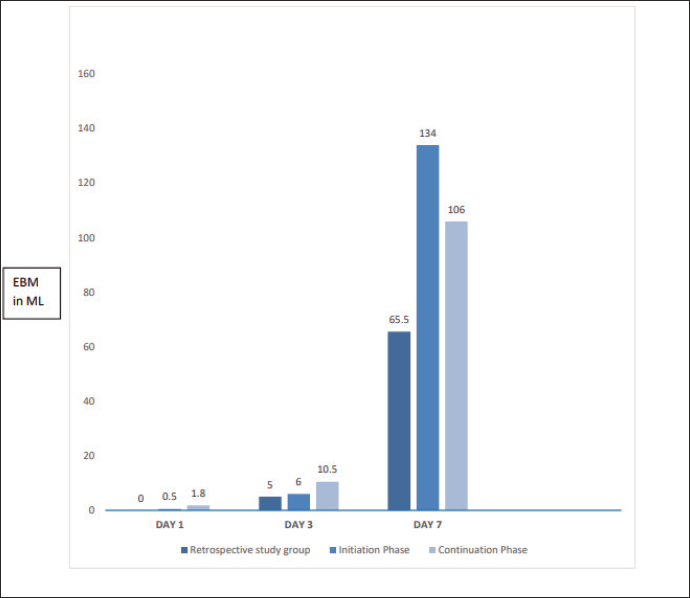
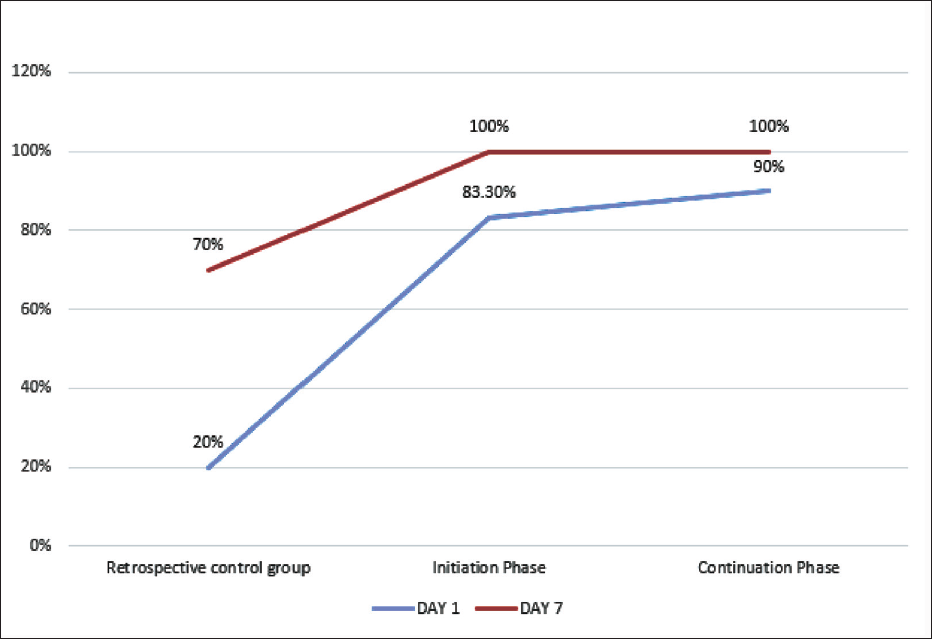
During the study period, 123 neonates were delivered. Of which a total of 17 neonates born before 32 weeks were admitted to the NICU. Sixteen babies fulfilled the inclusion criteria and one was excluded as his mother was admitted to the ICU. The baseline data of the study population has been depicted in Table 3. These babies were studied under the “initiation phase” and “continuation phase” as well as the results were compared with retrospective data. After 4 weeks of the initiation phase, the percentage of preterm receiving EBM within 24 hours of birth increased considerably and was sustained later. The time of receiving the first EBM also reduced significantly. Mothers were able to express as early as within 4.5 hours. The amount of expressed milk received on day 1, day 3, and day 7 increased significantly (Figure 3). Babies on only mother’s milk on day 7 increased to 100% in the initiation phase and remained so in the continuation phase (Figure 4).
Demographic Profile, Primary and Secondary Outcome, IQR (Interquartile Range).
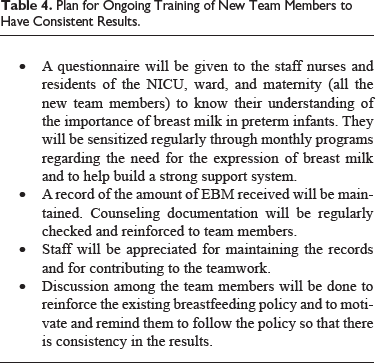
Plan for Ongoing Training of New Team Members to Have Consistent Results.
Amount of EBM Received on Days 1, 3, and 7 (in mL) in the Retrospective Study Group, Initiation Phase, and Continuation Phase.
Percentage of Neonates Receiving Expressed Breast Milk on Day 1, and Only on Mothers Milk on Day 7.
Discussion
There have been many QI initiatives to improve mother’s milk for preterm infants through various hospital breastfeeding support practices. Using a QI Bundle having several interventions will help to attain desired goals. Systemic Review and Meta-analysis done by Fang et al. 7 shows that a total of 12 interventions were used in the QI bundle. The most common is a multidisciplinary expert team developing evidence-based interventions and educating hospital staff and parents. For early initiation of milk expression, the availability of breast pumps was increased, and oropharyngeal administration of colostrum was done. For maintenance of lactation, emphasis on skin-to-skin care, and non-nutritive sucking was done along with follow-up visits and reminders were given by phone calls. This study improved the percentage of very preterm infants receiving mother’s only milk within 24 hours of birth using similar methods. It was noted that simple interventions through PDSA cycles, both antenatally and postnatally can promote early expression of milk resulting in increased MOM production.
A study done by Bagga et al., 8 in 2018, shows improvement in the first EBM from a median age of 2.5–1.16 days. Our study also had similar findings, with a reduction in the time of receiving the first EBM sustained in the continuation phase. Our results were similar to other studies.9, 10, 11
The strength of this QI initiative helped to emphasize MOM as the first choice of nutrition for preterm babies and attain EBM on day 1, and not be completely dependent on PDHM alone. After this QI study, we achieved sustenance from a PDHM unit by adopting early trophic feeds following organized nutrition strategies. MOM was used instead of PDHM, for colostrum swabbing, and also in the later phases. A brief plan to train the new team members to have consistent results has been described in Table 4.
The limitation of the study was having a small population size, so the effect of each intervention could not be analyzed separately.
Conclusion
To conclude, mothers of preterm babies were more motivated and took the initiative to express breast milk as early as possible through our QI interventions. This was in contrast to the delay in expression noted earlier as mothers were complacent due to the availability of PDHM. Existing donor milk banks have erratic supply, so self-sustenance in our NICU using only MOM has become a cheaper and better option. We planned to sustain this improvement by reinforcing the breastfeeding policy for preterm and applying it on a larger scale.
To have a preterm infant in the NICU is very stressful for parents. Mothers need continuous support from their loved ones in order to have a positive attitude, self-confidence, and consistency in expression and maintenance of milk supply. Her fear can also be relieved if she interacts with other mothers facing similar issues. In this technology-filled world, a mother’s club for preterm can be made which will include all recent NICU graduates willing to join along with the admitted preterm, where they are free to discuss their problems, give testimony, and share experiences. Also, 24 × 7 lactation-related queries can be sorted out. In our study, outborn preterm were not included. A Breastfeeding policy should be made for these infants too to help them benefit from their MOM.
Footnotes
Acknowledgement
We acknowledge the sincere contributions of all the consultants, colleagues, residents, staff nurses, and sisters in charge of the NICU, Maternity, and ward.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent Statement
A written informed consent for participation in the study was taken from the parents of babies.