
Abstract
Background
Admission of a newborn to neonatal intensive care unit is very stressful for family and poses significant financial burden.
Aim
To estimate the cost of neonatal care in a tertiary care level institution in northern India.
Methods
This prospective observational study was conducted over a period of 4 months at a 30-bedded level III neonatal unit in a tertiary care institute in north India. Data was collected from a self-written diaries by parents of all neonates admitted in the unit. The cost analysis included direct hospital cost and additional expenditure by families during entire hospital stay.
Results
A total of 135 newborns (86 males) were enrolled in this study. 60 babies required Neonatal intensive care unit (NICU) admission. The median total expenditure incurred in study cohort was US$172 (IQR 83.5–546.3); median duration of hospital stay was 7 (IQR 5–16) days. The total expenditure per day for babies with Neonatal intensive care unit stay was US$32.7 (IQR 23.5–48). The direct hospital charges amounted to approximately 3/4th of total expenditure, while rest 1/4th was additional cost incurred upon family.
Conclusion
The cost of care of a sick newborn in public sector hospital of India is substantial. Additional expenditure apart from direct cost of treatment contributes significantly to the financial burden.
Keywords
Background
Advances in the field of neonatal care have led to marked progress in the survival of premature and critically sick babies, albeit at a cost. Perinatal morbidity causes colossal undesirable impacts to both health outcomes and financial expenses. The financial burden resulting from poor neonatal outcomes begins at the time of delivery and often stretches into adulthood. Neonatal intensive care unit (NICU) stays are amongst the most expensive forms of hospitalizations. 1 There are proven actions that can be taken to significantly improve health outcomes and diminish the economic encumbrance for families. India contributes to 27% of neonatal deaths worldwide: 40% of low birthweight (LBW) babies and a quarter of preterm births.2-3 More than one-third of these deaths are due to premature births. There is huge variation in level of care and cost policies among hospitals; the costs also change due to inflation. Consequently, the role of economic estimations of healthcare interventions in NICU has become increasingly vital. There is limited information on the cost of NICU care, especially from developing countries like India.4–9 The study is an attempt to estimate the cost of neonatal care in a tertiary care-level institution in northern India.
Methodology
The study was a prospective study conducted over a period of 4 months (December 2020–March 2021) at a 30-bedded level III NICU in a tertiary care institute in Lucknow, India. The unit provides comprehensive care for critically sick neonates and is well equipped with incubators, open care systems, ventilators including high frequency ventilation, multipara monitors, phototherapy units, pulse oximeters, laminar flow system, and syringe infusion pumps. The unit admits both inborn and outborn babies and on an average 40–45 newborns per month from all the socioeconomic classes. A trained neonatologist supervises the services around the clock. The nurse/patient ratio varies from 1:2 to 1:4 depending upon the number of admissions. The study was approved by Institute’s ethics committee and a written informed consent was taken from parents.
All consecutive neonates admitted in NICU during the study period were enrolled. Parents unwilling for participation and neonates requiring with surgery were excluded. SNAPPE-II score was used for defining the sickness level at admission. The parents were given a diary for writing their daily expenses incurred during the entire hospital stay. The direct hospital expenses include charges for hospital bed, drugs, consumables, miscellaneous items, and towards various procedures and laboratory investigations used in the treatment of their newborn in hospital. Apart from direct hospital charges, additional cost incurred upon family in the form of stay, food for parents, items required for baby feeding, loss of pay of parents due to hospital stay were also calculated. The total cost was calculated in Indian Rupees (INR) and was converted to USD ($) using average price of USD ($) for the year 2021 as 1 USD ($) = 73.9 INR. 3 Hospital charges remained unchanged during the study period and the variations in the cost of drugs and consumables were marginal.
The hospital has a system of computerized Hospital Revolving Fund (HRF) wherein the surgical and medical items are provided to patients at a subsidized cost. The subsidization varies from 5% to 30% depending upon the utility rate of item. The items are divided into miscellaneous group that comprises frequently used items such as syringes, extension lines, cannula, plastic aprons, and feeding tubes. It is further classified depending upon level of use into low, medium, or high HRF and charged accordingly at an estimated price per day. The rest of the items are unit items where the items are charged only when used. The prices are fixed by the HRF committee and are available to patients in subsidized prices. The items not available in HRF are brought by parents at market price.
Data was analyzed using statistical package for the social sciences software version 21.0. Continuous data was expressed as median with interquartile range and categorical data was expressed as frequencies.
Results
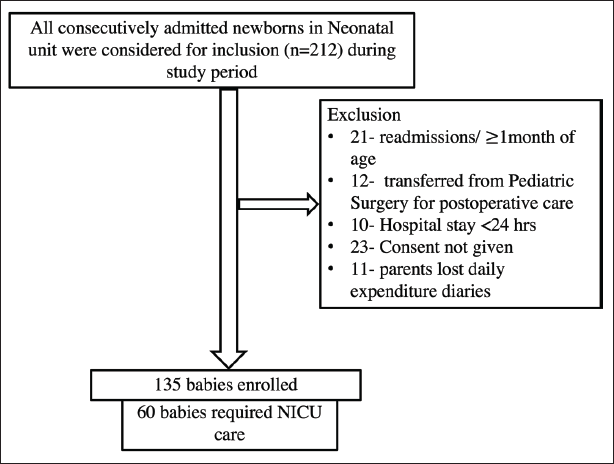
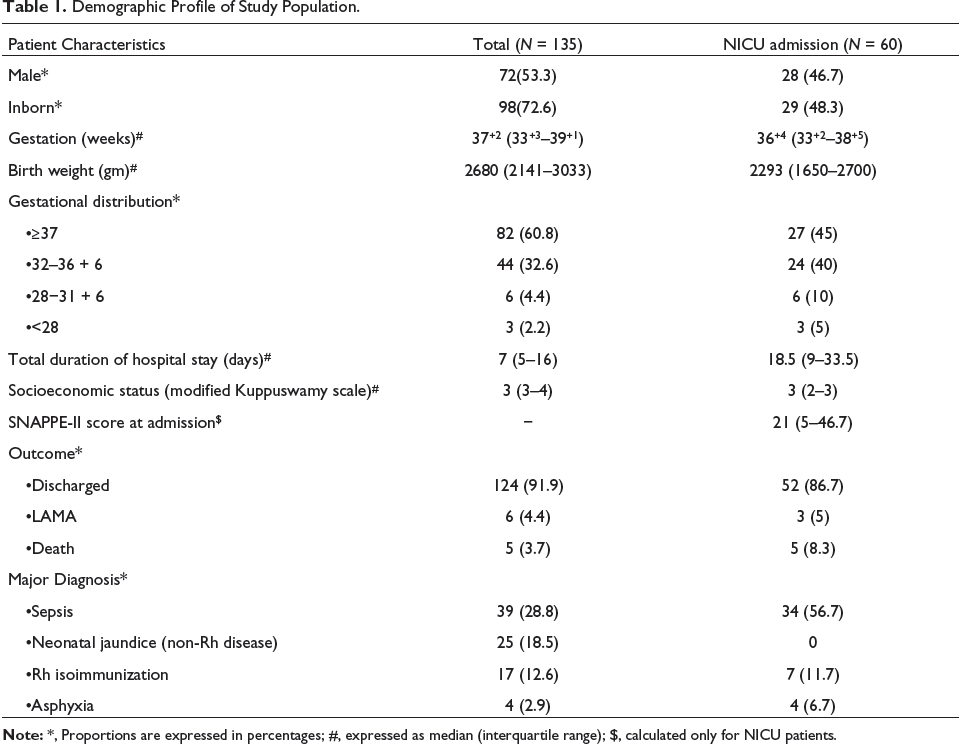
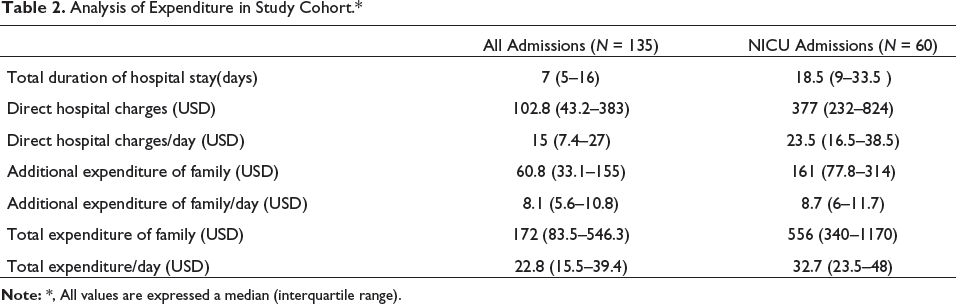
A total of 135 newborns (86 males) were enrolled in this study (Figure 1); a total of 60 babies required NICU stay of variable duration. The baseline demographic characteristics are as shown in Table 1. The median total expenditure incurred in study cohort was US$172 (IQR 83.5–546.3); median duration of hospital stay was 7 (IQR 5–16) days (Table 2). The total expenditure per day for babies with NICU stay was US$32.7 (IQR 23.5–48).
Flow Chart Showing Enrollment of Newborns.
Demographic Profile of Study Population.
Analysis of Expenditure in Study Cohort.*
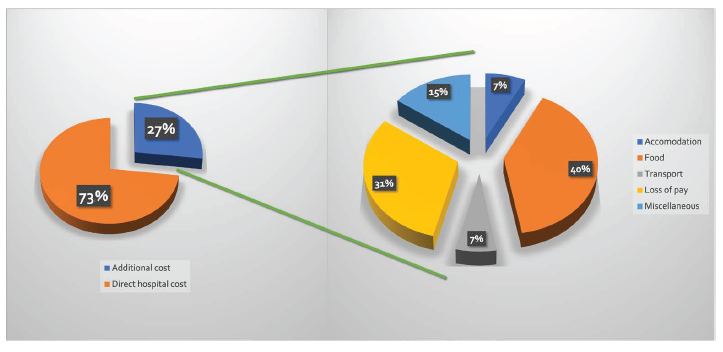
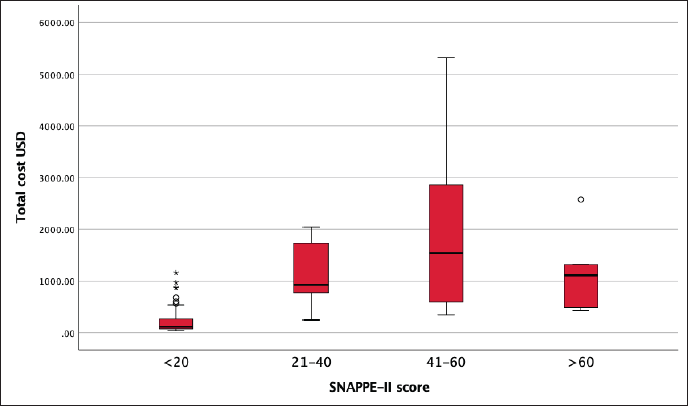
The direct hospital charges amounted to approximately 3/4th of total expenditure, while rest 1/4th was additional cost incurred upon family (Figure 2). Of the additional expenses, loss of pay and food outlays were the major contributor to the financial burden to the families. Median expenditure in outborn infants (n = 37) was US$842 (IQR 417–1171), while in inborn infants, (n = 98) it was US$113.4 (IQR 73–260). Maximum expenditure was observed in newborns with more severe illness with SNAPPE-II score between 40 and 60 (Figure 3).
Distribution of Expenditure in Study Cohort.
Expenditure According to Severity of Illness as Determined by SNAPPE-II Score.
Discussion
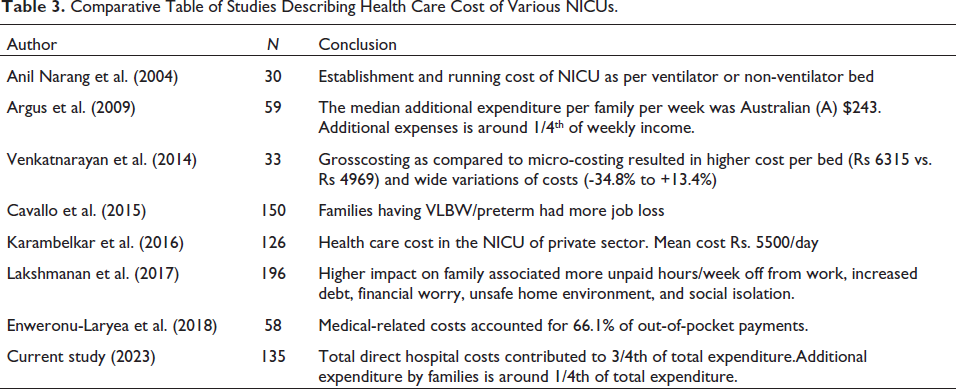
This study discusses about the cost analysis of a tertiary care NICU in a public sector academic Institute in India. There is scarcity of reported literature (Table 3) regarding estimation of fiscal valuation of NICU stay. Further, there are only a few recent studies on the evaluation of cost of stay in public and private sectors.10–16 Adjusting to cost of inflation over period of time, 17 the average cost of care per patient per day was estimated to be US$203 in Chandigarh (2003) 10 and US$157.2 in Delhi (2010) in public sector NICUs 11 and US$407 in a for-profit private sector NICU was US$ 272.4. 12 Different authors have used different models to estimate the cost of care, had varying sample size, used diverse inclusion criteria, and also gauged total running cost of NICU. The cost of treatment is expected to be varied (higher or lower) in different NICU (public/private sector) due to distinct input charges, quality of care offered, and policies of the organizations.
Comparative Table of Studies Describing Health Care Cost of Various NICUs.
In addition to the direct hospital costs, there remains an extra substantial drain on family, which is not reflected in hospital bills. Further, many families working especially in private sector lose the job while being in hospital for prolonged time. This contributes to the already strained economic situation. Most cost estimation studies does not include personal expenditure of patient attendees. This aspect is evaluated in this study and demonstrated that loss of pay contributed to almost 31.2% of additional expenditure that the families spent while in hospital.
The study found that as the severity of illness increased, the cost increased, which is expected; however, for the sickest baby, the costs were less as these babies succumbed to their illness early. Even though, the expenditure during NICU stay in this study is less when compared to previous studies, this fraction of expenditure may be differed due to various factors, but the study highlights the family personal expenditure that remained unaffected by the hospital settings.
Health care economics in developing and low-income countries is still largely based on out-of-pocket expenditures, and the privatization of advance mechanisms like insurance. In the absence of insurance, a sickness not only diminishes wellbeing unswervingly but also increases the risk of impoverishment due to high treatment expenditures. Out of India’s estimated population of 1.2 billion, almost 60% of people pay for medical treatment out of their own pockets and these account for an average increase in poverty by as much as 3.6% and 2.9% for rural and urban India, respectively. 18 NICU care of neonates being expensive adds to the cost burden, especially because of paucity of insurance plans and lack of knowledge amongst the users. 6 National Rural Health Mission in India has launched the Janani Shishu Suraksha Karyakram (JSSK) in 2011 that aims in financially supporting families in public sector hospitals.19, 20 This initiative has aptly led to greater use of the public health hospitals in India. Unfortunately, the execution has not become widespread so far. It is equally important to push policymakers to initiate programs and policies to extend health coverage to a larger number of individuals. The challenge in health coverage is to be able to find a way to cover the informal and unorganized sector workers and their dependents. While many schemes have been considered and launched, the success rates have been very low, and India remains one of the countries with least health coverage for those who need it the most. Family support services need to be incorporated into health policy as families incur significant additional expenses, highlighting the necessity for additional expenditure to be taken into consideration. This appeals for authorities to take action to create additional facilities of shelter, food, and social support system for parents of babies admitted to NICU.
This study adds to the meagre literature evaluating financial hardship of parents of hospitalized newborn babies. Also, the study addresses the indirect financial burden faced by families. Being a single center study, the results may not be representative of entire public sector in India. Further, there are very less number of VLBW and preterm <32 weeks in our study samples. The study did not calculate the unit’s establishment cost, the running cost, and healthcare worker salaries since the primary aim was to determine the economic burden faced by parents.
Conclusion
The cost of care of a sick newborn in public sector hospital in India is substantial. The major burden of financial bearings lies with the parents. Additional expenditure apart from direct cost of treatment contributes significantly to the burden.
Footnotes
What Is Already Known?
What This Study Adds?
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was conducted after obtaining permission from Institute Ethics Committee. A written informed consent was taken from parents of the newborns participating in the study.