
Abstract
Background
The World Health Organization (WHO) has set some standards of essential newborn care (ENC) with some activities, the implementation of which minimizes the incidence of neonatal morbidity and mortality. This study attempted to assess the practice of ENC services among nonpublic health-care facilities and determinants of adequate ENC practice in southeast Nigeria.
Methods
This was a cross-sectional descriptive study carried out in 4 of the largest cities in southeast Nigeria. The studied facilities were selected by purposive and convenient sampling method. Scores were assigned to the practice of ENC and computed based on standard validated criteria. Data analysis was done using Epi Info version 7.2 and statistical significance was set at P < .05.
Results
A total of 77 health facilities in the study area were surveyed. The mean annual birth rate in the surveyed health facilities was approximately 342.2. Majority (64.9%) of the health facilities efficiently executed 3 of the 8 ENC practices while only 27 (35.1%) facilities had good essential newborn practices score. The city where the health-care facilities were located influenced the practice of adequate ENC. A greater proportion of health facilities located in Abakaliki and Awka practiced adequate ENC compared to facilities in Enugu and Nnewi (P = .001).
Conclusion
ENC service is poor in nonpublic health-care facilities in southeast Nigeria. Training and retraining of health workers as well as provision of necessary incentives through government-private partnership may help ensure better implementation of ENC in order to reduce neonatal morbidity and mortality in southeast Nigeria.
Introduction
Essential Newborn Care (ENC) is care required for every newborn baby regardless of delivery location or birth weight and this care should be continued for at least the first 7 days after birth. 1 Following delivery, the transition from the fetus to neonate represents a series of dramatic physiologic changes. Those changes need skilled personnel interventions to ensure that they occur with the least possible problem. 2
To minimize problems newborns encounter after birth, the World Health Organization (WHO) recommended a standard of care that encompasses a series of 10 steps, which in turn has a set of activities. These recommended ENC includes dry and stimulate, evaluate breathing, cord care, keep the newborn warm, initiate breastfeeding in the first 1 hour of life, administer prophylactic antibiotics into eyes, administer vitamin K intramuscularly, place the newborn’s identification bands on the wrist and ankle, weigh the newborn when stable and warm, and record all observations of the baby. 3
The implementation of these care activities minimize the incidence of neonatal morbidity and mortality. 4 Even though there was a substantial decline in the global neonatal mortality rate (NMR) since 1990, high NMR is concentrated in Sub-Saharan Africa (40/1000) and South Asia (26.9/1000). 5 Nigeria is among the top 3e contributors to the global burden of infant mortality with a NMR that has stagnated between 37 and 41 per 1000 live births over the past 3 decades. 6 More than a million of these neonatal deaths occur on their first day of life, which would have been minimized with appropriate implementation of ENC.2, 4, 7–9
Even though each step of ENC is designed to be implemented based on prioritization of newborn problems and/or its impact on neonatal life, most studies from different parts of the world have indicated incomplete or inappropriate practice of ENC.10, 11
This study set out to assess the practice and the determinants of adequate ENC services provided to babies immediately after delivery in privately owned health facilities in southeast Nigeria.
Methodology
Study Area and Sampling Method
This was a cross-sectional descriptive study carried out in 4 cities in southeast Nigeria namely Enugu in Enugu State, Abakaliki in Ebonyi State, Awka and Nnewi both in Anambra State. The study is the second part of a multi-center survey conducted in these states. These study areas were selected due to the presence of a tertiary health institution within these localities which serves as referral center for private and faith-based health facilities. Selection of health-care facilities sampled was purposive and limited to only facilities that offered maternal and child health services. The selected health facilities were visited by at least one of the principal investigators and research assistants. During the visits, the purpose of study was explained and informed consent obtained from the head or director of all surveyed health facilities. Where consent was given, a questionnaire was administered to the director and/or their designates.
Measures
The study variables were collected into the relevant sections of the questionnaire. In the first section the characteristics and ownership structure of health-care facilities surveyed were obtained and categorized as follows: (a) professional qualification of health facility owners; specialist and general practitioner, (b) type of ownership; faith-based and private, (c) location of health facility; Enugu, Awka, Nnewi and Abakaliki, (d) annual birth rates of the facilities
The second section of the questionnaire collected information on the correct application of the ENC practices. Correct practices included: (a) cutting the cord between 1 and 3 minutes, (b) use of chlorhexidine for cord care, (c) administration of vitamin K1, (d) routine eye care with erythromycin, (e) skin to skin care within first 1 hour after delivery, (e) putting to breast within an hour after delivery, (f) bathing after 24 hours of delivery, and (g) no routine prescription of drugs after delivery. A scores of 0 and 1 was awarded respectively for incorrect and correct practices of each component of ENC. The maximum score obtainable was 8. The total scores were computed for each surveyed facility which were then categorized as 0 to 3 for poor and 4 to 8 for good ENC practices.
Data Collection and Analysis
Data collection was done using questionnaires administered by trained research assistants. Information were inputted into the relevant sections of the questionnaire and subsequently transferred into a Microsoft Excel Sheet. Data collected were categorized and reported in percentages and ratio. The chi-square test and independent sample t-test for non-normally distributed data (Kruskal-Wallis Test) was used to assess associations between the predictor and outcome variables. Data analysis was done using Epi Info version 7.2 and statistical significance was set at P < .05. Respondents with grossly missing information were excluded from the analysis.
Ethical Approval
Ethical approval for the study was obtained from the University of Nigeria Teaching Hospital (UNTH) Research and Ethics Committee. Additionally, permission to interview and inspect the newborn units of the surveyed health facilities was obtained from the owners of the hospitals and/or their designates.
Results
Characteristics of the Health Facilities Studied
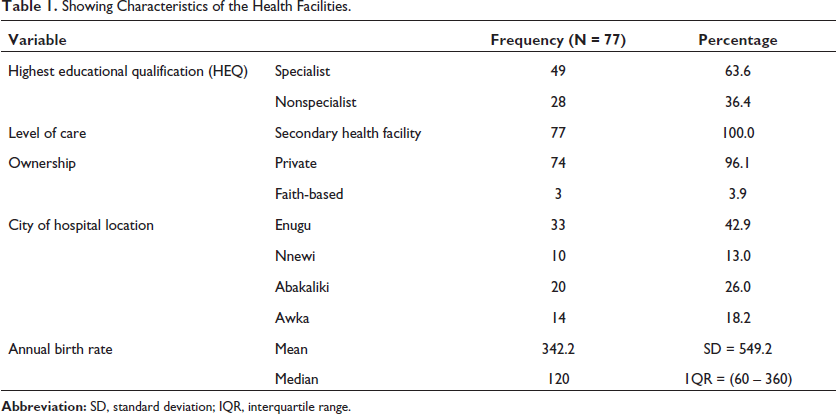
In all, a total of 77 health facilities were surveyed. About 4-in-10 of the health facilities surveyed were located in Enugu and the remainder located in Abakaliki (26%), Awka (18.2%), and Nnewi (13%). Most of the health facilities surveyed (96.1%) were privately owned while 3.9% were owned by faith-based organizations. The majority, 49 (63.6%), of the facilities surveyed were owned by specialists, while the rest were owned by nonspecialists. The mean birth rate of the health-care facilities enrolled in this study was 342.2 per year (Table 1).
Showing Characteristics of the Health Facilities.
Essential Newborn Care Practices in the Health Facilities
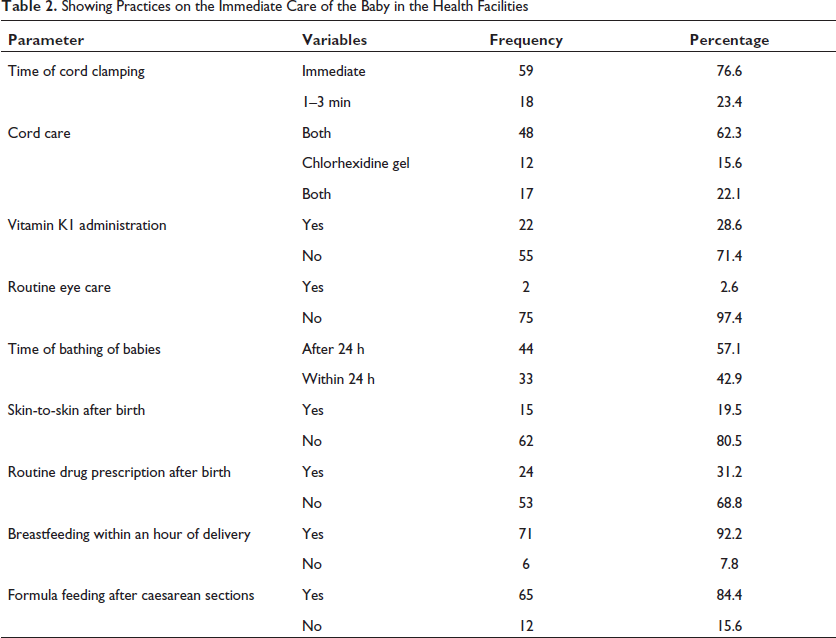
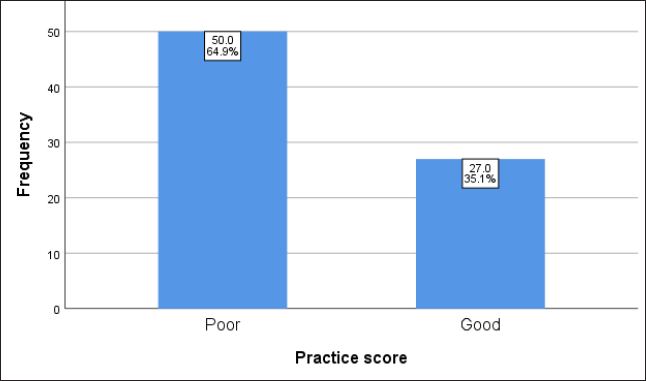
About a fifth of surveyed facilities (23.4%) practiced cord clamping between 1 and 3 minutes of childbirth, 15.6% used chlorhexidine for cord care, 28.6% administered vitamin K1, 2.6% practiced routine eye care with erythromycin while practice of skin-to-skin care within first 1 hour after delivery was done in 19.5% of surveyed facilities. Most of the surveyed facility (92.0%) practiced putting newborn to mother’s breast within 1 hour following delivery, 57.1% practiced bathing after 24 h of delivery and over half of surveyed facilities (68.8%) engaged in “no routine prescription of drugs” after delivery. In summary, it was observed that over two-thirds of surveyed health care facilities, (64.9%) had poor ENC practice score (0–3) while the remaining 27 (35.1%) facilities had good ENC practice score of (4–8) (Table 2 and Figure 1).
Showing Practices on the Immediate Care of the Baby in the Health Facilities
Bar Chart Showing Practice Score on the Immediate Care of Babies in Health Facilities.
Predictors of Good Practices of Essential Newborn Care Among Surveyed Facilities
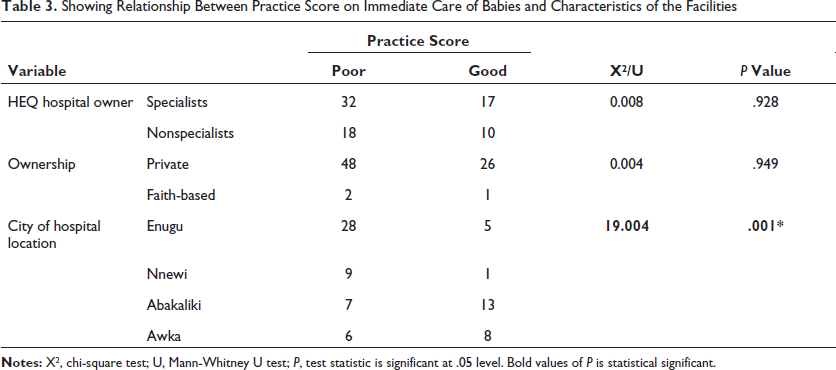
The relationship between good ENC practice score and characteristics of each health facility surveyed was assessed and it was noted that only the city where the health-care facility was located showed a significant association with good practice of ENC. More health facilities located in Abakaliki and Awka had good practice score of ENC compared to facilities in Enugu and Nnewi (P = .001) (Table 3).
Showing Relationship Between Practice Score on Immediate Care of Babies and Characteristics of the Facilities
Discussion
This study set out to explore the practice of ENC and its determinants among health-care facilities in southeast Nigeria.
Our study noted that approximately two-thirds of facilities surveyed did not implement adequate ENC necessary for optimal survival of newborns in its facilities. This finding was corroborated by a similar cross-sectional study conducted to assess quality of newborn care immediately after birth in 643 health facilities across six sub-Saharan African countries. In all countries assessed, it was observed that inadequacies existed in ENC services with causes ranging from poor health worker knowledge, poor performance in key routine newborn care practices to lack of equipment needed to provide these essential newborn services. 12 These observations in Africa are unfortunate especially when compared to another study conducted in 226 public health facilities in Afghanistan which showed a higher proportion of babies received ENC. 13 In the study, it was noted that close to 90% of babies delivered at health-care facilities were dried immediately and 89.7% had sterile cutting of umbilical cords. Other ENC practices noted in the study included skin-to-skin contact (49.2%), airway clearing and/or stimulation (72.5%), and prompt resuscitation with a bag and mask (72.5%). 13 Even though the Afghanistan study was conducted exclusively in public health-care facilities compared to only private/faith-based ones in our study, it does demonstrate that practice of ENC services can be achieved in resource-limited setting with proper planning and motivation on the part of health-care leaders. The WHO in its 2017 press release noted that to prevent or significantly reduce the 5.1 million babies that die within the first month of their life, political and health-care leaders must be committed to universal health coverage and essential newborn health services which are critical to life saving newborn interventions. 3
It was also noted in this study that more than two-thirds of the surveyed health facilities correctly implemented only 3 of the 8 ENC practices. Toma et al 14 and Amsalu et al 15 also documented poor practice scores in Jos Nigeria and conflicted affected areas of Somalia. Yosef et al 16 and Ayenew et al17–19 on the contrary reported high practice scores in Ethiopia which was attributed to the availability of frequent on-the-job trainings as observed in a study in Southwest Ethiopia. The practice of intramuscular Vitamin K1 and routine eye care at birth were poor in our study, a finding corroborated by Toma et al 14 in Jos Nigeria. The reason for this is unknown but reinforces the need for training and retraining to emphasize the importance of the implementation of all aspects of ENC services.
Finally, our study noted that only the city where health facilities were located significantly predicted good practice score for ENC with Abakiliki showing the strongest association. The reason for this finding is not immediately clear but we believe that the difference in good practice score of newborn care in the surveyed communities may be influenced by the sociodemographic characteristics of its residents. Awka and Abakiliki are well known to have higher proportion of civil servants who are relatively more educated and may have better understanding of the concept of ENC compared to residents in Nnewi who are predominantly traders. This understanding could significantly influence the quality of newborn services provided by health-care facilities in these localities.
Similarly, the good practice of ENC in Abakiliki may also be related to the Maternal and Child Survival program (MCSP) which was conducted in Ebonyi and Kogi by the USAID in 2018. 20 The program focused on strengthening newborn care, training, and enlightenment of health-care providers on adaptation and development of newborn training materials, operational guidelines and provided support to the states for health planning to ensure sustainability of MCSP activities. 20 This lends credence to the WHO call for continuous public enlightenment campaign and robust funding together with frequent retraining of health-care workers in ENC practices. This is where government support and regulations in individual countries play a decisive role.
Conclusion
Our study showed that essential newborn services is poor in nonpublic funded health-care facilities in southeast Nigeria. This calls for concerted efforts through government-private partnership for the provision of necessary incentives to nonpublic funded health facilities to improve service readiness and provision of timely training and retraining for health-care staff in these facilities.
Footnotes
Ethical Approval
The study was approved by the University of Nigeria Teaching Hospital (UNTH Research and Ethical Committee.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.