
Abstract
Introduction:
Clinical conditions of pre-adolescent age are of immense importance to be identified and treated, as it poses a high risk of developing some maladaptive personality pattern or mental and physical health problems in adulthood. Dialectical behavior therapy for children (DBT-C) targets emotional and behavioral dysregulation in pre-adolescent groups by presenting and packaging information into developmental and cognitive levels of children. Although DBT is not very commonly used with children, the present study aimed at understanding the role and efficacy of DBT-C in a nine-year-old child diagnosed with socialized conduct disorder (CD).
Material and Methods:
This study presented the execution of DBT-C on a nine-year-old male, Bengali speaking, hailing from an urban nuclear family with a diagnosis of socialized CD with prominent symptoms of behavioral problems, such as frequent anger outbursts, lying, playing with fire, running away from home, along with the presence of impulsivity, self-harming behavior, feelings of abandonment, and difficulties in interpersonal relationships. The DBT-C targets children’s presenting problems, parent-child relationship, and decreases the risk of psychopathology in the future. Thus, the present case study aimed at reducing these behaviors using the DBT-C approach in a 10-session therapy plan to bring an overall well-being of the child.
Results:
After 10 sessions of DBT-C, qualitative analysis showed that there were reduced anger outbursts and self-harming thoughts. Also, there was improved self-control and interpersonal relationships, especially with parents. Quantitative analysis showed reduced scores on the Devereux Scales of Mental Disorders (DSMD) post-intervention.
Discussion:
Childhood psychiatric disorders such as oppositional defiant disorder (ODD) or CD may predict borderline personality disorder (BPD) in adulthood, particularly for boys. The present study showed the efficacy of DBT-C on a pre-adolescent child with CD along with emerging borderline personality traits.
Keywords
Introduction
Dialectical behavior therapy (DBT) has been an evidence-based therapy for adults with borderline personality disorder (BPD). Dialectical behavior therapy for children (DBT-C) has been modified for adolescents for the pre-adolescent age group of 6-13 years. This is because the clinical conditions of pre- age warrant early identification and treatment, as there is a high risk of developing some maladaptive personality patterns or mental 1 and physical health issues in adulthood. Also, adolescents who are unable to manage their emotional states during their developmental period experience a higher risk of developing mental health problems in adulthood. 2 DBT-C is developed for children who have emotional dysregulation and corresponding behavioral dyscontrol. It retains the theoretical principles and therapeutic strategies of DBT. 3 Nearly all of the adult DBT skills and procedures are incorporated into DBT-C, which also includes a parent education component and adapts it to the developmental and cognitive level of the children. A major shift from the standard DBT is the treatment target hierarchy, which puts increased importance on adaptive patterns of parental responding, which is important to improve the child’s emotional and behavioral dysregulation.
DBT in adults has shown that the treatment targets the hyperactivity part of the disturbed neural circuitry underlying emotional dysregulation in BPD. 4 Studies toward the progress of adapting DBT for preadolescent children have shown that parental attitude indicates the overall acceptance of the intervention, and thus, the parental training curriculum is included as an important component of DBT-C. A randomized control trial of 43 children with disruptive mood dysregulation disorder showed that DBT-C led to improvements in behavior outbursts and angry/ irritable mood. Also, the improvements were maintained at the three-month follow-up. 5 Another randomized control trial of 47 children with severe emotional and behavioral dysregulation showed that children in DBT-C had significantly greater reduction in symptoms on both internalizing and externalizing subscales as compared to children in treatment as usual (TAU). 5 Additionally, it has been seen that adolescents with behavioral issues view their involvement in DBT skills training groups favorably and place a strong emphasis on reflective practice. 6 One of the largest randomized controlled trials on treatment of adolescents for severe emotional dysregulation, including suicidal behavior, non-suicidal self-injury, and deliberate self-harm, showed that DBT with supportive individual and group therapy was efficacious in reducing emotional dysregulation and, in turn, self-harming behaviors. 7
DBT has its partial roots in eastern cultures, but it has not been widely implemented, tested, and applied in low- and middle-income countries compared with Western settings. 8 Very few studies have indicated the feasibility and efficacy of DBT-C in pre-adolescents in multiple settings. Thus, an established intervention for this age group is the need of the hour. Since DBT in adults and adolescents is found to be an empirically supported intervention for suicidal and self-injurious cases, more research is required to determine the efficacy of DBT-C for suicidal and self-injurious behavior in children. The present study aimed at understanding the role and efficacy of DBT-C in a nine-year-old child diagnosed with socialized conduct disorder (CD). The main objective was to understand the efficacy of DBT-C in a child who was diagnosed with socialized CD along with emerging borderline personality traits.
Materials and Methods
Case Details
Index child, a nine years old boy, studying in Class II, hailing from an urban background, low socio-economic status family, was brought in a mental health center with complaints of disobeying others, stubbornness, use of abusive languages, tendency to play with fire, running away from home, lying frequently, stealing money for smoking, and frequent involvement in physical fights for one year along with self-harming behavior for 4-5 months.
On further probing, it was revealed that in 2019, the client’s parents admitted him to a child care home due to a financial crisis. The client’s parents reported that the environment of the child care home was uncongenial, so they withdrew him from there. A few days after returning to his house, the parents reported that they started observing that he became extremely defiant, started playing with fire, and burned papers. He had poor academic performance. He was unwilling to study and complete his homework. He would disturb other children during class and would also talk in between classes. He had a peer group in the mental health center and also in his house locality, but he would have frequent fights and arguments with them. He would lose his temper whenever his friends refused to act according to his wishes or did not listen to his demands. Following this, he would use abusive language and exhibit his aggression by physically harming his peers. He often engaged in big talks, especially with friends, and would also try to dominate them. He would also engage in plays mostly related to fighting or other games, such as football or cricket, in the center, but he was unable to sustain a game or play time, as he would engage in fights mid-play whenever things went out of his way.
The child’s parents also reported that he had a tendency to blame others for his own mistakes. He used to ask for toys frequently, and when buying, he would immediately break them. He used to go away from home without informing them. His parents also reported that he was restless since early childhood. He would not sit in one place for the required time. The child had subsequently improved with medication.
For the last 4-5 months, the child had started engaging in self-harming behavior by slashing his arms and wrists, especially after arguments with his parents. The child also reported that his parents did not give him time, and they did not love him. The child expressed feeling abandoned after admission to the child care home. The child and the caregiver at the mental health center reported that he was abused by his mother both verbally and physically.
Based on the history and the assessment, the child was diagnosed with socialized CD. No history was suggestive of autism spectrum disorder, specific learning disability, mood disorders, anxiety disorders, separation anxiety disorder, psychotic symptoms, substance abuse disorder, head injury, epilepsy, or any sensory deficits. Verbal informed consent was taken from the parents of the child, and they were cooperative during the therapeutic sessions.
Psychotherapeutic Formulation
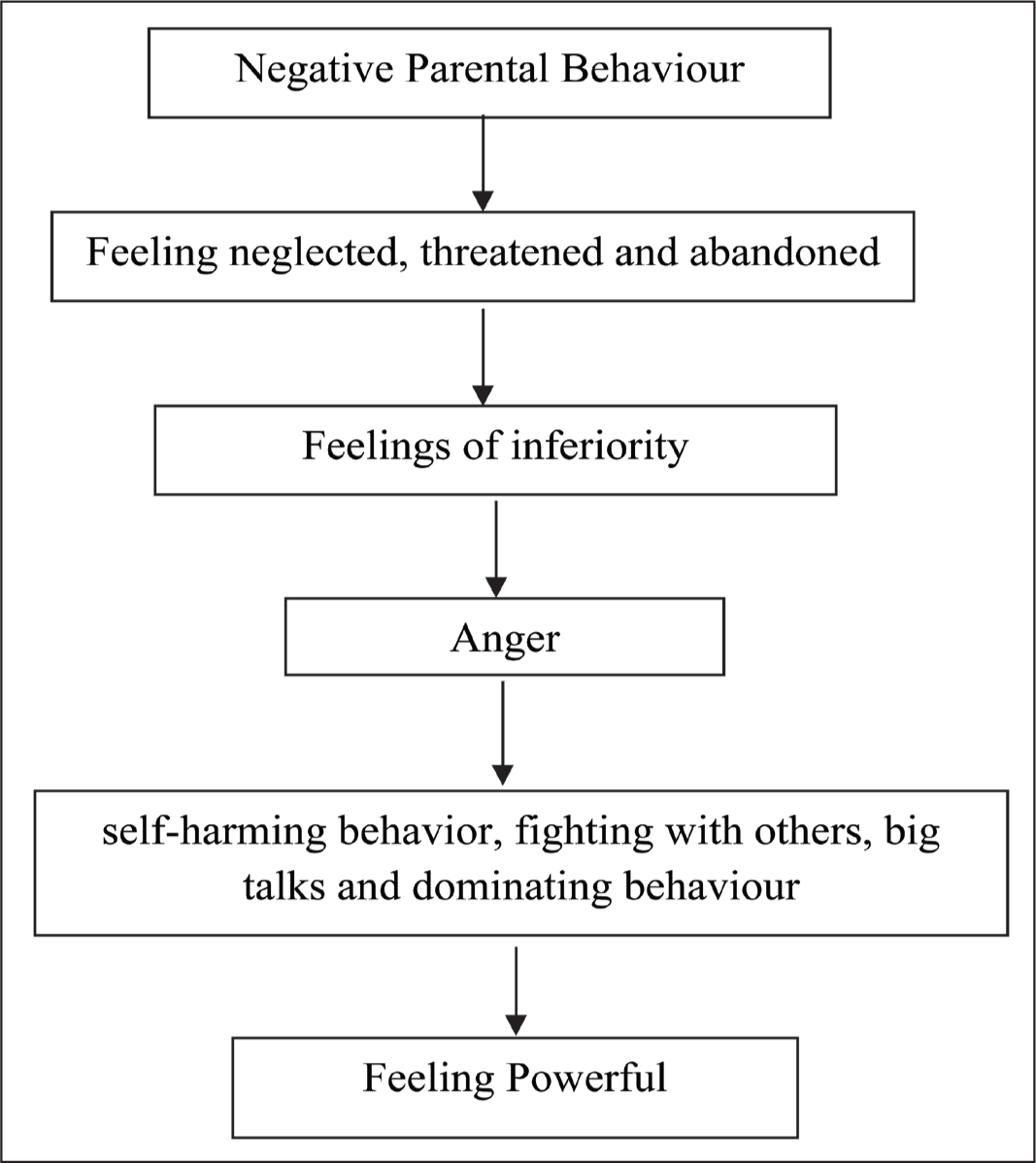
The child came with severe behavioral problems; however, a detailed history suggested the parents’ behavior played an important part in developing his psychopathology. According to the child and the caregiver at the mental health center, he was verbally and physically abused by his mother from an early age. His father was emotionally distant. Even though the child was more bonded to his mother, he also felt threatened by her actions and abandoned when he was separated from his family for a prolonged period of time. Also, when the child used to visit home, he was being neglected by his parents. Due to this, the child developed beliefs such as “I am unloved, I am inadequate,” which he manifests as anger outbursts and bossy behavior due to feelings of inadequacy. He became defiant and impulsive. After arguments with parents, he used to engage in self-harming behaviors to compensate for the feelings of being dominated and powerless. As the child was bullied in his earlier child care home, he may have developed feelings of inferiority and helplessness, which have led to his bossy behavior and big talk. Assessing the significant events in the patient’s history with his clinical presentation, it is understandable that the problems started from an invalidating family environment, along with feelings of abandonment and inferiority, and his subsequent efforts to overcome these feelings. The psychotherapeutic formulation of the case has been shown in Figure 1.
Psychotherapeutic Formulation.
Therapeutic Sessions
The child underwent 10 tailor-made DBT-C sessions, each lasting 45 minutes, at a mental health care center in Kolkata, West Bengal.
Mode of Therapy
Dialectical Behavioral Therapy for pre-adolescent children (DBT-C)
The Devereux Scales of Mental Disorders (DSMD) were administered to assess pre- and post-intervention outcomes. DSMD, developed by Naglieri, LeBuffe, and Pfeiffer in 1994, 9 is used to assess the global pathology in children and adolescents, and it can be administered to children (5–12 years of age) and adolescents (13–18 years of age). For the present case, the child version with 110 items was used. It includes six subscales, namely, the conduct and attention scales, which compose the externalizing composite; the depression and anxiety subscales, which comprise the internalizing composite; and the autism and acute problems scale, which composes the critical pathology scale. The DSMD scoring is a very useful method, as through this the clinician can compare the same child’s scores obtained on DSMD at different points in time during an ongoing treatment, 10 as done in the present case. The internal consistency coefficients for the DSMD total score were 0.98 for age and gender, respectively, and 0.97 for parent raters and 0.98 for teacher raters. The median reliability coefficients for the externalizing and internalizing composites and the critical pathology scale were 0.97, 0.94, and 0.90, respectively, for the child version. It also has good validity in the sense that it has the ability to differentiate between inpatient children diagnosed with attention deficit hyperactivity disorder (ADHD) and CD, and it also has high specificity and predictive power when evaluating children with emotional disturbances. 10
Psychotherapy Process
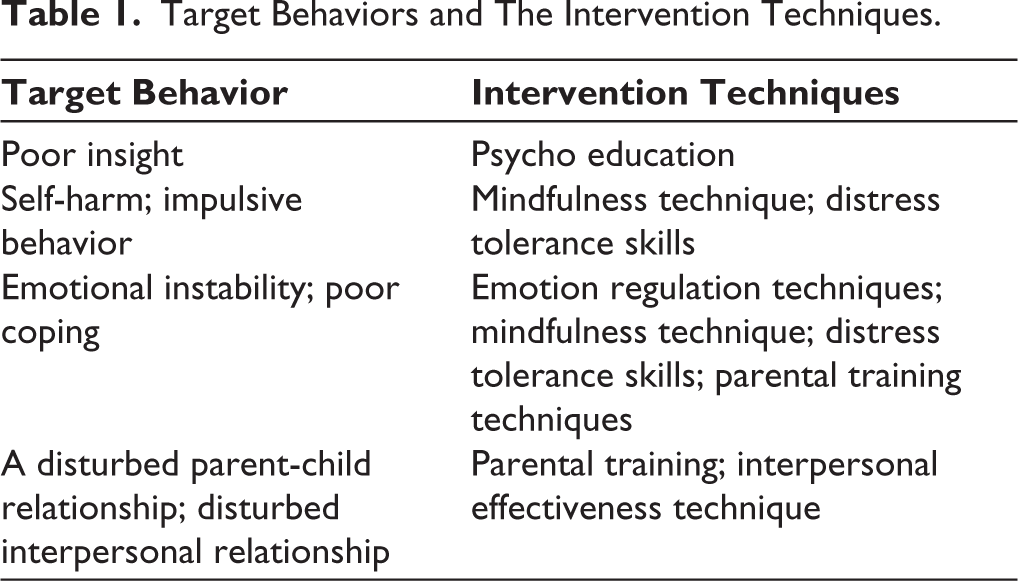
The target behaviors and the Intervention techniques have been shown in Table 1.
Target Behaviors and The Intervention Techniques.
Psycho Education
Psycho education was used to enhance the insight of the child and his family. At the beginning of the session, the ethics and confidentiality were explained to the parents and the child. Both the child and his parents were psycho educated about the problem behaviors and the family dynamics, reinforcing his pathology. The parents were helped in identifying the life-threatening and therapy-destroying behaviors of the child. Techniques such as planned ignoring were used to address therapy-destroying behavior, and the behavior was also treated as informative in the session. The parents’ participation in the therapy process and learning the techniques of the therapy was emphasized for addressing parental emotional dysregulation and improving the child’s problems.
Behavior Chain Analysis
The child and his parents were explained about the behavior chain analysis and how it will help him to identify the problems. The behavior chain analysis included the components, triggers, behavior, thoughts, feelings, and consequences.
Mindfulness
The mindfulness technique was used to target emotion dysregulation. It was reported by the parents that the child always tends to blame others for his problems and focuses on others’ negative behaviors. Thus, mindfulness would help him to observe the situation without any judgment. The concept of mindfulness was explained to the parents, while the child was introduced to the concept through concrete examples and hypothetical scenarios. The bubble challenge was used as a mindfulness technique. Here, the bubbles were blown in the air, and the child was asked to just observe the bubbles without trying to catch or hold them. Through this, the child was taught to observe one mindfully and non-judgmentally.
Another technique used was wrong play, where the child was given different situations with negative behavior, and the child was to identify the ineffective behavior and mention the alternative. For example, the child was given a situation: “Suppose your friend took your favorite toy without informing you and broke it. When you got to know, you started arguing with him and got angry and had a fight.” To this, the client could identify the problem as being angry, and the alternative he mentioned was to talk to him about why he did not inform him.
Emotion Regulation Techniques
The child and his parents both were given an understanding of emotions. A picture of a feeling thermometer was shown to the child, which assisted him in recognizing and quantifying his emotions about an issue. It was also used with the parents. The child was also introduced to different facial expressions to help him identify appropriate emotions. Another technique used was the opposite action, where the child was asked to act opposite to the emotion he was feeling to change the affective reaction. It was practiced in the session through role plays.
Distress Tolerance Skills
To reduce impulsivity, anger outbursts, self-harming behavior, and emotion dysregulation, distress tolerance techniques were used, which also helped to improve self-control. First, the child was explained about distress tolerance skills in the presence of his parents. Then, the child’s thoughts, such as “why it happened” or “why is it me” about a situation, were addressed by providing examples of age-appropriate real events, and he was further taught to “let it go” by accepting and understanding the current scenario.
Another distress tolerance skill that was used is STOP (S = Stop, T = Take a step back, O = Observe and P = Proceed mindfully). This was aimed at increasing awareness of his negative behavior and decreasing impulsivity. His impulsive behavior was listed and explained through a worksheet and practiced by role play in different contexts. Similar tasks were given as homework assignments, and participants were asked to note down their reactions to the situations.
Interpersonal Effectiveness Techniques
The parent training skills were used, and another technique called FRIEND (F-Be fair, R-Respect the other person, I-Act interested, E-Easy manner, N-Negotiate, D-Be direct) was also used. It helped the client to get along with others. The technique was explained, discussed, and practiced in the session.
F-Be fair, R-Respect the other person, I-Act interested, E-Easy manner, N-Negotiate, D-Be direct.
Parental Training Techniques
In DBT-C, whether an incident was effectively resolved is evaluated primarily by the environmental response. Parental behaviors can help ameliorate the child’s emotional dysregulation. The techniques involved are
Creating a Validating Environment
The parents were explained about validating and invalidating environments, the invalidating behaviors they engage in, and relating the child’s problems with the concept of validation. It was found during interaction that the child enjoyed drawing, but his parents never acknowledged his potential and always tended to ignore. Parents were told to acknowledge his positive behavior to validate the environment.
Introduction to Behavior Change
Different behavior change techniques were discussed with his parents, such as reinforcement, punishment, extinction, shaping, and how to give effective prompts. Their behavior change techniques were identified in the session, and they were informed about the positive impact of reinforcement and the negative effects of punishment. They were also informed that, rather than using positive punishment, they can use other techniques such as time out, taking away privileges, according to the demands of the situation. The child’s mother was asked to practice the techniques using role play with hypothetical and real situations in the sessions.
A-VCR Model
This model incorporated all the points by putting them together: Assess/attend, validate, coach skills use, and reinforce. To improve the parent-child relationship, the parents were informed about the concepts of punishment and retaliation. Retaliation, such as screaming, yelling, and inflicting pain, was often used by them as a way to respond to their problems. Thus, due to frequent mutual retaliation, it increased the pattern of invalidation and decreased the child’s willingness to engage in adaptive behaviors. His parents demonstrated the skills they can use in different problem situations. Role plays were done in sessions. They were asked to practice these skills either in an actual problematic situation or after an outburst has occurred, and they can use alternative solutions. They were also asked to plan for different skills to tackle different situations likely to happen in the near future.
To improve his relationship with parents and peers, this technique was implemented, where he was trained to follow the steps, and a worksheet was also provided to help him understand the steps.
Results
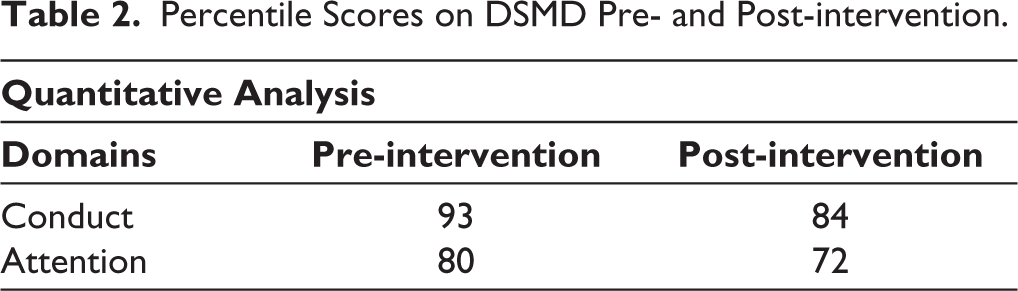
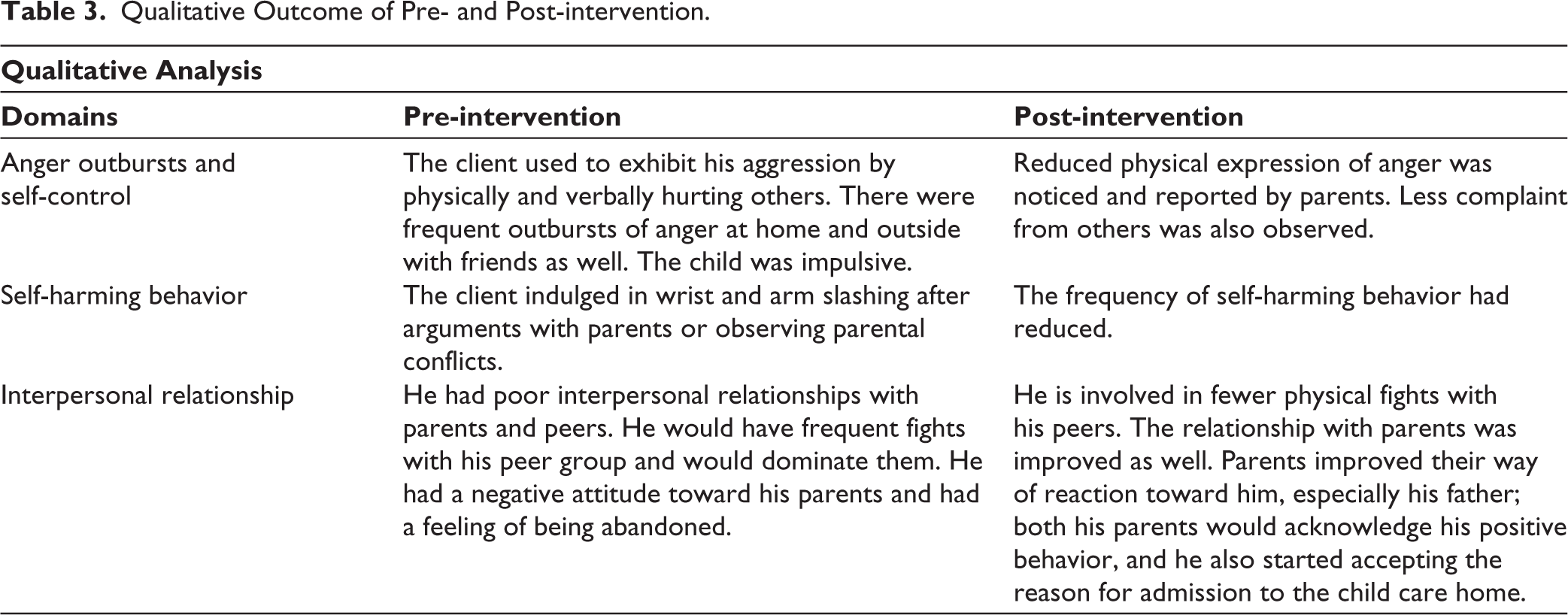
After 10-sessions of therapy, post-intervention quantitative analysis based on scores on DSMD indicated significant improvement in his behavior as shown in Table 2. Qualitative analysis based on parents’ reports and behavioral observation showed an overall improvement in his behavior as shown in Table 3. There was an anger outburst, self-harming thoughts, and improved self-control of the child. Compared to the pre-intervention phase, there was a significant decrease in the negative behavior of the parents and an increase in their approachability, which also served to strengthen the child’s interpersonal relationship with them.
Percentile Scores on DSMD Pre- and Post-intervention.
Qualitative Outcome of Pre- and Post-intervention.
Discussion
After 10 sessions, the case described above resulted in a positive outcome, as it can be seen that there was a reduction in the target symptoms, indicating the efficacy of DBT-C. DBT is an empirically supported intervention for adults with BPD, and it has also been adapted for suicidal and self-injurious adolescents. 11 However, DBT for pre-adolescent children is still in its budding stage. Children may not be able to express their concerns, and thus understanding the child’s emotions, important relationships, family, and neighborhood is important. Also, in countries such as India, the focus of therapy should be on short-term goals compared to long-term goals to avoid dropouts. 12 Thus, in Indian children, effective therapy must take into consideration the familial, cultural, and compatibility perspectives. Very limited studies have shown the efficacy of DBT-C in Indian children, and thus, this study is one of the stepping stones toward establishing the effectiveness of DBT-C.
Earlier studies have shown that the dropout rates in DBT-C were significantly lower than those in TAU. 13 Also, considering that DBT-C interventions have strong treatment demands, the low dropout and high patient satisfaction rates are noteworthy. It has also been seen that the response rates of children who responded well to DBT-C were substantially higher than those who responded favorably to TAU. For DBT efficacy studies, the high positive response rate of 90.4% is not an uncommon outcome. 14 Additionally, another research found that DBT-C improved outcomes without requiring the commencement of new psychiatric drugs; only children who were already taking psychiatric drugs at baseline continued to receive psychopharmacologic treatment. 15 Thus, literature suggests that DBT-C is effective and has a positive treatment outcome.
In the present case study, the child was diagnosed with socialized CD. The child also exhibited some borderline personality traits. Very few studies have shown the prediction of BPD in adulthood from psychiatric disorders in childhood. However, one of the studies indicated that ADHD and oppositional defiant disorder (ODD) predicted BPD symptoms in adulthood, and the oppositional behavioral dimension of ODD was particularly predictive of BPD. 16 Studies have also shown that DBT is efficacious in reducing anger control and improving emotion regulation in bullied children. 17 Due to the parallels between CD and BPD, which include emotional dysregulation, interpersonal relationship issues, and a poorer reaction to stress, DBT was chosen as the therapeutic modality for the present case. Thus, DBT-C was particularly used for the depletion of the target symptoms, such as anger outbursts, impulsivity, self-harming behavior, emotional dysregulation, and also to reduce future chances of development of BPD traits in the child in adulthood.
Parent training has been observed to be one of the most successful therapies for ODD. 18 However, it has also been observed that depending only on parent education and other forms of family engagement is challenging to execute because many caregivers are frequently reluctant to take part and attend clinics on a regular basis as a form of home management. Thus, DBT-C emphasized not just training and parental participation but also the child’s own transformation. 19 The DBT-C model also presumes the development of a validating and change-ready environment as the main therapeutic ingredient. 20 Therefore, parent training in conjunction with other modalities of DBT-C led to a significant decrease in the negative behavior of the parents and an increase in their approachability, which also strengthened the child’s interpersonal relationship with them.
Modifying the standard DBT techniques required taking into account the child’s developmental conditions. In the present study, DBT-C involved using more pictorial worksheets, such as the feeling thermometer or the STOP sheet. Using colors, bubble challenge, pictures, and repeated role plays were very helpful in the delivery of the various techniques and engaging the child to perform or involve into different tasks. Also, explaining the thought, emotion, and behavior triad with the help of examples and pictorial presentations of situations and dialogues was helpful in understanding the connection and carrying out the behavior chain analysis. In one of the studies, it was seen that modifying the cognitive behavior therapy (CBT) technique for children included using an acronym and metaphor, along with pictorial representation, for a better understanding of the child. 21 Also, parental adaptive patterns of responding may create a validating environment over time, which may in turn help in reducing the child’s emotional and behavioral dysregulation. 22 In the present case study, the intervention started with the parental training curriculum, followed by DBT skills for optimal recovery. Thus, this study showed that DBT-C is effective in reducing symptoms of socialized CD along with emerging borderline traits.
However, in the formulation and execution of therapeutic intervention, a few points were focused upon. The child had restlessness and temper tantrums since childhood. Thus, therapy-interfering behaviors were initially identified and focused on before initiating DBT-C modules. There was a family history of alcohol use, which was also taken into consideration during the case formulation. Also, there were some challenges faced during the therapy process. The first and foremost challenge was to build a rapport with the child. Although the child was interactive, establishing a rapport so that the child would comply with the therapy session was necessary. Second, the child was from a low socio-economic background, and both his parents were working. Thus, parental involvement in therapy sessions was limited. Only one of the parents could be involved in the therapy, and the parental training module was done in 4–5 sessions. Also, there was a family discord and an unhealthy family environment, which involved the use of abusive language and arguments. Thus, in case formulation, the family history, psychological factors of the child, and social factors were all taken into account. The parents were also referred for a couple of counseling sessions for managing their conflict. Despite these limitations, DBT-C was found to be effective for the present case study.
Thus, working with a nine-year-old child using DBT-C highlighted the importance of developmentally adapting the core therapeutic techniques to suit the child’s cognitive, behavioral, and emotional abilities. The therapist reflected on the need for creative, play-based techniques and using simplified language to introduce different techniques and skills, such as emotion regulation and mindfulness, so that it was both engaging and accessible. Additionally, the process underscored the importance of involving caregivers consistently to reinforce skills outside the therapy sessions. This case deepened the understanding that while DBT is originally designed for adolescents and adults, with careful modification and reflective practice, it can be an effective framework for younger children as well.
It can be concluded that DBT-C is effective in reducing problem behaviors associated with CD, such as anger outbursts, involvement in physical fights, along with emerging borderline personality traits such as self-harming behavior and disturbed interpersonal relationships. Thus, early identification and intervention of pre-adolescent psychological problems may reduce the risk of future development of maladaptive personality patterns. Since few studies have shown the effectiveness of DBT-C, the present study clarifies the efficacy of DBT-C in clinical settings and plans the therapeutic package for pre-adolescent children with both CD and emerging personality disorder. However, future studies must also focus on understanding the efficacy of DBT-C in other disorders as well.
Footnotes
Acknowledgements
The completion of this research would not have been possible without the support and guidance of many people. So, we would like to express our gratitude to all those people who have helped us in the completion of the work. We would like to thank our institution for giving us the opportunity to work in the department and supporting us throughout the journey. We are also grateful to our family members for their continued love and support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Verbal informed assent and consent were obtained from the patient and his parents, respectively. The ethical approval was obtained from the ethical committee of the Amity University, Kolkata with the approval number DRC-AIPSK/ETHICS/A95210919001/22 dated October 16, 2020. Verbal informed assent and consent were obtained from the patient and his parents, respectively. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.