
Abstract
Purpose of the Review:
Early menarche is recognised as a major apprehension, with associated psychosocial issues among girls and increased anxiety in parents. Although much has been presented on the biomedical aspects of such conditions, there is a lack of understanding about parental concerns, lived experiences, and attitudes in various sociocultural settings. The purpose of the proposed scoping review is to synthesise available evidence regarding parental concerns, attitudes, and experiences associated with early puberty and menarche in girls with a specific focus on psychological, cultural, and social determinants.
Collection and Analysis of Data:
The review followed a PRISMA-ScR framework and the Arksey and O’Malley framework, which was further developed by Levac et al. It undertook a detailed systematic search in PubMed, Scopus, ProQuest, and EBSCOhost, along with citation tracking. Peer-reviewed articles on the parental views on early puberty or menarche published between 2010 and 2025 were considered. Starting with 1,446 unique records, 22 studies were included according to the inclusion criteria. A standardised charting form was used to extract the data, which were subsequently thematically synthesised. The findings showed that in several settings, such as South Korea, Japan, Turkey, the United Arab Emirates, the United States, sub-Saharan Africa, Bangladesh, Ghana, and Indigenous North America, parents always reported high levels of anxiety, reliance on inaccurate information, stigma around menarche, and a strong demand for both medical and psychosocial interventions.
Conclusions:
Parental anxiety about early menarche is multidimensional and influenced by psychological distress, cultural traditions, lack of education, and healthcare services. These results demonstrate the relevance of interventions that are inclusive, culturally sensitive, and parent-centred to help the families in this developmental transition.
Introduction
Menarche, or the first menstrual period, is an important developmental milestone in the life of a girl child, as it marks the transition from childhood to adolescence. Although the average age of menarche is found to vary among different populations, an upward trend has steadily been observed regarding an earlier onset of menarche over the past decades, with serious implications for physical, psychological, and social health.1,2 Early menarche before age 12 has been associated with severe consequences such as obesity, Type 2 diabetes, and cardiovascular disease later in adulthood, and increased exposure to depression, anxiety, low self-esteem, and risk-taking behaviors.3,4
Early menarche has caused significant parental anxiety and stress because maternal distress is shown to directly affect adolescent adjustment and developmental outcome.5-8 Cultural practices shape how parents interpret menarche, ranging from stigma and secrecy to seeing it as a ritual that should be celebrated.9,10 Cross-national studies indicate mixed mother-daughter communication on the topic of puberty because of embarrassment, a generation gap, and misinformation.11,12
There are still gaps in the area of menstrual health education, and it is necessary to implement integrated, culturally sensitive curricula where parents are also involved.13,14 Age of pubertal onset has been progressively declining in various parts of the world due to increased rates of obesity, enhanced nutrition and exposure to environmental factors. 1 However, in most low- and middle-income backgrounds, restrictive measures and taboos concerning menstruation are widespread, 15 and in high-income areas, parents prefer medical intervention or reassurance.8 Despite such heterogeneity, there remains a significant gap in knowledge about the lived experiences of parents, coping mechanisms, and the kind of support that they need.
It is important to distinguish between early menarche, early puberty, and precocious puberty, as these terms are not interchangeable. Early menarche generally refers to the onset of first menstruation at a younger-than-average age, often operationalized as before 12 years in epidemiological studies. 16 Early puberty refers more broadly to the earlier development of secondary sexual characteristics relative to population norms. 4 In contrast, precocious puberty is a clinical diagnosis defined by the onset of pubertal development before age 8 in girls and requires endocrine assessment and possible treatment. 17 The review uses “early menarche” when referring to age at first period and “precocious puberty,” “early menarche” only when studies report clinical diagnoses or endocrinology cohorts.
Although biological and environmental causes of earlier puberty are outlined by epidemiological studies, there are limited studies to investigate parental concerns, attitudes, and experiences systematically. A scoping review is needed to trace the extent and nature of current evidence, outline shared issues and gaps in knowledge, and guide supportive interventions for both families and adolescents.
Method
This scoping review followed the methodological framework18,19 and documented on the Preferred Reporting Items of Systematic Reviews extension by Scoping Reviews (PRISMA-ScR) checklist. 20 The aim was to map and synthesize existing evidence on parental concerns, attitudes, and experiences in the area of early menarche and puberty.
Research Question
The main research question was the following: What are the sources of evidence on parental concerns, attitudes, and experiences involving the onset of puberty and early menarche in girls?
Eligibility Criteria
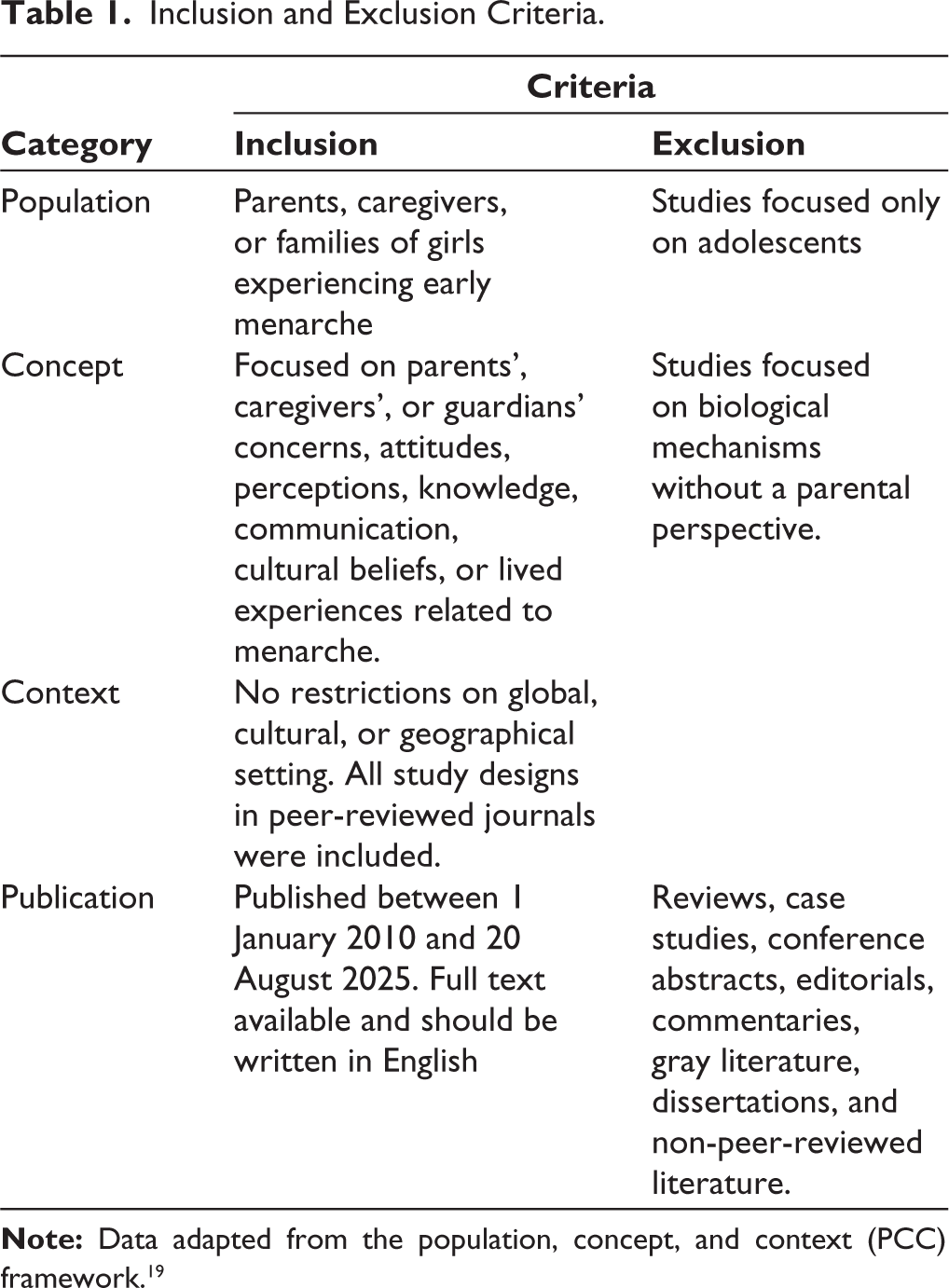
The Population, Concept, and Context (PCC) framework guided the eligibility criteria. 21 Table 1 presents the inclusion and exclusion criteria, which were developed to address the research question.
Inclusion and Exclusion Criteria.
Information Sources and Search Strategy
PubMed, Scopus, ProQuest, and EBSCOhost systematic searches were done in August 2025 using database-specific keywords and Boolean operators. To identify relevant articles for the review, a search was conducted using specific keywords. The additional search methods included citation tracking and Research Rabbit. The search strings and limits, which were used in each database, are given in the supplementary data in full.
Selection of Sources of Evidence
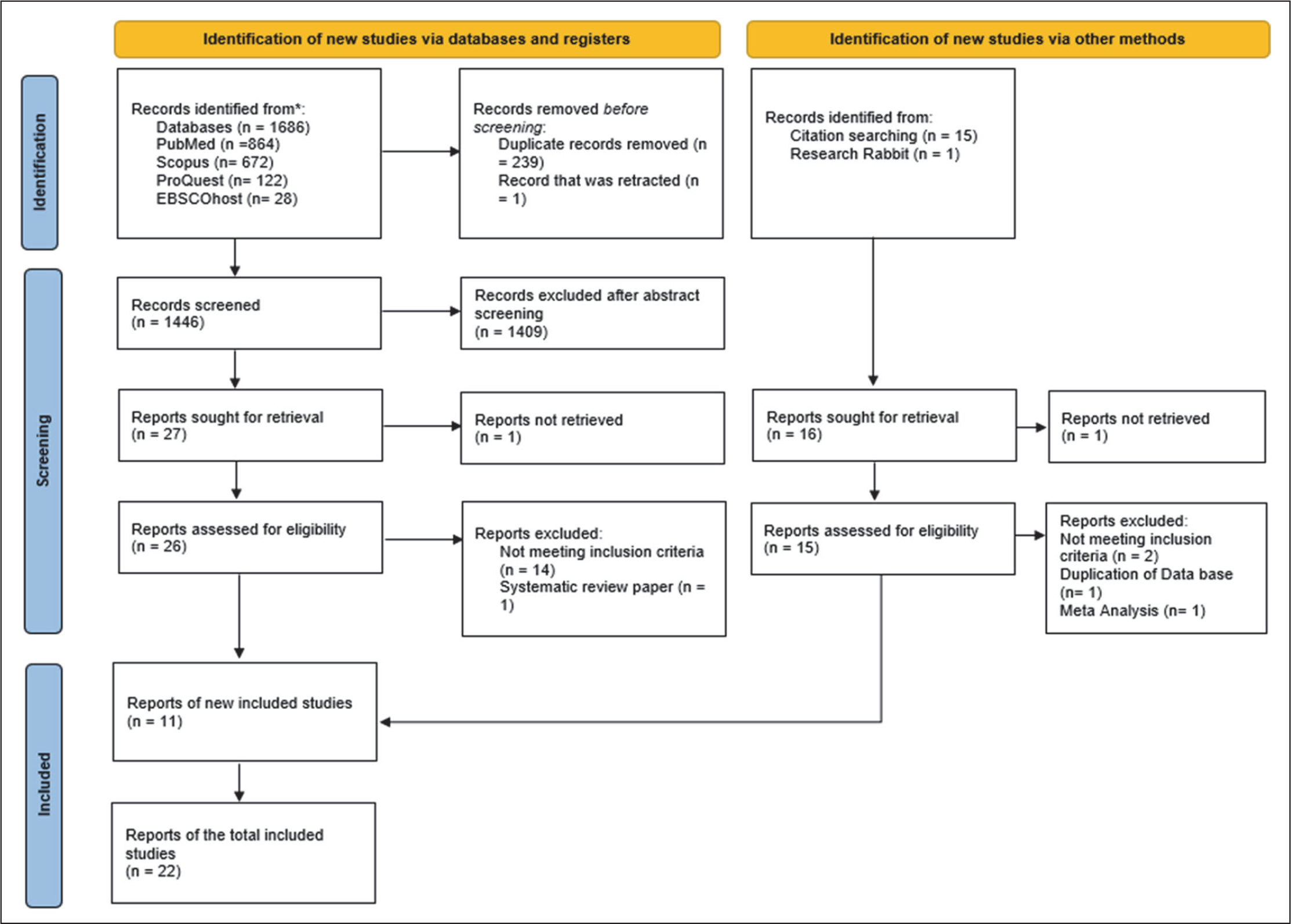
All the records were exported into Zotero as reference materials. After removing duplicates and retracted records, 1,446 records were screened; 45 full texts were evaluated; 22 studies were incorporated. The selection process is depicted by a PRISMA-ScR flow diagram (Figure 1).
PRISMA 2022 Flow Diagram.
Data Screening and Charting Process
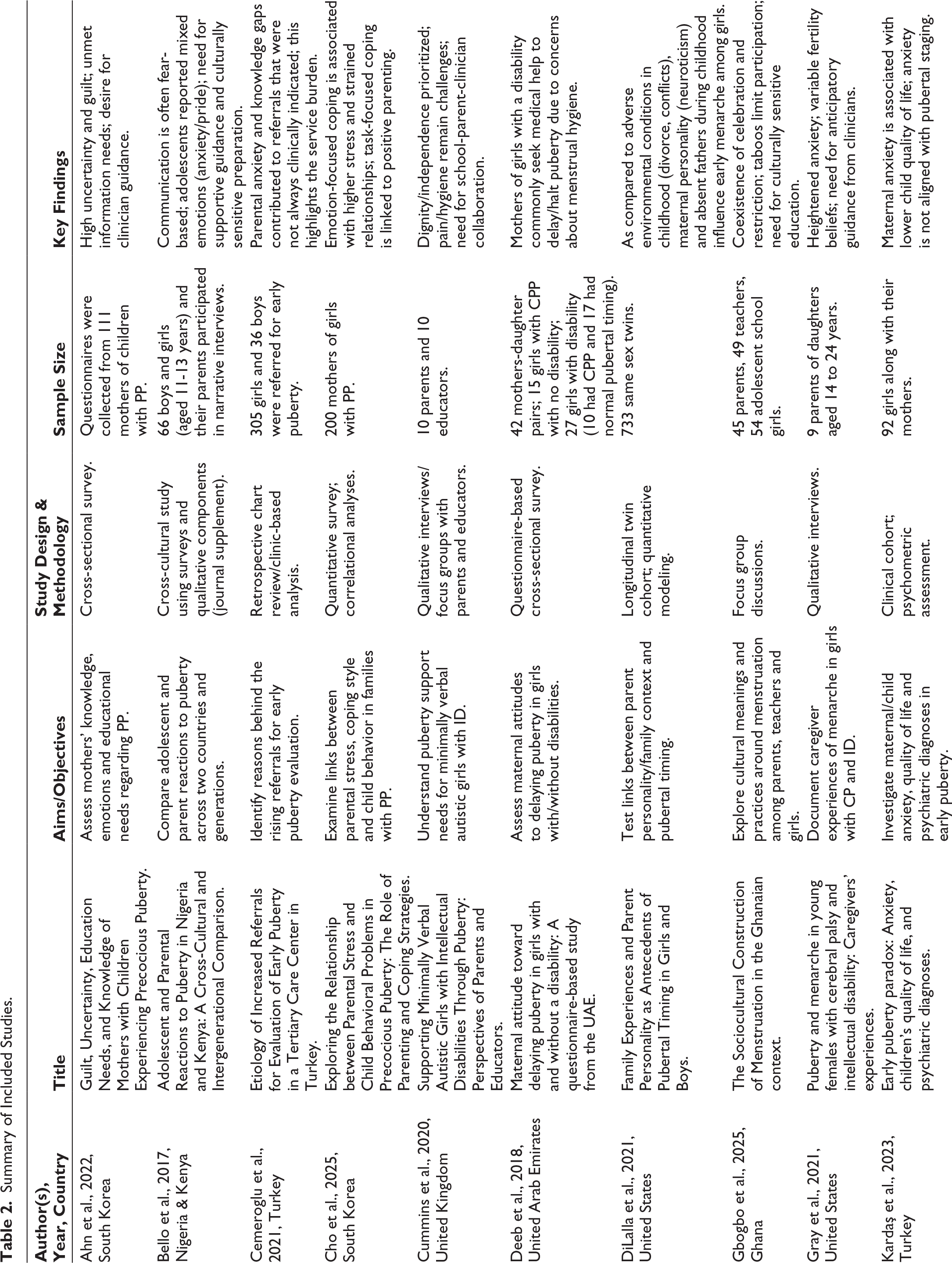
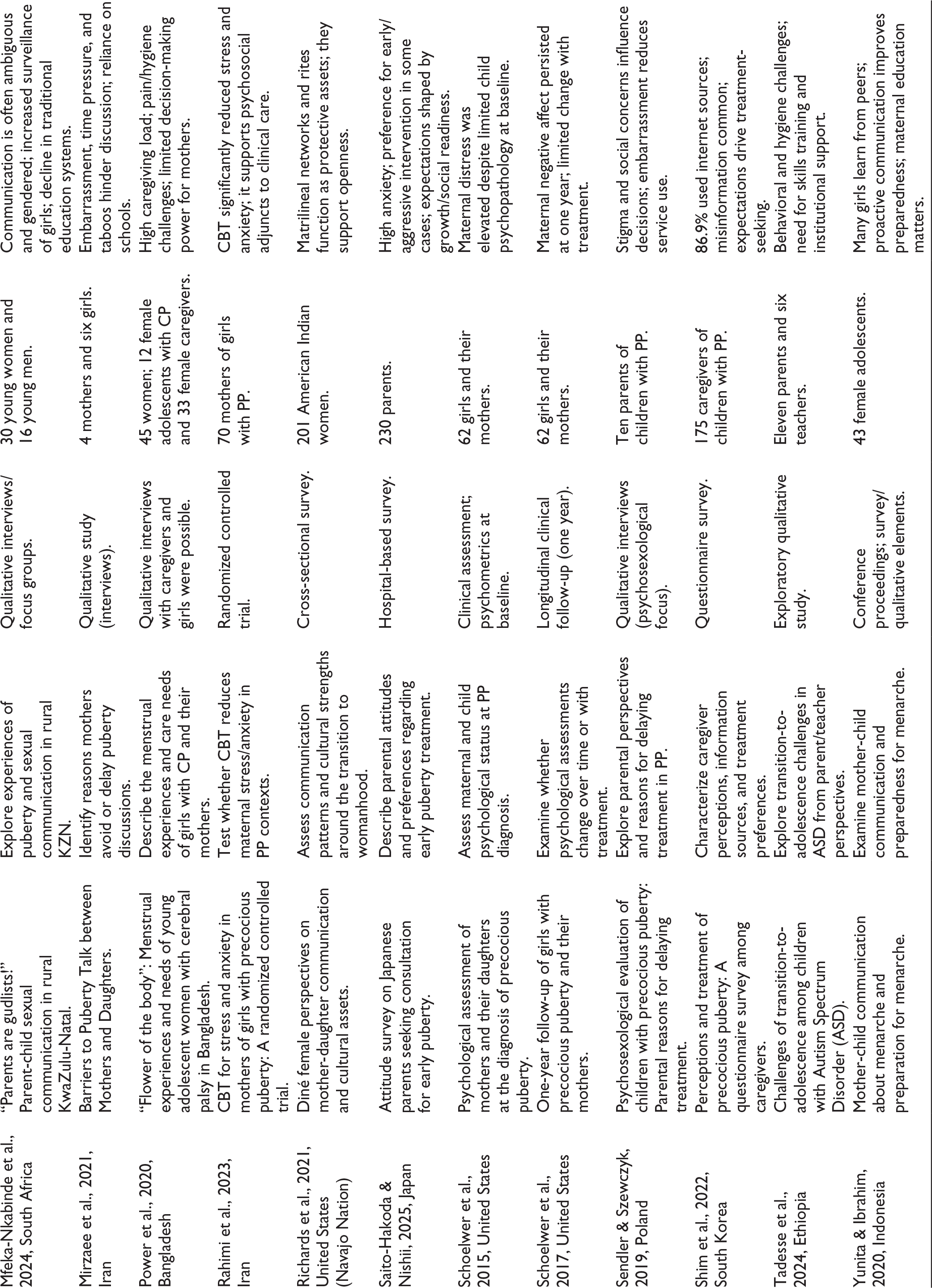
Data was screened by two independent reviewers, and any disagreements were resolved through discussion and consensus by the third reviewer. 19 A data charting form was designed based on the Joanna Briggs Institute guidance. 21 Data retrieved were incorporated (Table 2).
Summary of Included Studies.
Reporting
Results are provided according to the PRISMA-ScR checklist, which allows ensuring clear and full reporting of the scoping review procedures and outcomes. 20 Thematic analysis of the findings from all included studies was conducted, and the results are summarized. 22
An inductive approach was adopted to develop themes. All the studies were scrutinized and coded based on recurring patterns in the data. These codes were then combined to form broader themes. The resulting themes were also analyzed across various study designs, such as qualitative, clinical, and survey-based, to ensure that they captured common trends across different settings. Any overlap or differences in theme categorization were resolved through discussion until agreement was reached.
No formal quality assessment or risk-of-bias appraisal of the included studies had been conducted, because the aim of the present review was to map the extent and nature of the literature rather than assessing the effects of interventions or study validity.
Results
The review synthesizes evidence on parental concern, anxiety, attitudes, perceptions, communication patterns, and coping strategies. Although these constructs are conceptually distinct, they are closely interrelated within family systems during developmental transitions. While not all included studies explicitly examined “parental concern” as a primary outcome, they were included because they addressed parent-related experiences, responses, or behaviors in the context of early menarche and were therefore relevant to the scope of this review.
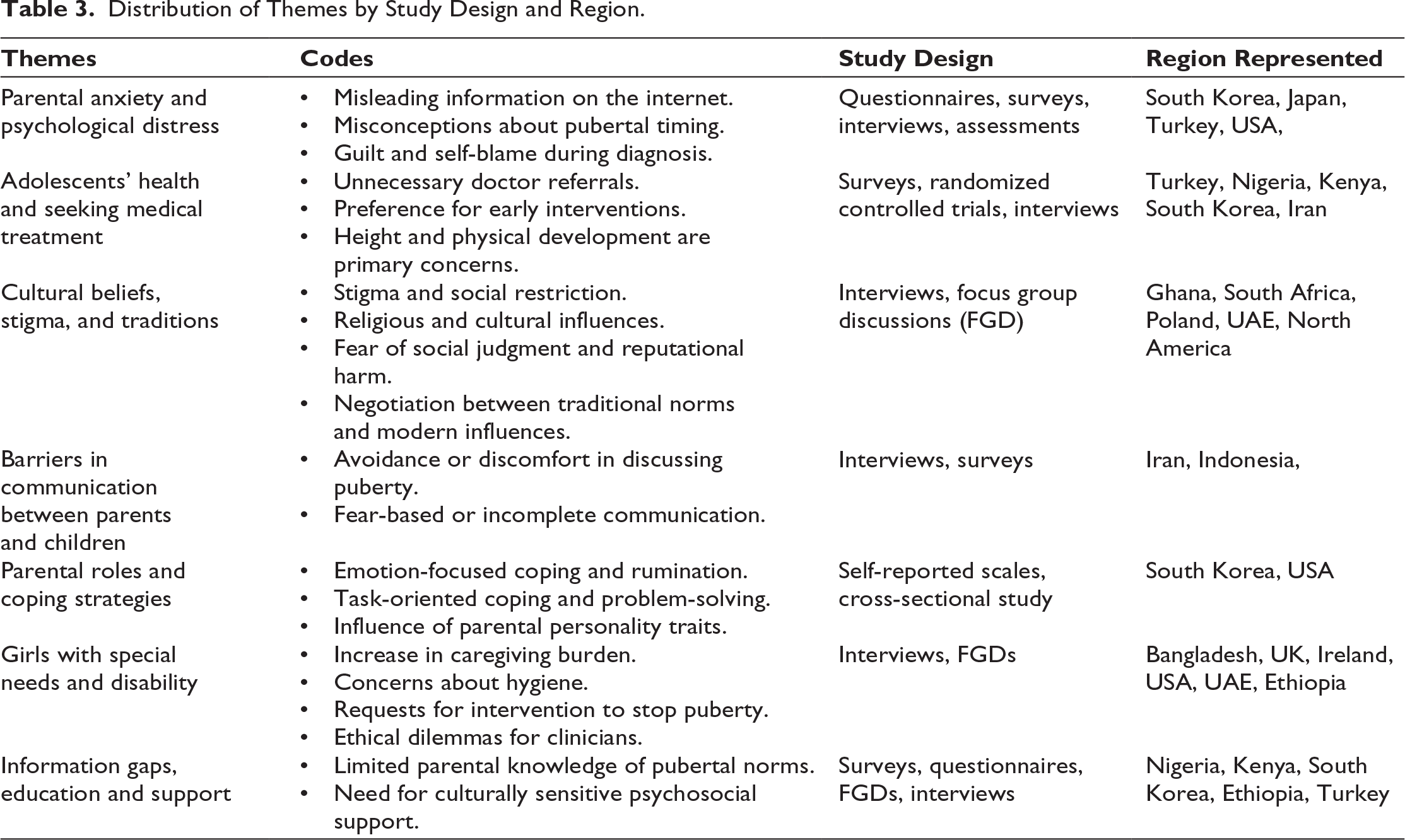
The scoping review was based on the synthesis of 22 peer-reviewed articles published in East Asia, North America, Sub-Saharan Africa, the Middle East, and Europe. Of the 22 included studies, 12 were qualitative, and 10 were quantitative studies. The results were grouped into seven themes. Table 3 describes the mapping of themes.
Distribution of Themes by Study Design and Region.
Theme 1: Parental Anxiety and Psychological Distress
In South Korea, parents of children with PP used internet resources for information, most of which were misleading and unreliable, which resulted in feelings of anxiety, guilt, and increased stress because of the diagnosis of their child.23,24 Japanese parents voiced similar fears and stated that they were too anxious even at the time when their child did not need medical attention, which were often based on misconceived ideas of pubertal development and inaccurate memories of their own pubertal development. 8 Mothers of children with early menarche reported shock, grief, guilt, and financial strains comparable to the stress experienced by parents of chronically ill children. Most of them explained the daughters attaining early menarche by the lack of parenting or by genetic predispositions, reporting loneliness or depressive symptoms, particularly where the spousal or family support was insufficient. 25
In Turkey, personal memories about their own experiences of puberty made mothers concerned about their girls. The anxiety regarding the earlier timing of puberty was a psychosocial issue and short final height. 5 Maternal anxiety was positively correlated with anxiety in daughters and negatively correlated with the perceived quality of life in daughters. Maternal anxiety was inconsistent with objective pubertal timing, which reinforced the fact that perceived worries, as opposed to clinical reality, were the main basis of maternal stress. 6 Studies in the United States showed high levels of depression in the mothers during their daughter’s diagnosis of PP, although the daughters did not exhibit any psychological dysfunction at baseline. 7 The longitudinal follow-up showed that even though no maternal psychopathology was found to be persistent, mothers still reported negative affect 1 year later, regardless of whether their daughters had reached puberty. 26
Theme 2: Adolescents’ Health and Seeking Medical Treatment
Collectively, the studies show that parental anxiety influences their health-seeking behavior. The constant worries about the health of their daughters were also present as parents often prioritized the height prognosis and menarche time, triggering unnecessary doctor visits. Parents indicated that they would prefer aggressive care during the first hospital visit of their child, even in cases when no overt daily problems were reported. 8
Some parents held on to the misconceptions about the normal timing of puberty; along with the over-emphasis of early puberty by the electronic media, this exacerbated unnecessary pediatric endocrinology referrals,5 consistent with the research, which confirms that the information-seeking behavior of the parents shapes treatment expectations. 23
Theme 3: Cultural Beliefs, Stigma, and Traditions
The cultural and religious structure shaped how parents perceived and managed puberty. In the UAE, parents of girls with disabilities stated that the religious and cultural considerations influenced pubertal management and sought medical help to delay or block pubertal development, creating ethical dilemmas. 27 Parents in Poland expressed concerns regarding social stigma in relation to early physical development, and were reluctant to utilize professional services due to embarrassment or denial. At the time of families seeking medical attention, there were fears about the social consequences of the treatment process and the long-term negative outcomes of the treatment. 28
On the other hand, the Indigenous Diné in the United States used protective cultural resources like extended family support, matrilineal networks, and traditional rites of passage to offset risks, including substance misuse and early pregnancy. 29 In rural South Africa, parental communication concerning puberty was usually ambiguous, evasive, and highly gendered, with more surveillance of the girls, which reflected the current gender practices. 30
Menstruation was both celebrated and stigmatized. In Ghana, both parents and adolescents reported having lived with restrictions and taboos, like not being allowed to do domestic chores or participate in religious activities, and at the same time having the need to change. Although some families maintained the traditional norms, some opposed them, thus shedding light on the conflict between modern education and cultural continuity. 10
Theme 4: Barriers in Communication Between Parents and Children
Parent-daughter communication became one of the key factors of preparation and emotional adjustment. Parents in Nigeria and Kenya indicated that they gave instructions on body changes and relationships, but did not always do this; some mothers used fear as a communication method. Adolescents themselves reported mixed feelings, including anxiety and pride, and a need to stay confidential. 31 In Iran, mothers often found it inappropriate to discuss puberty, and this was attributed to their lack of awareness, being too busy, or assuming that schools would provide the information. The working mothers, especially, had limited time to communicate, and cultural taboos made the discussion about puberty uncomfortable. 32
Poor mother-daughter communication was a cause of anxiety among girls in Indonesia during menarche. Educated mothers had more knowledge and experience in educating their children about menstruation. A good number of teenagers said that they had learned through their friends and not their parents. Good interaction minimized anxiety and enhanced the preparedness of girls to menarche, and poor interaction indicated that many girls were unprepared. 33
Theme 5: Parental Roles and Coping Strategies
The style of parenting was also a major contributor to family adjustment and coping. In South Korea, maternal stress caused emotion-based coping, where the focus was on regulating emotional distress caused by stress rather than directly solving problems. These strategies were used in situations perceived as less controllable. The parents used rumination and daydreams to preoccupy themselves and cope with the problems. Emotion-based coping strengthened negative parenting and aggravated behavioral problems in children. Task-oriented coping, on the contrary, where mothers viewed stress as a solvable problem and actively tried to solve it without being emotionally involved, helped improve positive parenting attitudes. 25 The study reiterated the significance of problem-oriented interventions, especially collaborative interventions that included other family members.
The longitudinal twin data study in the United States indicated that the family context and parent personality also influenced the timing of puberty. Girls with absent fathers during the ages 4-5 years reached menarche earlier than girls with fathers present, regardless of their temperament. Early menarche in girls was associated with higher maternal neuroticism scores. Parent personality traits showed greater consistency in shaping children’s developmental patterns than other family experiences, like divorce or conflict, and parental dispositions contributed to how parents managed pubertal transition. 34 Psychotherapeutic interventions proved to be effective. In Iran, cognitive-behavioral therapy (CBT) was significantly able to reduce stress and anxiety in mothers of girls with PP, and group counseling could help them to replace the maladaptive thinking with positive coping mechanisms, which improved the quality of life of mothers. 35
Theme 6: Girls with Special Needs and Disability
Parents of girls with disabilities feel embarrassed and anxious about early sexual development. Parents had trouble making decisions when it came to medical treatment. Parents insisted on surgery to suppress pubertal development despite the functional state of their daughters. They claimed they were concerned, humiliated, and worried about their girls not being able to handle their early sexual life and potential rejection by peers. 27
Adolescent females with ASD in Ethiopia were characterized by severe behavioral, emotional, and hygiene problems associated with menarche and required a lot of parental or teaching care. 36 Menstruation was perceived by mothers of the girls with cerebral palsy in Bangladesh as a sign of maturity and a source of shame. They reported that they must silently bear with caregiving load, indicating larger family systems of patriarchy, where mothers had responsibility but not power to make decisions. 37
Parents of girls with cerebral palsy and intellectual disability frequently feared menarche. Expectations of fertility ranged from beliefs of infertility to potential use of surrogacy or hysterectomy, highlighting the diversity as well as the contradictory nature of beliefs. Clinicians were advised to expect such perceptions and reassure and offer correct information. 38 Dignity and autonomy emerged as important concerns among minimally verbal autistic girls during menstrual management in the United Kingdom. Although parents were initially concerned, most of them noted that their daughters were coping in a better way than they had anticipated. However, there was still an issue of period pains, especially when the girls could not express discomfort. It was emphasized that collaboration between schools, parents, and medical experts is necessary. 39
Theme 7: Information Gaps, Education and Support
Across settings, a major barrier was an insufficient level of parental knowledge. There were misconceptions about pubertal timing and unnecessary hospital referrals that led to additional burden to families and health care systems.5,8 Education of parents about the normal timing of puberty may help avoid unnecessary referrals, parental anxiety, and financial burden to society. 5
Parents often said that they needed to have proper education programs to lessen the feeling of guilt, doubt, and dependence on untested treatment. Mothers were inclined to find unproven methods in case they did not have explicit guidance. Skills training and psychosocial interventions were emphasized by the parents. 36 This insight necessitates specific interventions that provide psychological support and evidence-based information. 24 Structured programs need to be designed to enable mothers to adjust to the task-based coping strategies, 25 and treatment plans need to be redesigned to suit cultural anticipations and information-seeking behavior among parents. 23
Discussion
This review reflects the complex nature of parental concerns surrounding early menarche. One of the important points identified was the prevalence of psychological burden on parents. It has been shown, through studies, that most parents seek unverified resources on the internet and have false ideas about what is both normal and early puberty, which causes anxiety and unnecessary doctor appointments.5,8,23,24
Stress levels of mothers are positively correlated to the quality of life of their daughters,6 and maternal distress levels during the time of diagnosis are elevated even when there is no other significant psychological dysfunction among children7,26 and continue to increase regardless of the clinical condition of the child and the outcomes of treatment. The parental stress, which is also influenced by cultural and contextual priorities, is a possible factor in increasing health-seeking behavior. These are in line with evidence demonstrating that parental anxiety influences children’s emotional and behavioral performance. 40 Parents indicated a high tendency to aggressive medical intervention, with an overall focus on growth, physical attractiveness, and social readiness 8 echoing trends where puberty onset is being medicalized, 17 raising concerns about overdiagnosis, overmedicalization and overtreatment highlighting the need for psychosocial support such as CBT, which has been found to reduce maternal stress and anxiety, 35 as an addition to standard medical treatment.
The cultural beliefs and traditions have an impact on the way puberty is managed in families, creating fears of stigma and social exclusion. 28 During menarche, girls are not included in family, religious, or social activities. Cross-cultural literature suggests that menstrual stigma and secrecy continue to be some of the most common obstacles to adolescent health in the global context.41,42 However, there is a change in attitude where some parents indicated the need to overcome stigma and create open communication with their daughters, thus unveiling a movement between tradition and modernity.10,29-31
The communication between parents and adolescents has become a frequent issue. Mothers’ avoidance or delay of discussion about puberty is due to embarrassment, ignorance, or conflicting demands, 32 as they do not provide information on menarche, believing that daughters will learn on their own, though. 33 Facts and fear-based strategies revealed how cultural norms and the education of the mother impact the quality of parent-child dialogue, 31 and become the source of misinformation within generations. Evidence also proves that open communication promotes resilience and minimizes risky behaviors. 43
The parenting techniques and family environment influence the puberty experience. Mothers who used emotion-focused coping styles like rumination and daydreaming due to stress caused by being the primary caregivers of daughters with PP led to poor parenting relationships, but task-based strategies like actively trying to solve the problems without being emotionally involved were linked to healthier family relationships and promoted positive parenting attitudes. 25 Environmental stressors were less predictive of when children reached puberty than parental personality traits and family context, 34 which could affect pubertal development indirectly via chronic stress exposure, emotional instability, attachment security, and caregiving consistency within the family. These results suggest that parental personality traits are an underexplored factor by which early pubertal timing can be influenced.
Parents and educators tend to perceive menarche in females with disabilities as a burden that requires high parental and institutional support. Parents sometimes demanded that their daughters have permanent surgical interventions to stop puberty. While such requests are often based on genuine concerns about hygiene management, vulnerability to sexual abuse, and long-term caregiving responsibilities, they overlap with issues of child rights, bodily autonomy, and assent. Clinicians, therefore, face ethical dilemmas when parental anxieties overshadow the voice of adolescents.27,36–39 Such findings highlight the risk of overmedicalization of puberty processes and the need to adopt disability-sensitive education and inclusive health policies to support the menstrual equity needs of girls with disabilities. 14
The literature indicates that an information gap exists across all settings. Mothers were not equipped to handle early menarche in children, 24 which was worsened by internet misinformation. 23 The lack of education increases both parental distress and the financial burdens of health care systems by creating unnecessary referrals. 5 All these studies emphasize the necessity of accessible learning programs. These results resonate with broader literature on adolescent health, where limited parental knowledge remains a barrier to menstrual literacy. 9
Implications
The evidence highlights the significance of the medical, psychological, and sociocultural approaches in dealing with early menarche. The healthcare providers should develop interventions and psychoeducation modules for parents and offer anticipatory guidance, which is socio-culturally sound and context- sensitive. Policies should go beyond biomedical management and address stigma, misinformation, and intergenerational silences through community-based and school-based education. Family intervention of girls with disabilities should focus on the inclusion of resources and joint planning with parents and teachers
Limitations
The scoping review has several limitations. The eligibility criteria limited the inclusion to English-language, peer-reviewed articles published between 2010 and 2025, which might have omitted relevant non-English articles and research in underrepresented areas. The exclusion of gray literature may also have introduced potential publication bias. Since scoping reviews are designed to map evidence instead of evaluate the quality of the study, the results reflect the diversity of themes identified and lack quality appraisal. There was heterogeneity in the study designs, populations, and measures used in qualitative and quantitative studies, making it hard to do further synthesis. Lastly, the views of fathers and other caregivers were scarcely mentioned in source studies, limiting the ability to understand more about the family dynamics.
Conclusion
This scoping review has summarized the evidence based on 22 studies in various settings and demonstrates that parental worry regarding early menarche is widespread and motivated by feelings of distress, cultural meaning-making systems, and lack of reliable information and services. Results indicate that maternal anxiety tends to influence both health-seeking and parenting behavior, that communication and cultural values have a significant impact on preparedness, and that the family of a girl with disabilities experiences a significant burden. The review reveals that there is an urgent call to implement culturally sensitive, parent-centered education and psychosocial supports along with cautious clinical decision-making to lower the unnecessary medicalization and enhance family well-being.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors gratefully acknowledge CHRIST (Deemed to be University), Bangalore, for their unwavering support throughout the project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not required because the study is a scoping review and does not involve primary data collection or human participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the CHRIST University, Bangalore, under the Seed Money Scheme (Reference Number: CU:CRP: SMSL-2418).
Informed Consent
Not applicable, as this study did not involve human participants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.