
Abstract
Introduction:
Structured physical activities provide predictability, creating a lower-stress environment for autistic children to learn necessary skills. This study aimed to identify the effects of structured physical activities on behavior issues, sensory issues, skill acquisition, and the severity of autism spectrum disorder (ASD) among autistic children.
Material and Methods:
This institution-based experimental study was conducted at a center for neurodevelopmental disorders in Jaffna, Sri Lanka, among 24 autistic children. In addition to their routine therapy, 12 of these children received adjuvant structured physical activity (intervention group), while the other 12, matched for age, gender and severity of ASD, engaged in unstructured physical activities (control group) for 40 minutes a day, thrice weekly for 3 months. Behavior issues, sensory issues, skill acquisition, and severity of ASD were measured before and after the intervention using a locally developed behavior checklist, Sensory Profile-2, Assessment of Basic Language and Learning Skills - Revised, and Childhood Autism Rating Scale, respectively. Data were analyzed in the R statistical computing software using linear multilevel regressions.
Results:
On average, the children were aged 4 years and 2 months (SD = 13 months). Children in the intervention group showed a greater decrease in behavioral issues (p < .001), visual (p = .004) and movement processing (p < .001) issues, and severity of ASD (p = .016), and greater improvement in gross motor, fine motor, social interaction, and play and leisure skills (p < .001 for all).
Discussion:
Incorporating structured physical activity as an adjuvant to routine therapy for autistic children will bring about improvement in multiple aspects of ASD. Expanding this program in other low-resource settings can facilitate early intervention for ASD and make such interventions accessible to all.
Introduction
Within the span of a decade, the prevalence of autism spectrum disorder (ASD) has increased from 0.62% 1 to 1%. 2 A study published 15 years ago assessed the prevalence of ASD in Sri Lanka and found it to be 1.07% 3 —much higher than the prevalence of ASD in other South Asian countries, and the global prevalence at that time. 4 Although recent studies have not assessed the current prevalence of ASD in the country, clinicians and other service providers have felt the increased need for service provision. 5
ASD is a complex neurodevelopmental disorder that involves persistent challenges in social interaction, communication, restricted interests, repetitive behavior, and sensory issues. 6 There is substantial variability in the presentation of autistic children and in the challenges they face. Hence, interventions to help these individuals are also varied, with speech and language therapy, occupational therapy, physical therapy, behavior therapy, and play-based therapy among the commonly used interventions.
Compared to neurotypical individuals, many autistic individuals exhibit lower motor skills, reduced coordination and balance, and impaired visual-motor integration. 7 Therefore, physical activities, especially outdoor activities, are included in their therapeutic routine to improve not only balance, coordination, muscle strength, and joint strength but also motor skills, skill-related fitness, and overall physical fitness. 8 A carefully designed physical activity program has the ability to provide autistic children with a fun environment and safe setting for interacting with other children, thereby offering great opportunities for developing and practicing social skills. 9 Furthermore, studies show a decrease in stereotypy, aggression, off-task behavior, and improved objective sleep following physical activities. 10 Studies have also found that physical activities improve visual attention. 11 Thus, physical activity programs for autistic children can produce moderate to large benefits in multiple aspects of ASD.
Physical activity can be structured or unstructured, both of which are important for a child’s development. 12 In structured physical activity, an adult initiates or joins in with the child’s play and offers directions or guidelines. Conversely, unstructured physical activity, often referred to as free play, is unplanned and arises spontaneously based on the child’s interests in the moment. 13 While free play encourages a child’s creativity, imagination, and problem-solving skills, structured physical activities make games and play activities more predictable and manageable for autistic children by providing the steps, skills, activities, or ideas needed to reach the end goal of the activity. 14 The consistency and predictable routine create a lower-stress environment where the children can learn the skills they need to play and interact successfully with other children. This also helps reduce challenging behaviors caused by the anxiety and frustration associated with inconsistent routines.
Healthcare for autistic children demands an individualized, multidisciplinary approach, including not only medical interventions but also specialized behavioral, speech and language, and educational therapies tailored to each child’s deficit profile. 15 These interventions are costly, labor-intensive, and require the providers to undergo lengthy periods of training, all of which can be challenging for centers in low-resource settings 16 characterized by factors such as financial pressure, suboptimal healthcare service delivery, limited infrastructure, paucity of knowledge, and human resource limitations. 17 Therefore, there is a dire need to develop interventions for autistic children that not only address multiple challenges in ASD but are also easy to implement and do not require extensive training. Including a structured physical activity program as an adjuvant is a good first step, as the effects of physical activity have been seen in multiple aspects of ASD, including improved communication and motor skills and reduced stereotypy and aggression. Despite these clear advantages, the benefits of structured physical activity have not been systematically explored among autistic children in Sri Lanka. This study attempted to fill this gap by measuring the effects of a carefully designed structured physical activity program for autistic children attending a center for neurodevelopmental disorders in northern Sri Lanka.
Materials and Methods
Study Setting and Participants
This institution-based, interventional study was conducted at Mathavam—a center for neurodevelopmental disorders in northern Sri Lanka, catering to a significant number of autistic children, predominantly from northern Sri Lanka. While this center offers a range of therapies comparable to those available in developed countries, this center is reflective of a low-resource setting due to the broader contextual environment, including financial constraints, limited availability of trained professionals, limited ASD-specific training for these professionals, and a lack of systemic support for neurodevelopmental services in the region. Furthermore, the client-to-staff ratio is considerably higher than recommended international standards, with a single therapist often being responsible for a large caseload, limiting the intensity and individualization of the intervention that can be provided.
This study was carried out with 24 children between the ages of 3 and 8 years, who were diagnosed with ASD at the center. These children were following speech therapy, play therapy, occupational therapy, or physiotherapy, but had not yet begun early intensive behavioral intervention (EIBI). Children who had begun EIBI were excluded from this study to avoid confounds. Children with severe physical deformities that limit their motor movements, physical activities, and independent play ability were also excluded from the study.
Before recruiting participants, all the children attending the center were screened for eligibility, after which 24 children were selected to participate in the study based on their regular attendance at the center as well as the parents’ interest and commitment to engaging in regular therapeutic activities. These children were paired according to their age, gender, and severity of ASD, and within each pair were randomly assigned to either the intervention group or control group using a simple randomization method.
The 24 children recruited for this study, like all other children diagnosed with ASD at this center, underwent comprehensive physiotherapy and occupational therapy assessments in which gross motor skills, fine motor skills, balance, coordination, and sensory issues were evaluated and individualized therapy goals were set with specific target activities, such as tandem walking, ball catching and throwing, jumping on a trampoline, animal walks, and swing activities for physiotherapy, and threading beads, lacing cards, pegboard activities, and tracing lines for occupational therapy. These activities were prescribed for a defined period, and progress was reviewed periodically to adjust goals according to the child’s improvement. All 24 children continued to receive their routine therapy after being recruited for the study. In addition, 12 of these children received adjuvant structured physical activity (intervention group), while the other 12 engaged in unstructured physical activities (control group) for 40 minutes a day, thrice weekly for 3 months.
Interventions
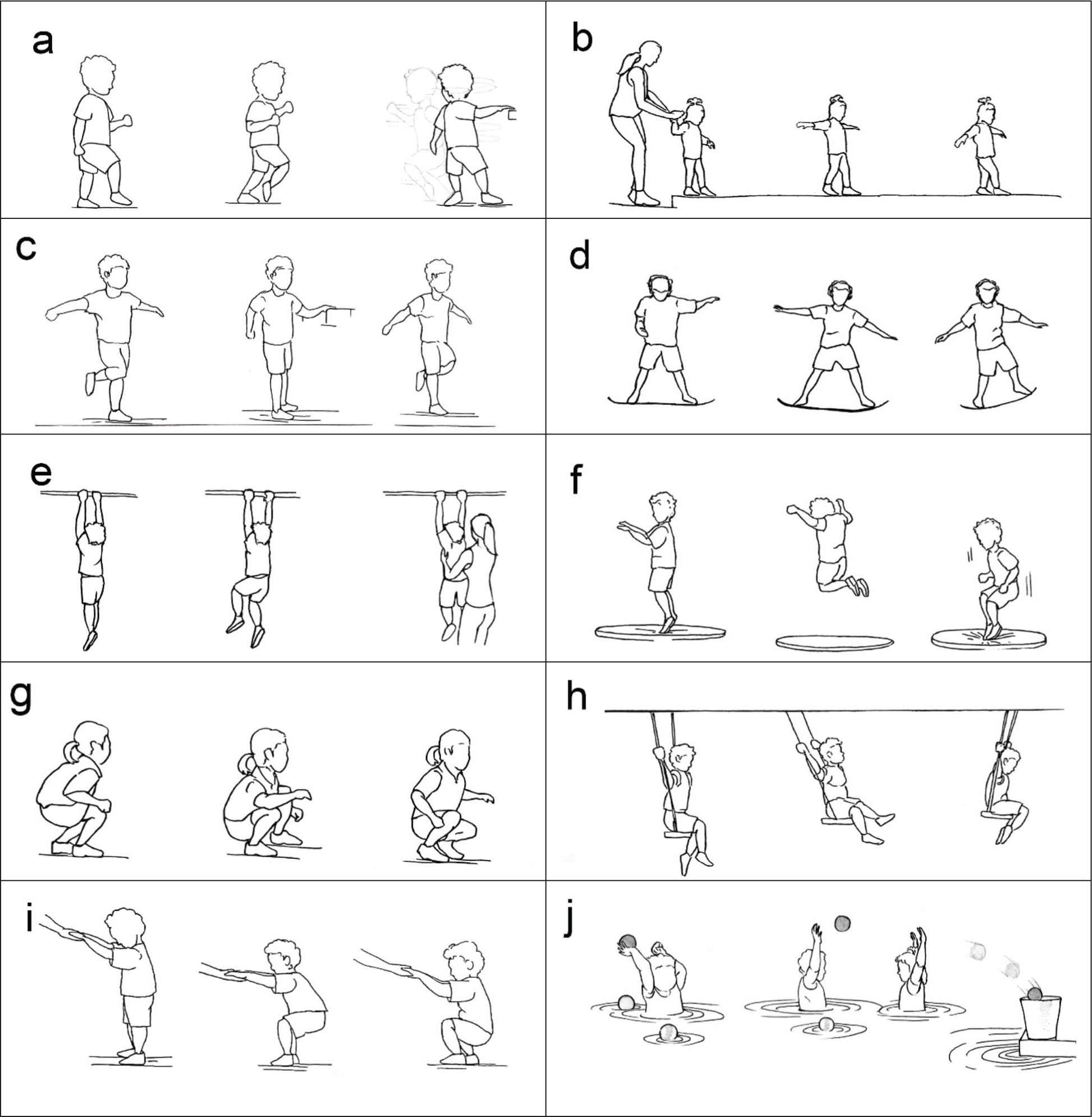
A structured physical activity manual (see Supplementary materials) was formulated based on the investigators’ experience working with autistic children, through trial therapies and extensive literature study. This manual comprises detailed instructions regarding 10 physical activities chosen to help improve the children’s coordination, balance, muscle strength, and joint strength (Figure 1). These activities were designed for a total duration of 40 minutes and included jogging (4 minutes), tandem walking (5 minutes), single-leg standing (3 minutes), balance board activities (3 minutes), bar hanging activities (3 minutes), jumping on a trampoline (3 minutes), animal walks (4 minutes), swinging (3 minutes), sit to stand (2 minutes), and water-based play (10 minutes) in which children were allowed to play in a swimming pool.
Along with the aforementioned regular therapies provided at the center, children in the intervention group engaged in these structured physical activities at the center itself thrice weekly for a period of 3 months. When the children were assigned to the intervention group, their parents were first trained on the selected physical activities using the structured physical activity manual. During the first 2 weeks of the intervention period, the children were trained by a physical therapist who modeled these activities. Once the children had learned these activities, they were prompted as needed using physical prompts or gestures and redirected if they disengaged during the intervention session. The physical therapist was present at all intervention sessions to guide and troubleshoot as necessary. The parents were actively involved in administering these intervention sessions thrice weekly at the center and were encouraged to do so at home on the other days.
Throughout the intervention period, children engaged in these activities in two groups of six. This allowed them to interact with other children, especially during water-based play, where they played in a swimming pool, throwing colored balls at each other and through a shooting ring at the edge of the pool. It also created opportunities to practice turn-taking through activities like swinging and jumping on a trampoline, where they needed to wait for their turn. The children also interacted with the physical therapist, who modeled these activities during the initial period, and parents, who functioned as co-therapists during these sessions.
The children in the control group engaged in 40-minute sessions of unstructured physical activities at the center thrice weekly for 3 months, along with the other regular therapies. During these sessions, children were allowed to create their own activities according to their interests and needs without adult guidance. Examples of unstructured physical activity include riding a toy horse or bike, playing tag, and playing in the playground. Unlike the intervention program, unstructured physical activities did not have a manual. The parents and a therapist were present to encourage the children to engage in physical activities while ensuring safety. Parents were encouraged to be involved in unstructured physical activities at home on the other days of the week.
Study Instruments
Basic sociodemographic data were extracted from the records available at the center. The outcomes of interest were the severity of ASD, sensory issues, and behavioral challenges, which were measured by the Childhood Autism Rating Scale™ 2nd edition (CARS2), Sensory Profile 2, and a locally developed Behavior checklist, respectively. In addition, a few selected skills from the Assessment of Basic Language and Learning Skills - Revised (ABLLS-R) were also analyzed.
CARS2, 18 a 15-item rating scale, is widely used to determine the ASD symptom severity through quantifiable ratings obtained from direct observation of the child. It is administered by a professional familiar with ASD who is trained in administering CARS.
Sensory Profile 2 19 is a standardized family of assessments that evaluates a child’s sensory processing patterns and behavioral responses associated with sensory processing. This family of assessments includes several versions of the tool based on the child’s age, and whether it is based on the observations of parents/caregivers or teachers. Since the participants in this study were all between 3 and 8 years of age, the Sensory Profile 2 Child version, which is designed for children aged 3 years to 14 years and 11 months and is based on the observations of the parents, was used in this study. This version of the Sensory Profile 2 evaluates auditory, visual, touch, movement, body position, and oral sensory processing issues, along with conduct, social-emotional, and attentional responses to sensory issues.
The behavior checklist is an interviewer-administered questionnaire designed and used by the center to assess the behavioral issues of the child and is content validated by local experts. This tool is administered to the parents and contains six sections—social communication issues, restrictive behaviors, mood- and anxiety-related issues, self-regulation issues, challenging behavior, and self-injurious behavior. The social communication section contains 12 items, while each of the other sections contains six items. The parents rate each item on a 0–5 scale based on frequency: 0—not applicable (the behavior has not been observed or is not relevant to the child), 1—almost never (less than 10% of the time), 2—occasionally (around 25% of the time), 3—about half the time (around 50% of the time), 4—frequently (around 75% of the time), 5—almost always (90% of the time or more). Lower total scores indicated fewer behavioral difficulties, and a few items in the social communication section were reverse-scored accordingly.
The Assessment of Basic Language and Learning Skills - Revised (ABLLS-R) 20 is a widely used assessment that explores 544 skills grouped into 25 different repertoires, emphasizing motor, language, self-help, social interaction, and academic skills. This therapist-rated tool is an important skills tracking system used in this center. Of the 25 repertoires, only gross motor skills, fine motor skills, motor imitation skills, play and leisure skills, social interaction skills, and requesting skills were analyzed in this study, as these skills were relevant to the structured physical activity program implemented here.
These assessments were carried out before and after the intervention period by therapists blind to the intervention/control group of the children. All pre-assessments were done within two weeks prior to the start of interventions, while post-assessments were completed within two weeks of completing the 3-month course of interventions.
Data Analysis
Data were analyzed in R statistical computing software. 21 The effect of structured physical activity on each of the outcomes of interest was analyzed separately using multilevel regressions, 22 to account for repeated measures. All models included Group (intervention, control), Timepoint (pretest, posttest), and their interaction term as fixed effects. The categorical variables Group and Timepoint were effect-coded so that the sample grand mean was represented by the estimate of a model’s intercept. The intercept was allowed to vary as a random effect in all models to enable the detection of differences in selected parameters between the pretest and posttest as well as between the intervention and control groups, while controlling for differences driven by the individual children. Following significant Group-Timepoint interactions, pairwise comparisons with Tukey-adjusted p values were conducted.
Results
The mean age of the children in this study was 4 years and 2 months, with a standard deviation of 13 months. The sample consisted of 20 males and 4 females.
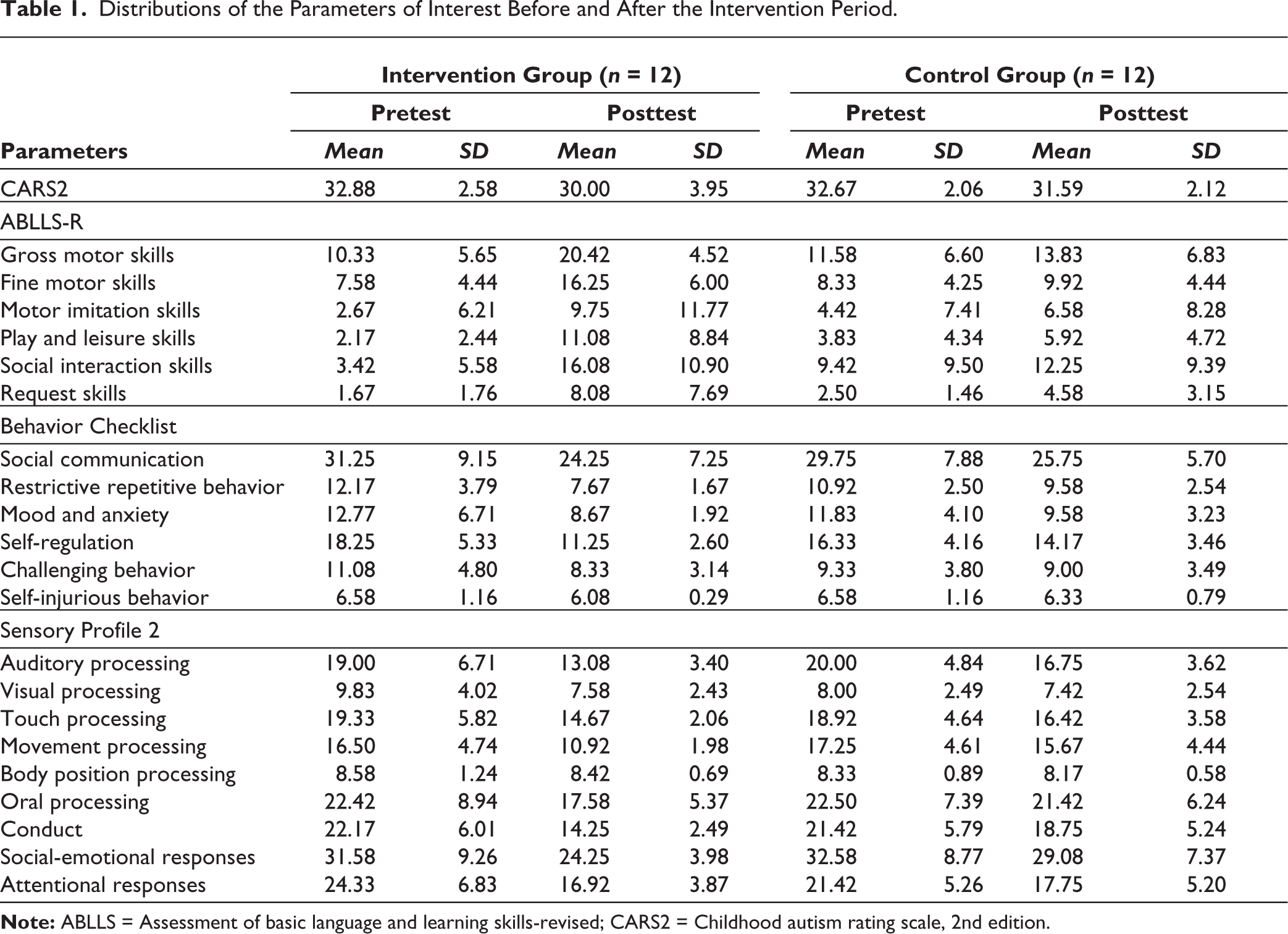
Before the intervention, children in the treatment and control groups did not show significant differences in any of the parameters assessed (Supplementary Table S1). The outcome measures for children in both groups at pre- and post-intervention are summarized in Table 1.
Distributions of the Parameters of Interest Before and After the Intervention Period.
Effect of Structured Physical Activity on the Severity of ASD
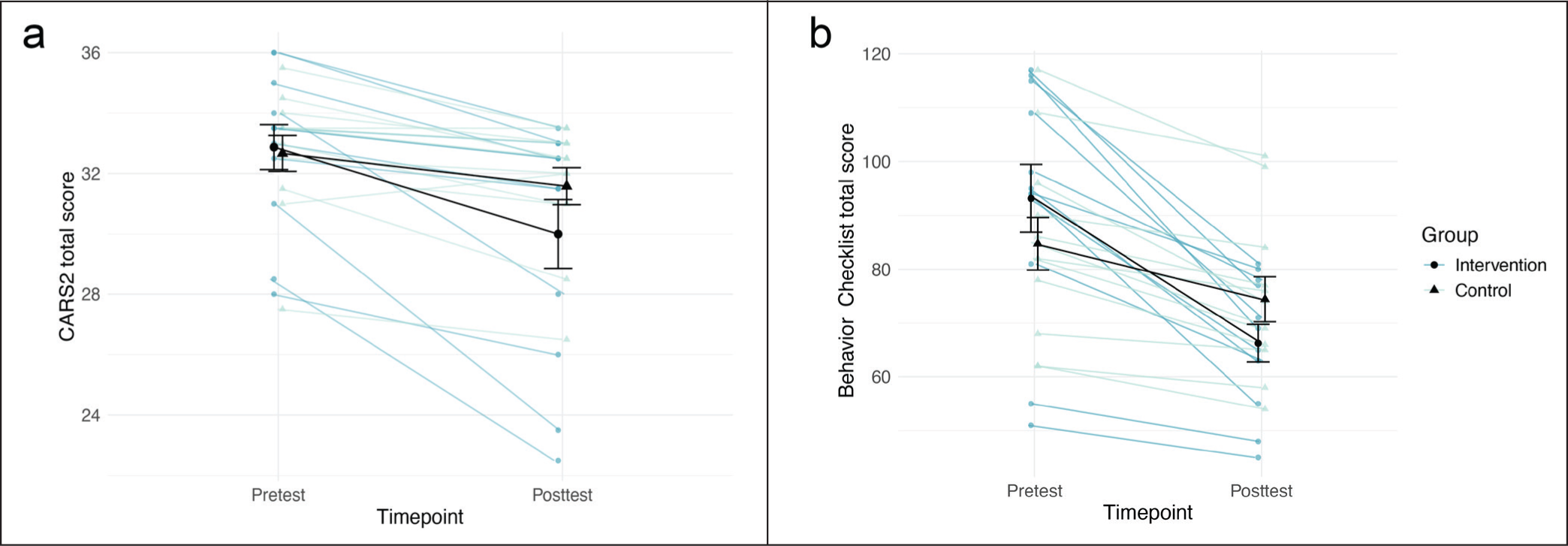
Severity of ASD was assessed using CARS2, in which higher scores indicated greater severity. The children in the intervention group had lower CARS2 scores following the intervention, indicating an improvement in the severity of ASD (Figure 2a). A linear multilevel regression carried out to statistically explore this effect revealed that there was a significant interaction between Group and Timepoint. χ2(1) = 5.85, p = .016, where the CARS2 score of children in the intervention group was significantly lower in the posttest compared to the pretest, b = 2.88, SE = 0.52, t(22) = 5.49, p < .001.
Effect of Structured Physical Activity on Behavioral Issues
Behavioral issues were assessed using Behavior Checklist, where higher scores indicated greater behavioral issues. The total score for Behavior Checklist decreased for children in both groups. However, this decrease was greater among children in the intervention group than in the control group (Figure 2b). The linear multilevel regression exploring this effect revealed a significant main effect of timepoint, χ2(1) = 75.70, p = < .001, where the posttest scores were less than the pretest scores for all, and a significant interaction between Group and Timepoint, χ2(1) = 15.00, p = < .001. Pairwise comparisons revealed that while both the control group, b = 10.33, SE = 3.03, t(22) = 3.41, p = .012, and the intervention group, b = 26.92, SE = 3.03, t(22) = 8.89, p < .001, had significantly lower total Behavior Checklist scores in posttest than pretest; this difference was greater in the treatment group.
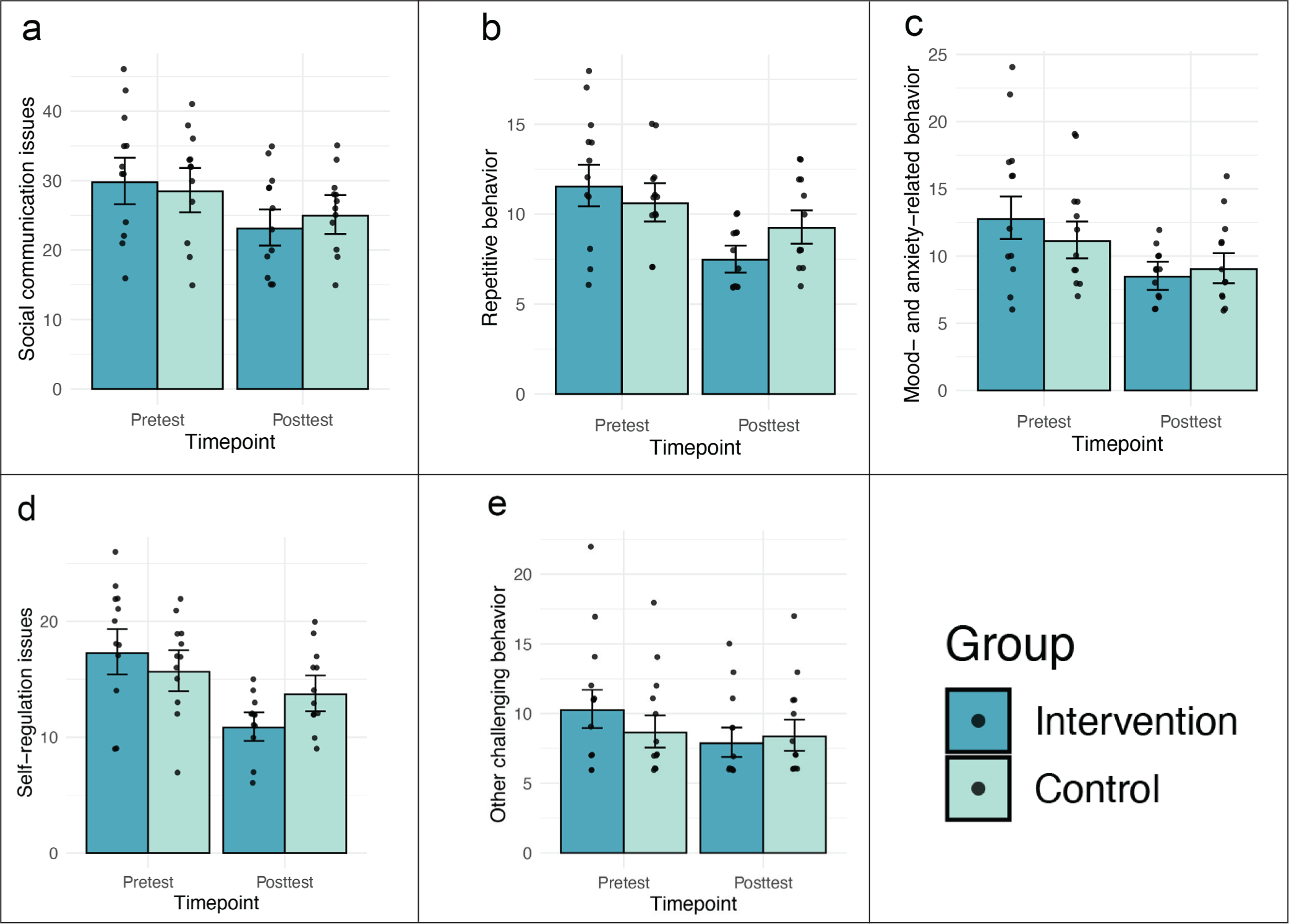
When looking at the individual sections of the behavior checklist, structured physical activity had a significant effect on social communication issues, repetitive behavior, mood- and anxiety-related behavior, self-regulation issues, and other challenging behavior, but not on self-injurious behavior. These sections were statistically analyzed using multilevel gamma regressions on account of their skewed distribution.
A multilevel gamma regression exploring the effect of structured physical activity on social communication issues showed a significant Group and Timepoint interaction, χ2(1) = 5.82, p = .016, with children in the intervention group having significantly lower social communication issues after the intervention than before, b = 0.25, SE = 0.04, Z = 7.07, p <. 001. Repetitive behavior also had a significant interaction between Group and Timepoint, χ2(1) = 20.76, p < .001, where the repetitive behavior scores in the posttest were significantly lower than those in the pretest in the intervention group, b = 0.43, SE = 0.05, Z = 9.43, p < .001. This interaction between Group and Timepoint was also seen for mood- and anxiety-related behaviors, χ2(1) = 5.70, p < .017, with children in the intervention group showing decreased levels of mood- and anxiety-related behaviors following the intervention when compared to their pretest level, b = 0.41, SE = 0.06, Z = 6.82, p < .001. Similarly, there was a significant interaction between Group and Timepoint, χ2(1) = 51.05, p < .001, in the model for self-regulation issues, where the self-regulation issues in the pretest were significantly higher than those in the posttest in the intervention group, b = 0.47, SE = 0.03, Z = 14.12, p < .001. Other challenging behaviors also showed a significant interaction between Group and Timepoint, χ2(1) = 8.22, p = .004, with the challenging behaviors being significantly higher in the pretest than posttest in the intervention group, b = 0.26, SE = 0.06, Z = 4.58, p < .001. Visual representations of these effects are given in Figure 3.
Effect of Structured Physical Activity on the Acquisition of Skills
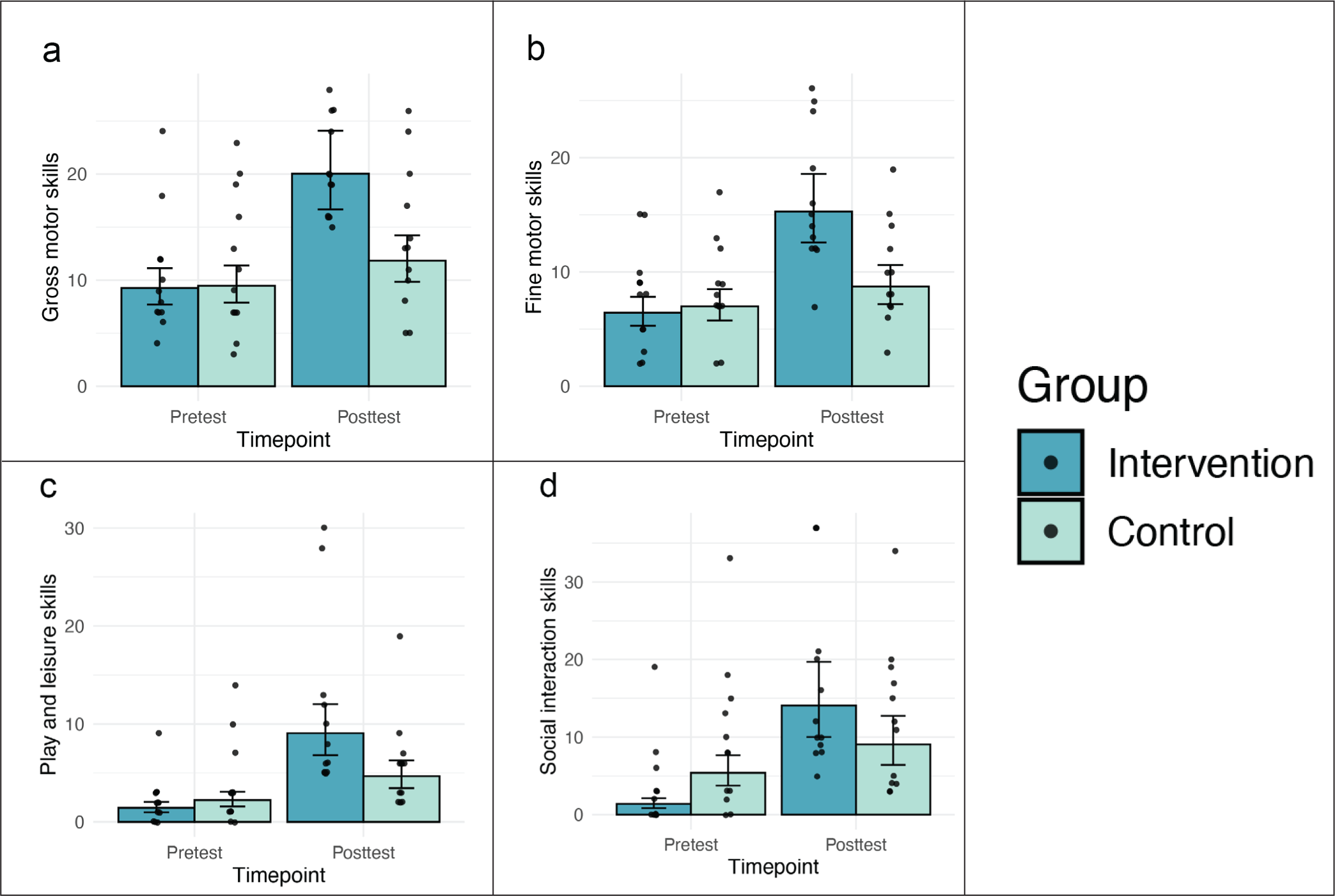
Skill acquisition was assessed using ABLLS-R. Of the 25 sets of skills assessed by ABLLS-R, only 6 sets were assessed in this study. Higher scores in these sections indicate more skills and, hence, are desirable. The effect of structured physical activity on these skills was analyzed using multilevel gamma regression.
The model exploring gross motor skill acquisition revealed a significant interaction between Group and Timepoint, χ2(1) = 33.83, p < .001, where the level of gross motor skills in the posttest was significantly higher than that in the pretest in the intervention group alone, b = 0.77, SE = 0.07, Z = 11.50, p < .001. Similarly, there was a significant interaction between Group and Timepoint, χ2(1) = 18.29, p < .001, in the model with fine motor skills as the outcome. Pairwise comparisons revealed that the fine motor skills in the posttest of those in the intervention group were significantly higher than their pretest level, b = 0.87, SE = 0.11, Z = 8.04, p < .001. The model looking at play and leisure skill acquisition also revealed a significant interaction between Group and Timepoint, χ2(1) = 20.37, p < .001, where the level of play and leisure skills in the posttest was significantly higher than that in the pretest, only among children in the intervention group, b = 1.60, SE = 0.15, Z = 10.,61 p < .001 . There was a similar significant interaction between Group and Timepoint, χ2(1) = 28.48, p < .001, in the model exploring the effect of structured physical activity on social interaction skills, where the posttest level of social interaction skills was significantly higher than the pretest level among those in the intervention group, b = 2.05, SE = 0.22, Z = 9.55, p < .001 . These effects are shown in Figure 4. Structured physical activity did not have a significant effect on motor imitation skills or request skills.
Effect of Structured Physical Activity on Sensory Processing Issues
Sensory processing issues were assessed by Sensory Profile 2, where higher scores indicated greater sensory processing issues. Multilevel gamma regression was used to analyze the effect of structured physical activity on sensory processing issues and behavioral responses to sensory issues (Figure 5).
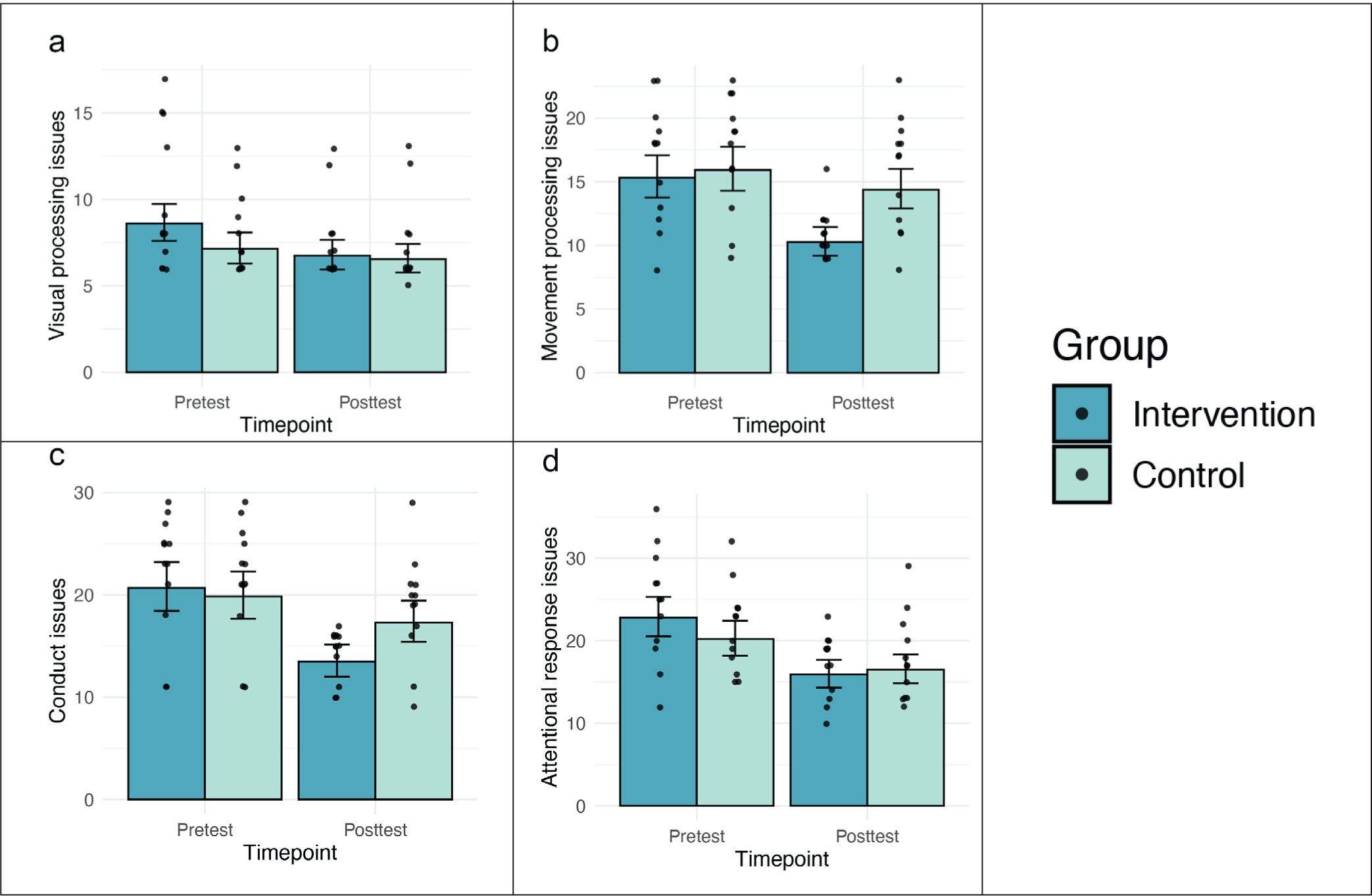
A significant interaction between Group and Timepoint, χ2(1) = 8.46, p = .004, was present in the model exploring visual processing issues. Pairwise comparisons revealed that the level of visual processing issues in the posttest was significantly lower than that in the pretest among children in the intervention group, b = 0.23, SE = 0.04, Z = 6.35, p < .001. The model exploring the effect of the intervention on movement processing issues also found a significant interaction between Group and Timepoint, χ2(1) = 20.32, p < .001, where the movement processing issues in the posttest of those in the intervention group were significantly lower than their pretest level, b = 0.39, SE = 0.05, Z = 8.55, p < .001. Models assessing the effect of the intervention on other sensory modalities did not reveal significant results.
Sensory Profile 2 also assesses conduct, social-emotional, and attentional responses to behavior. The model exploring the effect of structured physical activity on conduct revealed a significant Group and Timepoint interaction, χ2(1) = 28.05, p < .001, where the conduct issues in the posttest of those in the intervention group were significantly lower than their pretest level, b = 0.41, SE = 0.04, Z = 11.00, p < .001. Similarly, the model exploring the effect on attentional responses also revealed a significant interaction between Group and Timepoint, χ2(1) = 7.69, p = .006, where issues with attentional responses were significantly lower after the intervention than before it among children in the intervention group, b = 0.35, SE = 0.04, Z = 8.94, p < .001.
Discussion
The mean age of the children included in this study aligns with the mean age at which children present to this center for assessment. 23 Since the study sample did not have a sufficient number of girls, sex differences were not explored.
Compared to the children who engaged in unstructured physical activity, children who engaged in the structured physical activity program in this study showed greater reduction in behavioral issues such as social communication issues, repetitive behavior, mood- and anxiety-related behavior, self-regulation issues, and other challenging behavior. Similar findings have been reported by multiple reviews exploring the effect of physical exercise on ASD,24-26 which all point to the planned, repetitive, and thus predictable, nature of the structured physical activity to be the driving force behind the behavioral changes seen among autistic children engaging in structured physical activity.
Greater improvement in gross motor skills and play and leisure skills observed among the children in the intervention group of this study can be explained by the choice of activities included in the structured physical activity program, which directly targeted gross motor skills such as walking, jumping, and throwing and catching a ball, and included opportunities to develop play skills such as taking turns, playing simple ball games (during water-based play), and coordinating with peers. However, these children also showed greater improvement in fine motor skills, which are not directly targeted by the program. This suggests the possibility that improving gross motor skills will also improve fine motor skills. While previous studies have shown physical activity programs to improve motor skills among autistic children, many studies have not explored gross and fine motor skills separately.25,27
The group-based implementation of the intervention allows children to develop their social skills,28,29 such as eye contact, shared attention, and responding to social cues. This study shows that the children in the intervention group did demonstrate improvement in social communication and that this improvement was reflected in two outcomes: a reduction of social communication issues as measured by the parent-rated behavior checklist and an increase in the social interaction skills as measured by the therapist-rated ABLLS-R scores.
Few studies have explored, in detail, the effect of physical activity programs on sensory issues among autistic children. Since the intervention consisted of physical activities, improvement was expected in movement and body-positioning processing issues. However, of all the sensory modalities assessed in this study, improvements were seen only in visual and movement processing issues following the intervention period. The inclusion of colorful balls during water-based play, and the use of visual cues and modeling to train the children are both aspects of sensory integration therapy, which were incorporated in the intervention program and could have helped improve the visual processing issues of the children in the intervention group. 30 The absence of improvement in body-positioning processing issues could be due to the fact that the children had fewer issues with body-positioning processing to begin with, as indicated by lower pretest scores. The absence of significant improvement in other sensory processing issues could be attributed to the lack of diverse aspects of sensory integration in the intervention program. Systematically incorporating elements of sensory integration into this structured physical activity program could bring about improvement in multiple sensory modalities.
The overall reduction of behavioral and sensory issues in conjunction with the greater acquisition of motor, play, and social interaction skills among children in the intervention group aided these children to obtain a lower score, indicating lower ASD severity, in the CARS2 assessment, which assesses the severity of ASD based on the severity of behavioral, sensory, and cognitive symptoms of ASD.
Autistic children have a multitude of social, behavioral, and communication challenges and require a combined treatment approach incorporating different interventions, such as behavior therapy, speech and language therapy, play-based therapy, physiotherapy, occupational therapy, and nutritional therapy, that are designed to address their needs. However, while high-resource settings often have access to such a range of specialized services, countries with low-resource settings with fewer specialities often do not. In such places, it is often the case that only a few basic therapies are available, and that too to a small number of individuals at any given time. This leaves the rest of the children on a long waiting list. If all the interventions require extensive training to implement, parents also cannot step in to help their children. As such, there is a need to implement an effective intervention that can be easily implemented with minimal training, so that autistic children can receive some form of early intervention as they are waiting for more specialized therapies. Such an intervention would also facilitate the recruitment of parents as co-therapists to their children—a model followed by several institutes in low-resource settings. 31
As this study shows, structured physical activity effectively brings about changes in multiple aspects of ASD, including its severity, behavior issues, and skill acquisition. The structured physical activity program consists of simple activities that therapists, parents, or caregivers can easily learn to implement and do not require specialized training or sophisticated equipment, thus rendering it sustainable. It should preferably be implemented for a much longer period, spanning years, provided that children are periodically assessed by a professional and the activities are modified to suit the needs of the developing child. In addition to being customizable for each child, this program could easily be modified to incorporate cultural aspects of the community, such as traditional games involving physical activity. Including these cultural aspects would help the program resonate with local values and practices, enhancing engagement and participation. These features make a structured physical activity program suitable for expansion in low-resource settings to promote long-term benefits.
This study is among the first in our region to evaluate the integration of a parent-delivered structured physical activity program as an adjuvant to the routine therapy for autistic children. Unlike previous studies that examine physical activity in isolation, our research explored its role alongside ongoing therapies other than EIBI. As such, it is important to acknowledge that this intervention could merely have augmented the effects of the physiotherapy and occupational therapy the children were receiving. Nevertheless, structured physical activity warrants further exploration as a standalone early intervention as well as an adjuvant, as physical activity has been shown to produce beneficial effects not only at the behavioral level but also at the molecular level.32,33
Despite promising findings, this study is limited by its small sample size and the short duration of the intervention. Replicating the study with a larger sample size and an intervention duration of around 6 months would be beneficial to demonstrate the benefits more clearly. The influence of prior exposure to therapeutic activities on the observed outcomes might not have been systematically captured since the pre-intervention period was not considered here when assigning participants to groups. Similarly, since follow-ups beyond the post-intervention assessments were not included, the maintenance of the intervention’s effects over time was not captured. Future studies should consider the pre- and post-intervention periods to better understand the effects of the intervention. This study’s subject pool was conveniently selected based on their regular attendance at the center and the parents’ commitment to therapeutic adherence. Consequently, it is possible that the findings of this study generalize only to a sub-population with good therapeutic adherence. The effectiveness of structured physical activity as an adjuvant should be explored in a larger sample that includes various levels of compliance for better generalizability. Another limitation of this study is the lack of enough female participants to explore the sex effects on the benefits of structured physical activity. This should be addressed in future studies.
Conclusion
This study showed that the addition of structured physical activity to the repertory of therapies for autistic children will help decrease the severity of ASD, behavior issues, and visual and movement processing issues, while improving social interaction, motor, and play skills. Expanding this program in other low-resource settings can facilitate early intervention for ASD and make such interventions accessible to all.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We extend our sincere gratitude to the parents of all the children included in our study and to the staff of Mathavam, the center for neurodevelopmental disorders, for supporting the study. We would also like to thank Ms. S. Sadhana and Ms. T. Jana for their assistance in data entry, and Mr. M. Ramkumar for creating the diagrams of the physical activities used in this study.
Data Availability
Deidentified data will be available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was approved by the Ethics Review Committee of the Faculty of Medicine, University of Jaffna (J/ERC/23/152/NDR/0309) and the Sri Lanka Clinical Trials Registry Committee (SLCTR/2024/023). Ethical clearance was obtained before study initiation. Informed written consent was obtained from the parents of all participating children. Consent for publication was not applicable. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.