
Abstract
This case report presents the application of a client-centered approach integrating art and play therapy techniques to support an eight-year-old child exhibiting persistent withdrawal behaviors. Grounded in the Play Therapy Dimensions Model (PTDM), the intervention aimed to facilitate emotional regulation, social engagement, and self-expression. The therapeutic process was guided by non-directive principles, with creative modalities such as painting, sand tray play, and therapeutic storytelling forming the intervention’s core across 12 weekly sessions. Pre- and post-intervention assessments were conducted using the Strengths and Difficulties Questionnaire (SDQ), supported by structured therapist observations and parental interviews.
The child, initially characterized by anxiety, avoidance of peer interaction, and emotional inhibition, showed notable progress in emotional expression and social responsiveness. Artwork themes and metaphorical processing through storytelling reflected the child’s evolving internal world and emergent coping strategies. Neuropsychological and attachment-based theories were employed to interpret behavioral and expressive changes, highlighting the hemispheric processing of affect and the therapeutic utility of metaphor. The study underscores the effectiveness of client-centered play-based modalities in addressing internalizing difficulties among children and proposes the PTDM framework as a clinically useful structure for tailoring interventions.
Keywords
Introduction
Childhood withdrawal is a common internalizing problem that often goes unnoticed, yet it significantly affects emotional, social, and academic functioning. Studies estimate that internalizing symptoms—including anxiety, social withdrawal, and inhibition—affect approximately 10%-15% of school-aged children, with withdrawn children being particularly vulnerable to emotional dysregulation, peer exclusion, and low self-esteem.1,2 These children tend to avoid interaction, suppress emotional expression, and may struggle to verbalize internal distress, which makes traditional talk therapy, such as cognitive behavioral therapy or psychodynamic psychotherapy, less effective during early developmental stages.
Play therapy has emerged as a developmentally appropriate method for supporting children’s emotional growth. Through symbolic play and creative expression, children can externalize internal conflicts, rehearse adaptive behavior, and process unresolved emotions. Axline’s 3 non-directive, client-centered play therapy emphasizes acceptance, empathy, and the child’s autonomy in navigating therapeutic engagement. The Play Therapy Dimensions Model (PTDM), introduced by Yasenik and Gardner, 4 extends this framework by categorizing therapeutic interactions across conscious–unconscious and directive–non-directive quadrants. This structure offers therapists a dynamic and responsive approach while remaining grounded in child-led principles.
This case report explores the use of a client-centered, PTDM-informed approach to art and play therapy in the treatment of an eight-year-old girl presenting with persistent withdrawal behaviors. Through 12 weekly sessions using creative tools including drawing, sand tray play, and therapeutic storytelling, the intervention aimed to enhance emotional expression, build relational trust, and support self-regulation. The case is presented to illustrate how integrating creative modalities with the PTDM framework can facilitate therapeutic change in withdrawn children. It also contributes to the growing evidence base that underscores the relevance of play-based interventions in child mental health, particularly for children who cannot easily access or articulate their emotional experiences.
Case Presentation
Demographic and Referral Background
An eight-year-old girl, living in a joint family in an urban Indian setting, was referred for evaluation and management of withdrawn behavior by her parents and teachers, following increasing concerns about her social disengagement and limited participation in school activities. She is the eldest of two siblings, born to non-consanguineous parents. The father is employed, and the mother is a homemaker. The child lives with her extended family of approximately 20 members, although she is reportedly not close to anyone in the household.
Presenting Concerns
Teachers reported that the child displayed pervasive signs of withdrawal in the classroom. She isolated herself from peers, avoided conversations, and rarely responded even to direct instructions from teachers. She was often seen staring blankly and exhibited marked hesitation when approached. There were frequent observations of her freezing in social situations, avoiding eye contact, and speaking minimally, if at all. Rather than acting out or causing disruptions, she seemed to fade into the background; quiet, solitary, and often overlooked by those around her. Additionally, she took significantly longer to complete basic routines like eating lunch, often missing free-play time.
At home, the mother reported that the child was frequently nervous, cried easily, and was particularly fearful of her mother’s punitive behavior. The child preferred to spend time with her grandparents (living in a different city) and shared a positive relationship with her younger brother. Since early childhood, she had been described as timid and sensitive; however, her withdrawn behavior became markedly evident after the age of six, when she started formal schooling. Her mood was often subdued, and her interests were minimal, although reactivity was intact. Thus, the child had demonstrated persistent withdrawn behavior for approximately two years before presentation.
Psychosocial History
The child had no prior history of psychiatric consultation, therapy, or medication. There were no known medical or neurological concerns. Her developmental milestones were reported to be normal. No significant trauma history was disclosed by caregivers during the intake process. The family dynamics indicated possible emotional neglect or authoritarian discipline, which may have contributed to her internalizing symptoms. A separate psychiatric evaluation was not pursued because initial screening and clinical history did not suggest the presence of a psychiatric disorder requiring such assessment. Additionally, the parents expressed a preference to continue with therapeutic interventions without psychiatric consultation at this stage.
Ethical Considerations
Informed consent for both therapeutic intervention and the publication of this case report was obtained from the child’s legal guardians. All identifying information has been anonymized, and the child is referred to using a pseudonym. The therapist adhered to ethical guidelines for working with minors in clinical settings, including ensuring the child’s emotional safety and voluntary participation. Ongoing clinical supervision was maintained throughout the therapeutic process to support ethical and reflective practice.
Therapeutic Formulation and Intervention
Formulation and Theoretical Framework
The therapeutic understanding of the case drew upon psychodynamic, attachment, and neurobiological models to explain the child’s persistent social withdrawal, emotional constriction, and difficulty with verbal expression. The child’s relational history revealed fear of her mother’s punitive behavior, a lack of emotional safety within the home, and a preference for solitary activities, suggesting disrupted early attachment and possible emotional inhibition. According to Winnicott, 5 the absence of a “holding environment” in early development impairs a child’s capacity to play, which is essential for emotional integration and self-development. Balint’s 6 notion of the “basic fault” further contextualizes the child’s retreat from interpersonal contact as a response to perceived relational threat.
John Bowlby’s 7 model of avoidant attachment provides a useful lens to understand the child’s reluctance to seek help or display emotional needs. Neurobiological literature supports these observations: lateralized emotional processing in the brain suggests right-hemisphere dominance in withdrawal behaviors and negative affect, 8 which was reflected in the child’s left-sided imagery in art and the predominance of solitary themes.
Given the child’s difficulties with verbalization, a client-centered play therapy approach rooted in Axline’s 3 non-directive model was adopted. The PTDM 4 was used to guide the therapist’s moment-to-moment decisions across different therapeutic quadrants—beginning with non-directive, unconscious work and gradually progressing toward co-facilitated and active utilization strategies.
Intervention Overview
The therapeutic process was structured across 12 weekly sessions (45 minutes each) and divided into three clinical phases.
Initial phase (sessions 1–4): The focus was on establishing trust through non-directive, unconscious-level interventions. The child entered the space quietly, avoided eye contact, and confined herself to a small area of the room. She consistently chose watercolor painting, using fine, gentle strokes. Her body language was guarded, often slouched or tense, and she rarely initiated interaction. The therapist remained silently present, following Axline’s 3 principle of unconditional acceptance and allowing the child full autonomy in choosing materials and pace. The artwork frequently depicted natural elements (trees, clouds, flowers), but always included a solitary girl figure placed to the left side of the page, reflecting themes of emotional distancing and withdrawal. These sessions aimed to create a safe holding environment and gently invite symbolic expression.
Middle phase (sessions 5–9): As trust deepened, the therapist gradually introduced structured, yet still client-led, techniques such as sand tray play and therapeutic storytelling. The child began to explore the sand tray, arranging zoo and park scenes using miniatures. She also responded positively to the therapist-created metaphorical story, “Betty the Cloud,” which subtly mirrored her emotional struggles and relational fears (The full narrative is presented in Box 1)). Following this, the child crafted a paper handbag called “Treasure of Cloud,” filled with colorful beads, a symbolic act of integrating affective experience. Her engagement increased noticeably; her posture became more upright, brief eye contact occurred, and she verbalized simple responses related to the story themes. Through metaphor, the child appeared to process her anxiety and internal conflict more safely.
Termination phase (sessions 10–12): The therapeutic stance shifted toward co-facilitation. The child continued painting, but now included brighter colors and began to depict two characters instead of one. Her body language became visibly more relaxed and expansive, and she smiled more often. These subtle shifts indicated emotional softening and emerging interpersonal openness. The therapist used gentle reflections to reinforce her growth and prepared her gradually for the end of therapy. The space, once a site of quiet containment, became a site of cautious expression and emerging connection.
Outcomes and Assessment Summary
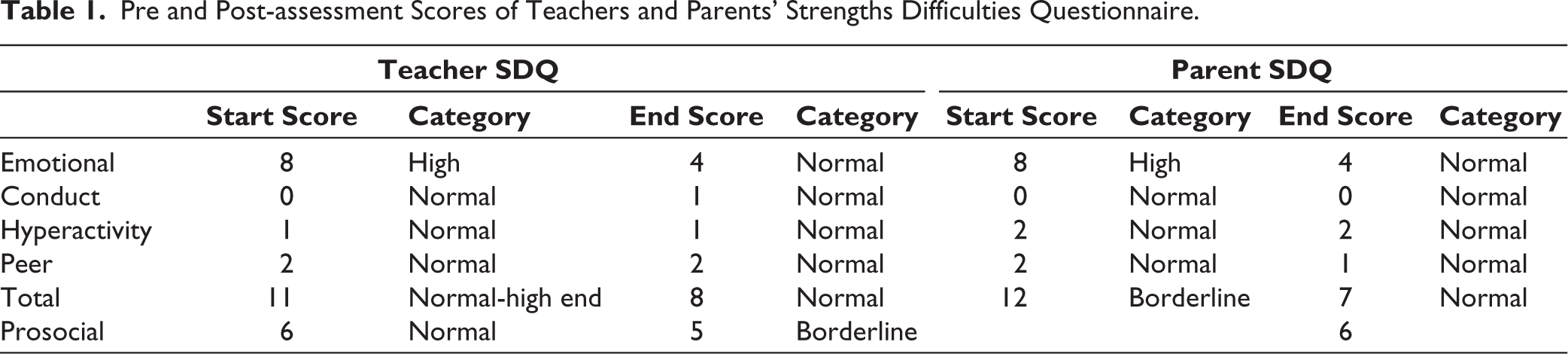
Therapeutic outcomes were assessed using a combination of developmental screening, standardized measures, session observations, and qualitative analysis of the child’s behavior and artwork. Neurodevelopmental disorders were ruled out based on developmental history, school feedback, repeated behavioral observations across sessions, and administration of the Developmental and Psychosocial Checklist (DPCL), which did not indicate features suggestive of autism spectrum disorder, attention-deficit/hyperactivity disorder, or other neurodevelopmental conditions. The Strengths and Difficulties Questionnaire (SDQ) was then administered pre- and post-intervention to both the parent and teacher, providing insight into multiple domains of functioning (Table 1).
Pre and Post-assessment Scores of Teachers and Parents’ Strengths Difficulties Questionnaire.
Therapeutic Story: “Betty the Cloud.”
BETTY THE CLOUD
Betty woke up in the morning from sleep. She was still dreadfully sleepy and felt that her body was so heavy. She looked dark and dull. She carried lots of waterdrops inside and she could only move very slowly.
All her friends were far ahead of her. She moved slowly with lots of pauses.
On her way, she looked at the shining sun. The sun smiled at her and asked her to come nearby. The sun offered help to her. But Betty was very scared and nervous of going to the sun. Betty changed her direction and continued moving.
There was a wonderful surprise for Betty. Rainbow! Little Betty loved colors. She reached fast toward the Rainbow. She was thrilled. She put both her hands into all the colors and tinted all over the sky which she loved doing.
The colors started fainting and the Rainbow waved at her and said Goodbye. It started raining suddenly. That was disappointing for some time. But Betty felt so nice about it and she started moving when she remembered that she must reach out to her friends.
And there came a group of birds…. they were flying up and up by squawking. Betty started trembling by looking at them. They were flying toward her. She closed her eyes and ears as the noise was getting closer and closer. They just passed by her and nothing happened to her. There was a long sigh from Betty.
She continued to move slowly. By looking down she saw a thirsty tall plant in a dry land. The plant was desperately looking at her pleading to Betty for some shade and water. The plant begged “I can’t stand hunger anymore; can you please help me out of this.” Betty felt sad but at the same time she was scared to give water.
The wind was trying to hold and help Betty to move. This is a puzzling situation for Betty. Finally, with lots of courage Betty decided to give shade and then water to the plant.
Betty showered a bit of water to the plant. The Plant felt happy. Betty felt lighter and thinner after pouring water. Betty was so glad that she could move better now.
Betty started singing and humming “In and out and out and in, Quick as a flash I jump and spin.” Betty floated in the sky and was happy because of her new discoveries in the journey.
A self-report assessment was not undertaken because the child’s engagement with the therapist was minimal in the initial sessions, both verbally and nonverbally, which limited the feasibility of administering such tools. In addition, given her age (8 years) and her withdrawn presentation, the validity and reliability of a self-report measure would likely have been compromised.
At baseline, the child presented with high scores in the emotional problems domain and borderline scores on overall difficulties, consistent with observations of social withdrawal, anxiety, and affective inhibition. Post-therapy scores reflected a marked improvement: both parent and teacher ratings showed a reduction in emotional symptoms from the “high risk” to the “normal” range. While conduct and hyperactivity scores remained in the normal range throughout, this was expected given the child’s internalizing presentation. Notably, the teacher’s prosocial rating declined slightly, shifting from “normal” to “borderline,” which may reflect a cautious re-entry into peer interaction rather than true regression.
The child’s qualitative progress was evident through shifts in behavior, posture, engagement, and creative expression. Initially, she exhibited restricted affect, avoided eye contact, and produced artwork featuring solitary figures in muted tones. As therapy progressed, she demonstrated increased willingness to explore new materials (e.g., sand tray, crafts), more animated affect, and artwork that incorporated multiple figures and vibrant colors. Her final painting featured two girls holding hands, an image that contrasted sharply with her earlier isolative themes and suggested cognitive-emotional movement toward connection.
The story-based metaphor (“Betty the Cloud”, (refer Box 1))) also served as a turning point, allowing the child to externalize and symbolically process her emotional burdens. After this intervention, she began to show increased spontaneity, including crafting a paper bag labeled the “Treasure of Cloud,” and engaging in shared affect with the therapist through eye contact and spontaneous speech.
Feedback from parents and teachers further corroborated these gains; the child initiated play with friends, communicated more openly, expressed feelings to teachers and peers, and showed progress in academic participation.
Overall, the child made measurable gains in emotional regulation, symbolic expression, and social responsiveness. While continued support was recommended to consolidate these gains, the 12-session intervention demonstrated the potential of PTDM-informed, client-centered art and play therapy in supporting emotional development in withdrawn children.
Discussion
This case highlights the therapeutic value of client-centered, creative modalities for a child experiencing significant social withdrawal and emotional inhibition. The intervention, guided by the PTDM, enabled the therapist to tailor engagement across developmental, emotional, and cognitive levels without compromising the child’s sense of safety or autonomy.
Children with internalizing symptoms often find it difficult to articulate emotions through verbal language alone. As supported by Landreth 9 and Oaklander, 10 play therapy creates a symbolic space where children can externalize emotions, test new relational patterns, and process experiences nonverbally. In this case, the child’s progression from solitary painting to symbolic sand tray scenes and eventual metaphor engagement mirrored her internal movement from fear and inhibition to tentative connection and affective expression.
The PTDM framework 4 was central in structuring this therapeutic progression. Initially, the therapist operated within the nondirective-unconscious quadrant, offering silent presence and freedom of choice. As trust deepened, the intervention moved toward active utilization, incorporating structured metaphor and storytelling. The child’s responsiveness to “Betty the Cloud” supports the role of therapeutic metaphor as a bridge between implicit affective experience and conscious meaning-making.11,12
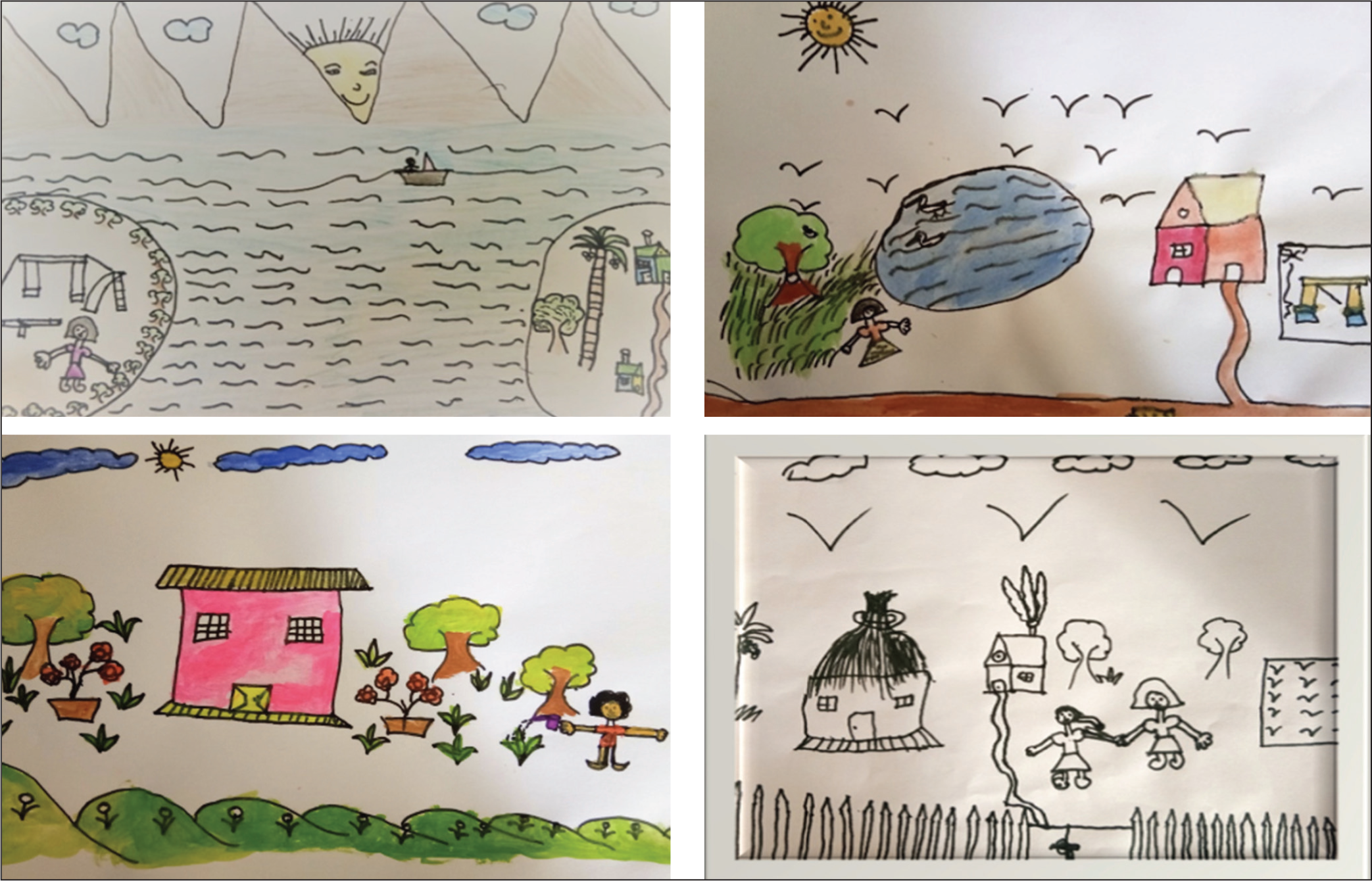
Neuropsychological theory further supports these clinical observations. The child’s early artwork (refer Figure 1) displayed left-sided imagery and solitary figures, consistent with right-hemisphere activation, which has been linked to withdrawal and negative affect.8,13 As therapy progressed, her images shifted in valence and spatial use, aligning with evidence that left-hemisphere processing and approach motivation are associated with emotional engagement and positive affect. 14
Image of Drawing in the First, Second, Third, and Last Sessions.
The case also supports findings from empirical studies. Haeyen et al. 15 observed that art therapy interventions improve emotion regulation and self-concept among clients with personality vulnerabilities. Similarly, Kõiv and Kaudne 16 documented reduced emotional symptoms in institutionalized girls following arts-based therapy. These outcomes align with the improvements seen here, especially in SDQ emotional and total scores.
Importantly, the therapy process required the therapist to tolerate silence, respect spatial boundaries, and allow the child to lead. This aligns with Axline’s 3 principle of acceptance, where the therapist offers structure without intrusion. The shift from non-directive presence to co-facilitation was not linear, but guided by the child’s readiness, as reflected in her engagement with materials and metaphors.
Clinical Implications
This case underscores the importance of flexible, developmentally appropriate interventions for children with internalizing problems. The integration of symbolic expression, metaphor, and a client-led structure enabled therapeutic movement without requiring verbal disclosures. The PTDM framework may serve as a useful clinical guide for tailoring therapist responses to emotional readiness, particularly in culturally sensitive contexts where emotional expression may be further inhibited.
Conclusion
This case demonstrates the effectiveness of a client-centered, PTDM-guided art and play therapy intervention for a child with pronounced social withdrawal and emotional inhibition. Over 12 sessions, the child progressed from nonverbal, solitary behavior to more expressive, engaged, and socially responsive functioning. Improvements were evident in both behavioral observations and pre-post SDQ scores. The integration of non-directive play, creative expression, and therapeutic metaphor allowed the child to symbolically process emotions that could not be accessed verbally. This approach underscores the clinical utility of combining structured therapeutic models like PTDM with developmentally appropriate creative modalities, particularly for children with internalizing presentations who may not respond to traditional talk-based methods.
Footnotes
Acknowledgements
Dr. Sherin P Antony, Associate Professor, School of Psychological Sciences, Christ University, India. Dr. Deviga Subramani, Assistant Professor, School of Psychological Sciences, Christ University, India.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The author has discussed with the parents regarding the sharing of the clinical data of the client for supervision and a research project without revealing the identity of the client, and consent was taken from the parents. The Research Conduct and Ethics Committee of Christ University has reviewed the study.