
Abstract
Purpose of the Review:
Attention-deficit/hyperactivity disorder (ADHD) is increasingly recognized as a neurodevelopmental disorder that persists into adulthood, associated with functional impairments and psychiatric comorbidities. Global estimates range from 2% to 7%, with higher rates reported in low- and middle-income countries (LMICs). In India, where a large proportion of the population is young, understanding the prevalence and clinical profile of adult ADHD is vital for public health. This article aims to summarize the existing evidence on adult ADHD in India, focusing on prevalence patterns, clinical correlates, and methodological challenges.
Collection and Analysis of Data:
Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, a systematic review was conducted using PubMed and Google Scholar up to August 2025. Original studies reporting prevalence or clinical features of adult ADHD in India were included, while reviews, case reports, and studies of Indian populations abroad were excluded. Twenty-four studies were identified and synthesized narratively with attention to conceptualization, prevalence, comorbidities, and cultural influences.
Conclusions:
Prevalence estimates varied across settings. Community and student samples reported rates between 5.5% and 23.3%, with the inattentive subtype consistently dominant. Clinical and substance use disorder (SUD) populations demonstrated higher prevalence, ranging from 18% in opioid-dependent inpatients to 62% in alcohol-dependent cohorts. Comorbidities commonly included depression, anxiety, bipolar disorder, and substance dependence, with ADHD amplifying illness severity and relapse risk. Gender disparities were evident, with women often underdiagnosed due to internalizing presentations. Methodological gaps included reliance on self-report tools, limited retrospective childhood confirmation, and a lack of intervention trials. Adult ADHD in India shows higher prevalence and distinctive cultural influences compared with global estimates. Standardized diagnostic protocols, gender-sensitive approaches, and culturally adapted interventions are urgently needed to improve recognition and care.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by persistent symptoms of inattention, hyperactivity, and impulsivity. 1 Historically, ADHD was conceptualized as a childhood-limited disorder, with the assumption that symptoms remit during adolescence. 2 However, longitudinal studies over the past two decades have challenged this view, showing that ADHD frequently persists into adulthood and, in some cases, may even first emerge later in life.3,4 Previously, ADHD was recognized as a childhood- onset condition that persisted into adulthood, referred to as persistent ADHD, whereas cases emerging later in life were characterized as late-onset ADHD. 5 While the persistence model is well established, 6 some researchers debate the validity of late-onset ADHD. Some argue that such cases may reflect previously undetected childhood ADHD or the influence of comorbidities7,8 while others contend that late-onset ADHD is a distinct subtype influenced by environmental and developmental triggers.5,9,10 This conceptual debate reflects the heterogeneity of ADHD and its interaction with psychosocial, biological, and cultural factors.11,12
The global prevalence estimates suggest that approximately 2%–3% of adults meet criteria for persistent ADHD, while 5%–7% may present with symptomatic ADHD depending on diagnostic criteria and methodology. 13 A systematic review and meta-analysis highlighted that prevalence estimates are generally higher in low- and middle- income countries (LMICs) than in high-income settings. 14 For instance, persistent and symptomatic adult ADHD were estimated at 3.25% and 7.66% in high-income countries, compared with 8% and 10.68% in LMICs. 14
With nearly 65% of India’s population below 35 years, understanding adult ADHD is especially relevant, particularly as Indian studies report a higher prevalence than Western countries.15–18 Indian studies report relatively high prevalence of adult ADHD, such as 14% among college students in Delhi-National Capital Region (NCR) and nearly 25% among fishermen in South India. 20 Despite such findings, adult ADHD remains under- recognized in clinical practice.21,22 Limited awareness among healthcare providers, diagnostic overshadowing by comorbidities, and cultural stigma surrounding mental health contribute to widespread underdiagnosis of adult ADHD in India, resulting in significant psychosocial and economic burden.21,23
The clinical presentation of adult ADHD differs from childhood forms. While hyperactivity is prominent in early life, these symptoms often diminish with age; meanwhile, inattentive symptoms, disorganization, impulsivity, and emotional dysregulation persist, or become more pronounced.24,25 Adults with ADHD frequently report difficulties with time management, sustaining attention in occupational tasks, maintaining relationships, and regulating emotions.26,27 Comorbid conditions such as depression, anxiety, bipolar disorder, and substance use frequently co-occur, complicating diagnosis and worsening functional impairments.28,29
Despite this burden, adult ADHD remains underdiagnosed and undertreated in India. Limited India-specific research, lack of culturally adapted diagnostic tools, and normalization of ADHD-like symptoms within Indian society contribute to delayed diagnosis, often until comorbid psychiatric or medical conditions become evident.21,28,30
In our previous systematic review, 9 we examined the prevalence of adult ADHD in India and demonstrated that the disorder is not uncommon in young adults or clinical populations. Building on that foundation, the present review extends the scope to explore not only prevalence but also the conceptual underpinnings and clinical profiles of adult ADHD, with attention to symptomatology, comorbidities, functional impairments, and cultural considerations. By situating Indian findings within the global evidence base, this review aims to provide a comprehensive synthesis and highlight key priorities for future research, clinical practice, and policy.
Methodology
Study Design
This study is a systematic review conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines. The review exclusively focused on studies conducted in India that examined the concept, prevalence, and clinical profile of adult ADHD. The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; Registration ID: CRD420251142924).
Search Strategy
An electronic search was conducted, encompassing all studies published up to August 2025, using PubMed and Google Scholar. The search terms and syntax used for PubMed were (adult ADHD OR ADHD OR attention-deficit disorder with hyperactivity OR hyperactivity disorder OR attention-deficit hyperactivity disorder OR ADHD attention-deficit hyperactivity disorder OR ADDH OR hyperkinetic disorder OR attention-deficit disorder hyperactivity OR attention-deficit disorders hyperactivity OR child attention-deficit disorder OR hyperkinetic syndromes OR syndromes hyperkinetic OR hyperkinetic syndrome adult OR India*) AND (adult ADHD OR ADHD OR attention-deficit disorder with hyperactivity OR hyperactivity disorder OR attention-deficit hyperactivity disorder OR ADHD attention-deficit hyperactivity disorder OR ADDH OR hyperkinetic disorder OR attention-deficit disorder hyperactivity OR attention-deficit disorders hyperactivity OR child attention-deficit disorder OR hyperkinetic syndromes OR syndromes hyperkinetic OR hyperkinetic syndrome adult) AND (Prevalence) AND (India*). Further articles were searched on Google Scholar, and the search terms related to adult ADHD, prevalence, and epidemiology in India were used to look for appropriate results. The search terms used were (“adult ADHD” OR “adult attention-deficit/hyperactivity disorder”) AND (India OR Indian) AND (prevalence OR epidemiology OR “clinical profile”)
Inclusion and Exclusion Criteria
The following inclusion criteria were considered for selecting articles: (a) All original articles on the prevalence of adult ADHD in India, (b) studies that have employed a categorical diagnosis of ADHD. The exclusion criteria for the review were as follows: (a) Studies on the prevalence of adult ADHD among Indians not residing in India, (b) case reports, editorials, and reviews; and (c) studies with incomplete or unclear information regarding diagnostic tools.
Result and Discussion
Study Selection and Characteristics of Included Studies
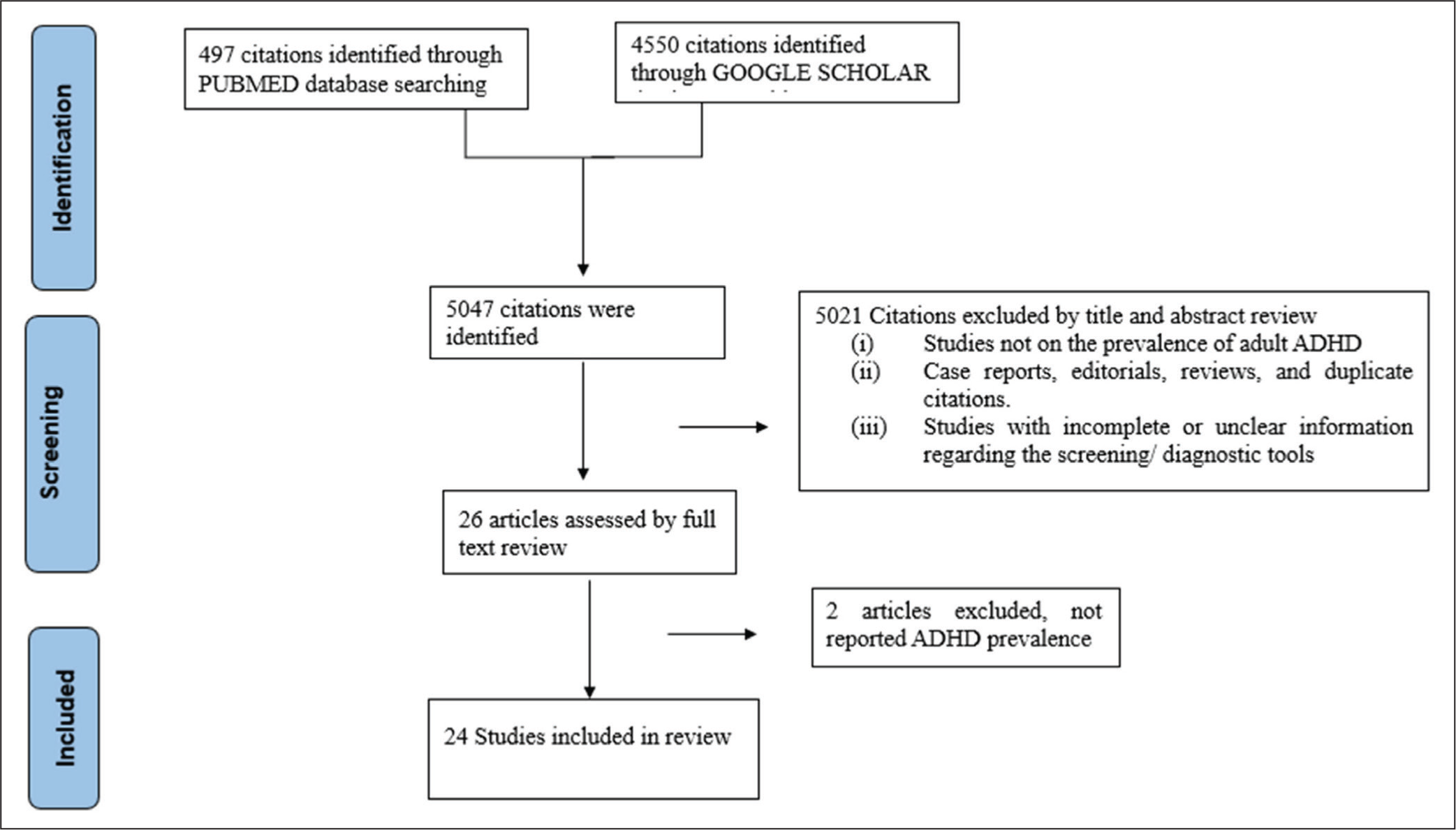
The literature search initially yielded 5047 records, including 497 from PubMed and 4550 from Google Scholar. After removal of duplicates and screening by title and abstract, 24 studies met the inclusion criteria (Figure 1).
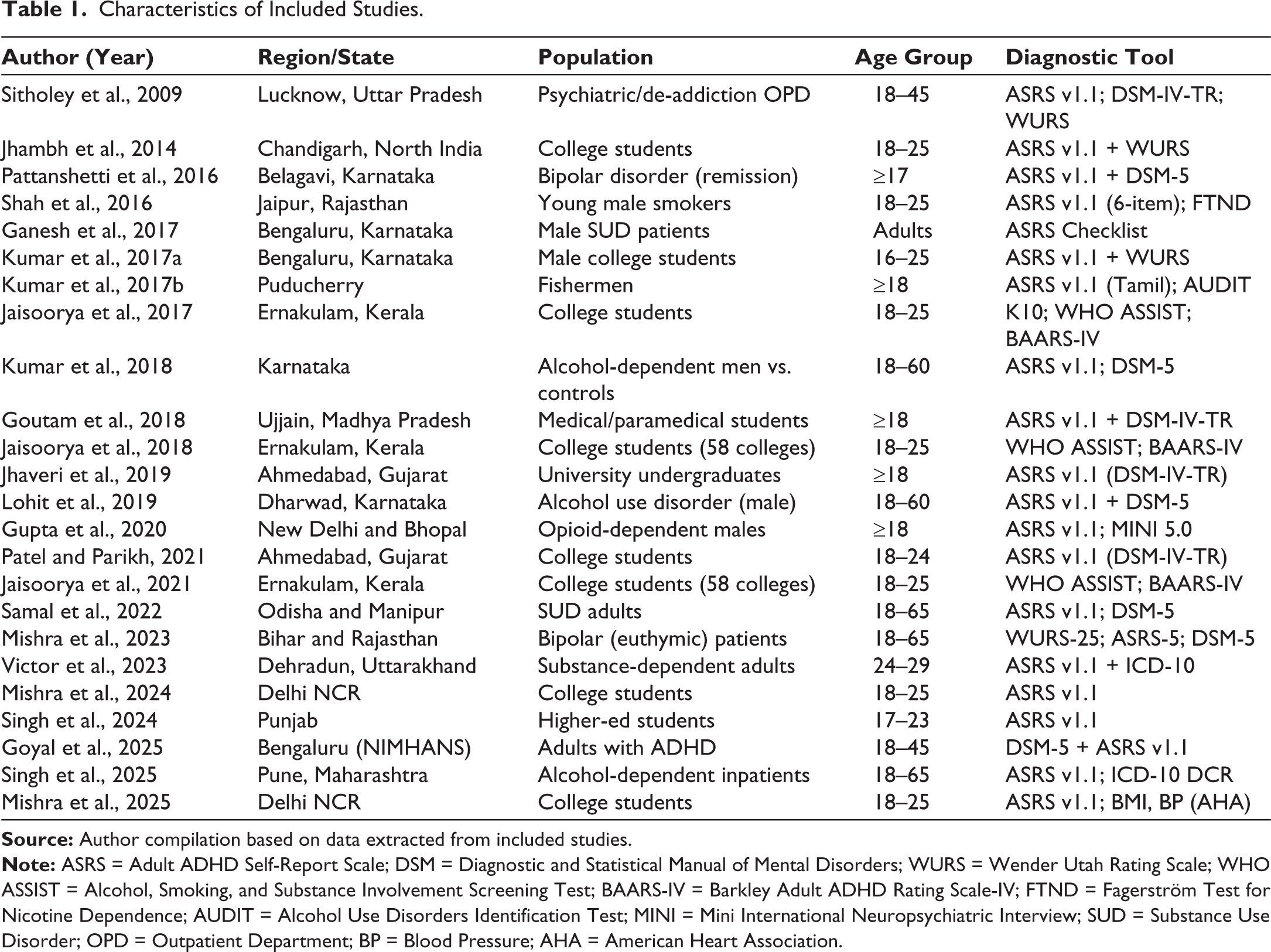
The included studies were conducted between 2000 and 2025 across multiple Indian regions, such as Delhi NCR, Karnataka, Kerala, Gujarat, Rajasthan, and the North-East.19,20,31–52 Samples included community, student, and clinical groups (psychiatric and substance use populations) (Table 1). Most studies were cross-sectional in design and employed validated instruments, most commonly the Adult ADHD Self-Report Scale (ASRS v1.1), followed by the Wender Utah Rating Scale (WURS) and Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV/DSM-5-based diagnostic interviews.31,44,47,50
Characteristics of Included Studies.
Concept of ADHD
Indian research presents a complex understanding of ADHD in adulthood. While international literature now defines ADHD as a lifespan neurodevelopmental disorder. Indian research shows an uneven representation of this global trajectory. Among student and community populations, ADHD has often been examined through the lens of functional outcomes. Few studies employed the ASRS v1.1 to assess current symptoms in college students, linking them with academic stress, sociodemographic variation, and regional background.19,39 Some studies similarly relied on symptom checklists, treating ADHD primarily as a functional construct rather than a diagnostic entity.33,42
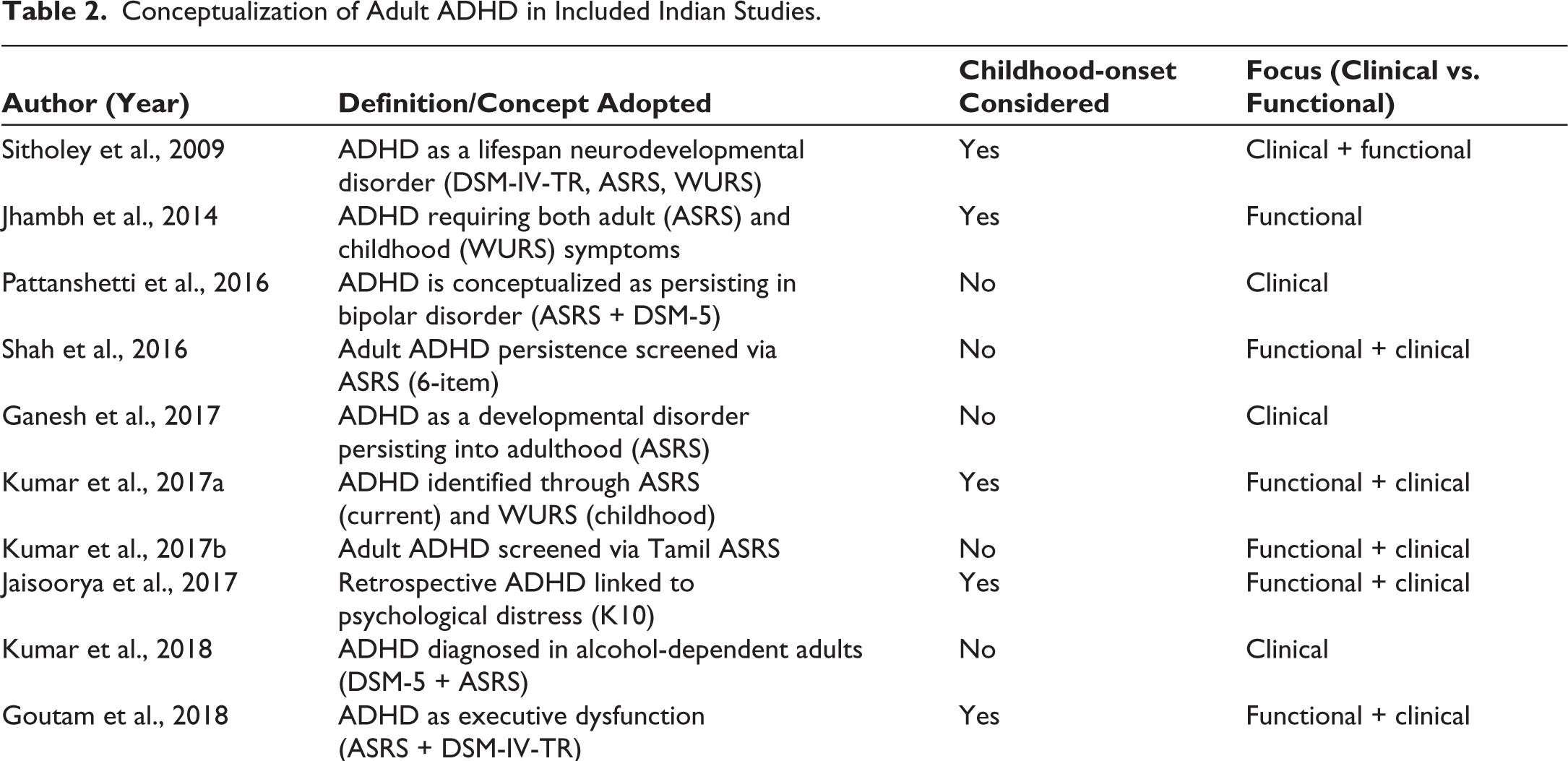
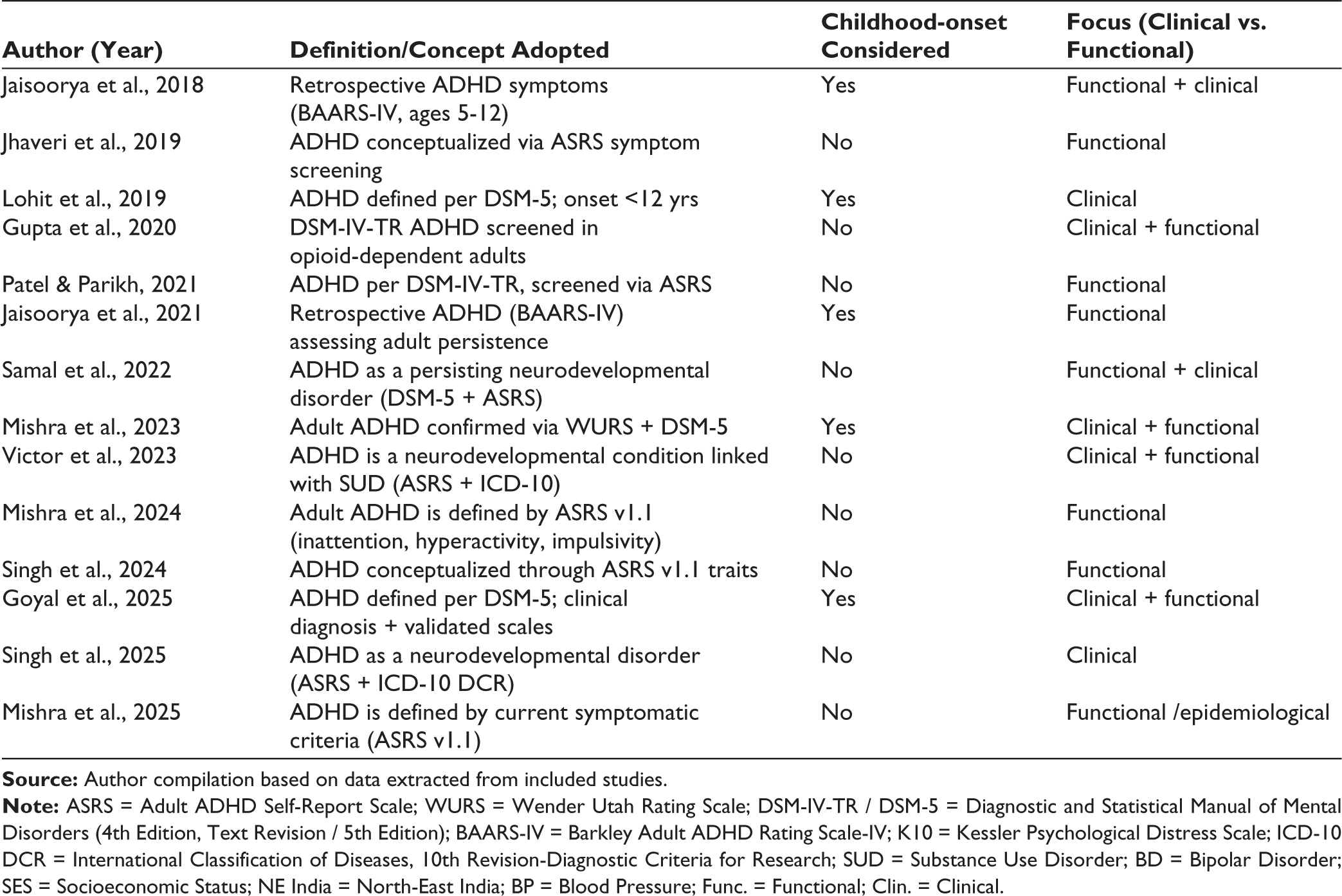
Only a few studies incorporated retrospective childhood measures such as the WURS or Barkley Adult ADHD Rating Scale-IV (BAARS-IV), thereby aligning more closely with DSM-based requirements31,32,44,47 (Table 2). Overall, the absence of systematic childhood-onset confirmation in most of these investigations demonstrates a gap between Indian research practices and international nosology. Yet these studies highlight important functional consequences of ADHD in young adults, ranging from poor academic performance and emotional instability to association with behavioral factors such as substance use and unsafe sexual practices.
Conceptualization of Adult ADHD in Included Indian Studies.
In parallel, another set of studies examined the comorbid conditions associated with ADHD, underscoring its broader clinical and psychosocial implications beyond functional impairments. The studies on diagnosed ADHD individuals revealed a persistent co-occurrence of ADHD with alcohol use.36,37,40,51 In alcohol-dependent populations, ADHD has been portrayed as a psychiatric comorbidity with direct implications for illness trajectory. Similarly, studies also show a strong association of ADHD with other substance use disorders (SUDs), including heroin, cannabis, and opioid.35,41,46,49
Beyond addiction, ADHD has also been examined as a modifier of psychiatric illness. A study reported ADHD in patients with bipolar disorder in remission, 34 while another study found that comorbid ADHD predicted earlier illness onset, higher episode frequency, and increased suicidality. 47 Another study further emphasized developmental continuity by documenting childhood-onset in more than 90% of clinically diagnosed adult ADHD patients in a tertiary-care setting. 50
Indian research reveals two conceptualizations of ADHD. Community studies view it as a functional, symptom- based construct linked to academics or behavior, while clinical studies treat it as a DSM/ICD-defined disorder with comorbidity and prognosis. However, inconsistent methods and the lack of culturally validated tools persist. Most studies rely on untranslated ASRS or WURS scales, and only one study used a Tamil version of the ASRS, highlighting the need for psychometric adaptation in India. 20
These findings indicate that ADHD symptoms are common among Indian students but are often normalized as outcomes of academic or lifestyle stress.19,39 This functional interpretation reflects a broader trend in low and middle-income settings, where psychological distress is attributed to external pressures rather than neurodevelopmental causes. Consequently, adult ADHD remains under-recognized, limiting clinical referrals and targeted interventions. 21 The developmental vulnerability hypothesis is supported, suggesting that impulsivity and reward dysregulation in ADHD increase susceptibility to addictive behaviors. Cultural factors such as permissive drinking norms in fishing communities or easy access to opioids in the North East further intensify these risks. Moreover, ADHD interacts with affective and behavioral systems, shaping illness trajectories and contributing to diagnostic overshadowing in psychiatric settings. The most distinctive contribution of Indian research lies in its cultural contextualization. Studies among migrating students in Delhi, reflecting cultural and environmental differences between North and South India that create adaptation challenges 19 along with fishermen in Puducherry, 20 military personnel in Pune, 51 and North-Eastern populations, illustrate this diversity. 46
Prevalence of ADHD
The prevalence of adult ADHD in India has been examined across diverse populations, including students, community samples, SUD patients, alcohol-dependent cohorts, and psychiatric populations (Table 3). Estimates vary widely, reflecting methodological differences, population characteristics, and contextual influences.
Prevalence of Adult ADHD Reported in Indian Studies.
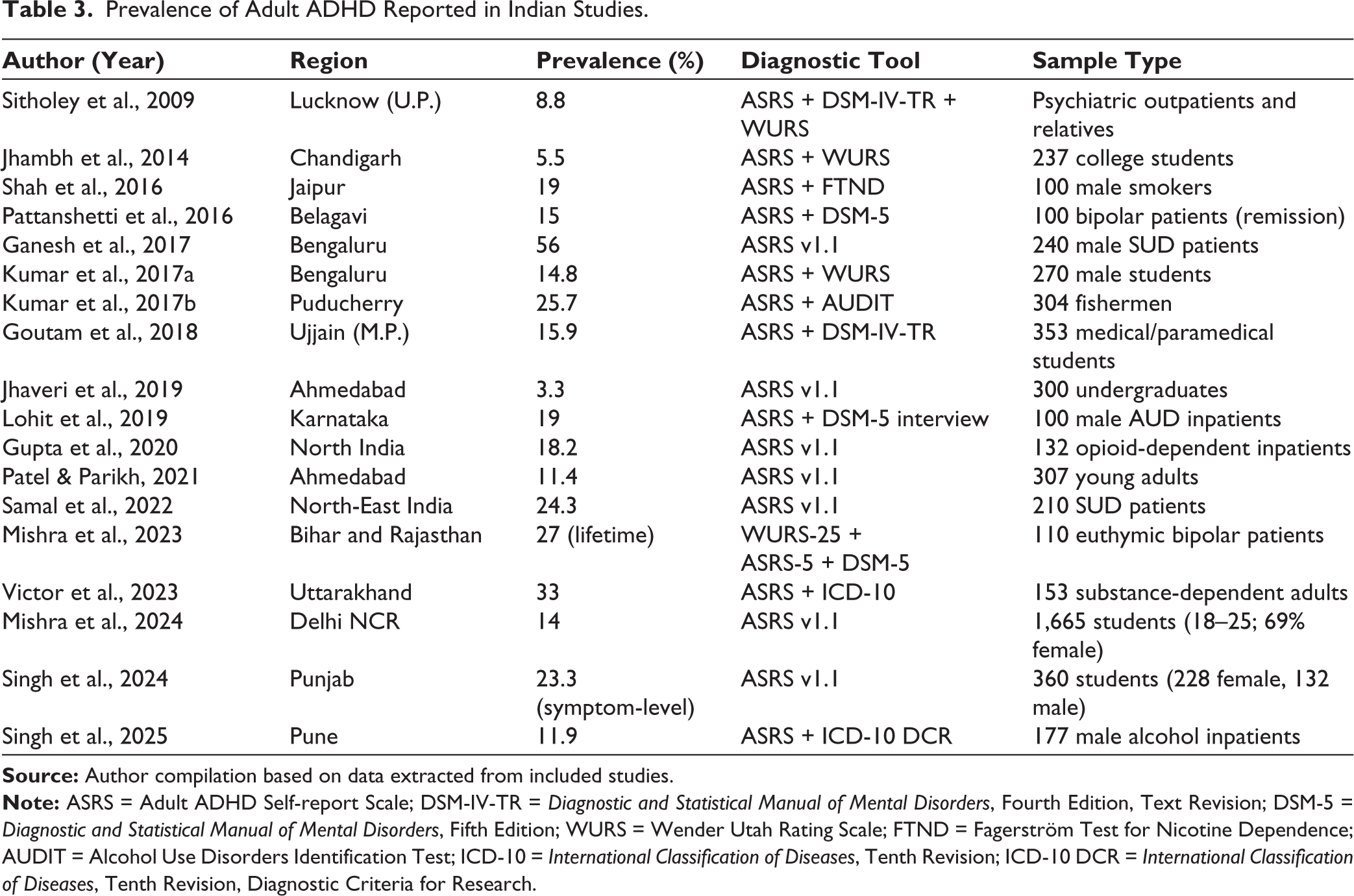
In community and population-based studies, prevalence ranged from 5.5% in Chandigarh to 23.3% in Punjab.32,52 Mid-range estimates included 14% in Delhi-NCR 19 and 15.9% in Ujjain. 38 Across community-based studies, the inattentive subtype was consistently dominant; in Delhi, nearly two-thirds of ADHD cases belonged to this subtype. 19 These rates are broadly higher than those reported from Western population-based studies, indicating possible contextual amplification, or diagnostic overestimation.
Functional impairments were common, including emotional instability, low self-esteem, poor academic performance, and risky sexual behaviors,32,37 among individuals with ADHD.32,37 Interestingly, higher maternal education and South Indian origin were associated with increased ADHD risk, whereas low socioeconomic status appeared protective in Delhi students, possibly reflecting reduced academic competition or differing cultural expectations. 19 MBBS students in Ujjain showed a higher prevalence compared to physiotherapy and nursing peers. 38 These findings suggest that ADHD in young adults is shaped not only by symptom profiles but also by sociocultural and academic contexts, such as migration-related stress and competitive education environments. Studies conducted among students or in community settings appear to yield higher ADHD prevalence when compared with the global estimates, ranging from 2.5% to 5%.4,14
While student and community studies depict ADHD as relatively common, clinical populations show even higher prevalence and stronger associations with comorbidities. In alcohol and SUD populations, prevalence estimates were markedly higher, ranging from 18.2% among opioid- dependent inpatients to 62% among alcohol-dependent men in Karnataka. 41 A study reported that 56% of SUD patients screened positive for ADHD symptoms, with early-onset dependence groups showing significantly higher ADHD prevalence. 35 Another study reported 33% prevalence in substance-dependent adults, with cannabis users most affected (47.6%), 49 while another study found 24.3% prevalence in North-East India, with polysubstance users reaching 65%. 46 Clinical remarks across studies reveal that ADHD-positive patients were younger, consumed more alcohol daily, relapsed earlier, and had higher psychiatric comorbidity.40,52 In Puducherry, fishermen showed a prevalence of 25.7%, doubling to 40% in alcohol-dependent subgroups, reflecting the impact of occupational stress and a pervasive alcohol culture. 37 In North-East India, cultural acceptance of alcohol and opioids shaped outcomes, producing higher prevalence rates. 46 These findings align with global pooled estimates of 23% for SUD populations. 53 Meanwhile, in a few studied populations in India, the prevalence exceeded, underscoring how social environments and addiction pathways intensify ADHD expression. 54
Methodological differences cause wide variation across Indian studies. Most used the ASRS v1.1 for screening, while a few included retrospective tools such as WURS or BAARS-IV, or conducted structured diagnostic interviews. In studies using retrospective confirmation, such as a study among college students reported the prevalence dropped sharply from 23.6% to 5.5%, showing the importance of developmental continuity. 32 International research often uses standardized interviews such as Diagnostic Interview for ADHD in Adults, version 2.0 (DIVA 2.0) or Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID) (Ramos-Quiroga), producing more accurate and consistent results. Reducing these methodological gaps is crucial to developing reliable national estimates and improving adult ADHD screening practices in India.
Clinical Profile of ADHD
Indian studies on adult ADHD have mainly focused on inattention and hyperactivity/impulsivity, with most using the ASRS v1.1 as the primary screening tool. Across community and student populations, the inattentive subtype consistently appears most common. A study reported that 62.6% of ADHD-positive college students in Delhi NCR were inattentive, 19 while similar trends were reported among college students in Chandigarh and Madhya Pradesh32,38 (Table 4). Even in studies with lower prevalence, inattentive subtypes dominated, accounting for roughly 35%-63% of cases.42,52 These results align with international findings, showing that hyperactivity declines with age while inattention remains the defining feature in adulthood. 55
Clinical Profile and Comorbidities of Adult ADHD in Indian Studies.
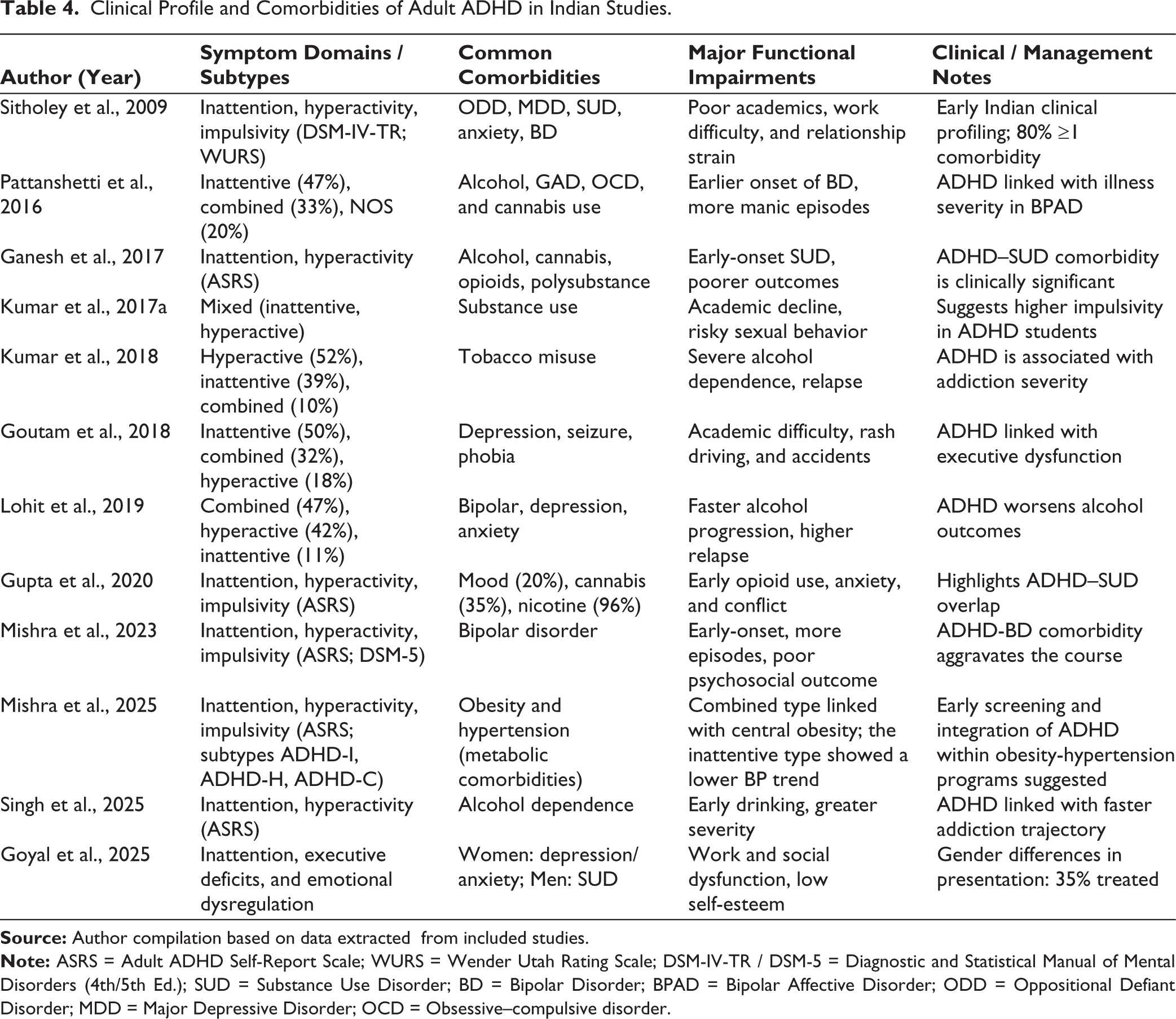
The scope of symptom evaluation extended beyond core domains in clinical samples from India. A study in Bengaluru assessed executive dysfunction, emotional dysregulation, and social cognition, showing that adults with ADHD experienced impairments beyond DSM-defined symptoms. 50 Women reported greater symptom severity and atypical features such as mind-wandering, hyper-focusing, and mood lability, while men more often showed externalizing behaviors such as substance use.50,56,57 These gender-specific patterns mirror global findings, where women are frequently underdiagnosed because internalizing symptoms are misattributed to depression, anxiety, or personality disorders.57–59 Thus, Indian evidence supports international trends while highlighting unique diagnostic barriers for women in low-resource mental health settings.
Comorbidity profiles varied substantially between community and clinical contexts. Student-based studies either did not assess psychiatric comorbidities or reported very low levels; for instance, a study among medical students reported isolated cases of depression and phobias. In contrast, hospital and psychiatric samples showed higher comorbidity, with ADHD prevalence ranging from 15% to 27%.34,47 Bipolar patients with ADHD displayed greater alcohol dependence, anxiety, OCD, and cannabis use, 34 while another study found 27% lifetime ADHD prevalence, 47 consistent with international estimates.60,61
Studies revealed a strong, persistent association of alcohol use and ADHD.62,63 A study identified mood and anxiety disorders among alcohol-dependent populations who are ADHD-positive. 40 Another study found high ADHD prevalence among alcohol-dependent inpatients, 51 with diagnoses confirmed through DSM-5 criteria, linking ADHD with earlier initiation of drinking, greater severity, and higher relapse rates. 40 Further evidence from coastal populations showed that occupational pressures and a culture of heavy alcohol consumption interacted with ADHD symptoms. 20 A comparative study between alcohol-dependent cases and healthy controls also found that ADHD exacerbated dependence severity. 36
Studies on SUDs reveal consistent associations with ADHD. One study reported high ADHD prevalence among treatment-seeking substance users in Bengaluru, particularly those with early-onset dependence. 35 Another study identified ADHD among heroin- and cannabis-dependent adults in North India, 49 while similar patterns were observed in opioid-dependent inpatients, linked to risky behaviors and poorer quality of life. 41 Research from North-East India highlighted how social acceptance of alcohol and opioids shaped the expression of ADHD. 46 These findings, consistent with the studies that emphasize India-specific factors, occupational alcohol culture 20 and stronger ADHD associations with cannabis and opioids,41,49 with consequences such as relapse, unemployment, and family strain. 46 Another study reported that nearly 80% of adults with ADHD had at least one psychiatric comorbidity, including major depression, substance use, anxiety, and oppositional defiant disorder. 31 These results align with global evidence showing that adult ADHD is rarely “pure,” often co-occurring with mood, anxiety, and SUDs.64,65 The Indian data thus mirror international patterns while highlighting the diagnostic complexity and challenges of managing multimorbid ADHD in resource-limited psychiatric settings.
In alcohol and SUD populations, the functional impact of ADHD was markedly greater. Research showed that ADHD-positive alcohol-dependent patients had earlier onset, faster progression, and more severe ICD-10 dependence features. 51 Another study found shorter abstinence, higher relapse, and severe withdrawal in comorbid cases. 40 Research also linked early-onset substance use with higher ADHD prevalence, along with greater psychosocial instability across affected groups.35,46,49 These findings, consistent with global evidence66–68 suggest sociocultural factors such as fishing- community alcohol culture 19 and regional opioid use intensify outcomes. 46
In psychiatric populations, comorbid ADHD was linked to more severe illness trajectories. A study reported that noted that ADHD-positive bipolar patients experienced earlier onset, more frequent manic episodes, and higher drug burdens compared with those without ADHD. 34 These results align with international research showing that ADHD in psychiatric populations, particularly in bipolar disorder, is associated with a more severe and chronic illness course, higher suicide risk, and poorer psychosocial outcomes.69–71 Overall, the evidence supports that ADHD functions as a risk amplifier across psychiatric contexts, aggravating functional impairments irrespective of the primary disorder.
Despite substantial evidence of burden, there was a paucity of treatment and management approaches in the Indian literature. None of the reviewed studies conducted structured intervention trials. Most articles limited themselves to recommending early screening, clinician awareness, and integration of ADHD assessment into psychiatric or addiction care pathways. One study emphasized that only 35% of women in their clinical sample received ADHD specific interventions, with most being treated instead for comorbidities, underscoring the problem of diagnostic overshadowing. 50 Contradictorily, international research provides evidence base for interventions, including stimulants and non-stimulants such as atomoxetine and guanfacine, and cognitive-behavioral therapy have all demonstrated efficacy in improving symptoms and functioning in adult ADHD.72,73 The lack of Indian intervention studies, therefore, represents a significant gap, highlighting the need for culturally adapted trials that address both psychiatric and functional outcomes.
Indian research shows that adult ADHD involves core attentional deficits, high comorbidity, and significant functional impairments, consistent with international evidence. However, higher prevalence in substance use populations suggests strong contextual influences such as migration stress, occupational drinking culture, and regional drug access. Functional impairments are prominent among students, including poor academics, low self-esteem, and risky behaviors.32,37,42 These patterns align with global findings linking ADHD to academic failure, impulsivity, and risky sexual or substance use behaviors.74,75 Yet, intervention research in India remains limited, underscoring the need for evidence-based treatments to support functional recovery.
Conclusion
Adult ADHD is increasingly recognized in India as a clinically and socially significant condition marked by persistent inattention and hyperactivity-impulsivity. Indian evidence shows wide prevalence variation, ranging from 5% to 16% in student and community populations to 18%-62% in psychiatric and substance use cohorts, reflecting methodological diversity and contextual influences. Consistent with global findings, the inattentive subtype predominates, and comorbid mood, anxiety, bipolar, and SUDs are common. Clinical studies reveal that ADHD frequently exacerbates alcohol and drug dependence, accelerates illness progression in bipolar disorder, and contributes to academic, occupational, and social dysfunction.
Distinctive to Indian research are cultural insights linking ADHD expression to migration stress, competitive academic environments, and occupational alcohol norms. However, methodological limitations persist: Most studies rely on self-report screeners without retrospective childhood confirmation or structured diagnostic interviews, and intervention research remains absent. Gender differences are rarely explored, leading to underrecognition among women.
Future research should prioritize standardized diagnostic protocols adapted to Indian contexts, gender-sensitive approaches, integration of ADHD screening into psychiatric and addiction services, and culturally informed treatment trials. Bridging these gaps is crucial to transform diagnostic awareness into effective, evidence-based care for adults with ADHD in India.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Not Applicable as this article does not report any patient data.